
Abstract
Background
Socioeconomic disadvantage is associated with shorter adult stature. Few studies have examined socioeconomic differences in stature from birth to childhood and the mechanisms involved, particularly in middle-income former Soviet settings.
Methods
The sample included 12,463 Belarusian children (73% of the original cohort) born in 1996–1997, with up to 14 stature measurements from birth to 7 years. Linear spline multi-level models with 3 knots at 3, 12 and 34 months were used to analyse birth length and growth velocity during four age-periods by parental educational achievement (up to secondary school, advanced secondary/partial university, completed university) and occupation (manual, non-manual).
Results
Girls born to the most (versus least) educated mothers were 0.43 cm (95% confidence interval (CI): 0.28, 0.58) longer at birth; for boys, the corresponding difference was 0.30 cm (95% CI: 0.15, 0.46). Similarly, children of the most educated mothers grew faster from birth-3 months and 12–34 months (p-values for trend ≤0.08), such that, by age 7 years, girls with the most (versus least) educated mothers were 1.92 cm (95% CI: 1.47, 2.36) taller; after controlling for urban/rural and East/West area of residence, this difference remained at 1.86 cm (95% CI: 1.42, 2.31), but after additionally controlling for mid-parental height, attenuated to 1.10 cm (95% CI: 0.69, 1.52). Among boys, these differences were 1.95 cm (95% CI: 1.53, 2.37), 1.89 cm (95% CI: 1.47, 2.31) and 1.16 cm (95% CI: 0.77, 1.55), respectively. Additionally controlling for breastfeeding, maternal smoking and older siblings did not substantively alter these findings. There was no evidence that the association of maternal educational attainment with growth differed in girls compared to boys (p for interaction = 0.45). Results were similar for those born to the most (versus least) educated fathers, or who had a parent with a non-manual (versus manual) occupation.
Conclusions
In Belarus, a middle-income former Soviet country, socioeconomic differences in offspring growth commence in the pre-natal period and generate up to approximately 2 cm difference in height at age 7 years. These associations are partly explained by genetic or other factors influencing parental stature.
Trial Registration
Current Controlled Trials: NCT01352247 assigned 9 Sept 2005; ClinicalTrials.gov. Identifier: NCT01561612 received 20 Mar 2012.
Similar content being viewed by others


Background
Adult attained height reflects fetal, infant and childhood growth and hence the influence of in utero and postpartum environment and genes [1, 2]. Height is an important marker of health, because shorter people have higher cardiovascular disease risk [3, 4] and higher overall mortality [5], albeit a lower risk of developing some cancers [4–6]. Socioeconomic differences in length and/or height (abbreviated to length/height) have been demonstrated at all ages and in various settings [7–14], with socioeconomic disadvantage associated with shorter stature.
In high-income populations, some cross-sectional studies have found that socioeconomic differences in height have narrowed over the generations [15], whilst others report their persistence [16]. Socioeconomic height differences have also recently been reported in contemporary low- and middle-income populations [17, 18]. Better living conditions in high-income countries may lead to improvements in childhood health, environment and social conditions [15] and may reduce adverse environmental effects, allowing genetic potential to be reached and a reduction in socioeconomic differences. Factors such as improved infant-feeding [19], reductions in maternal smoking [20, 21] and overcrowding [19] or other environmental features may affect children’s stature. Such factors are important to examine in relation to growth because they are potentially modifiable and their distribution may change across socioeconomic groups over time. In contrast, parental height reflects both environmental and genetic influences [22] on growth but is not immediately modifiable.
Few studies have examined the development of socioeconomic differences in length/height from birth through infancy to childhood using repeated measures of stature; of those that have, most have been set in high-income countries [23–26], with fewer in low- or middle-income countries, such as Brazil [18, 27] or former Soviet countries, such as Russia [28]. It is important to understand not only the magnitude and timing of the emergence of socioeconomic differences in length/height (as these may clarify important growth periods when public health interventions aimed at reducing these differences, and hence inequalities in later health outcomes, might be targeted), but also the mechanisms involved (which may suggest modifiable factors suitable for intervention). By examining socioeconomic differences in childhood growth and the factors that affect growth in a middle-income former Soviet country, we aimed to understand whether the findings are specific to this context or share similarities with those in other settings.
Belarus is a middle-income [29], former Soviet republic, with features in common with high-income countries such as high adult literacy and low child mortality rates but, in contrast to many high-income countries, low income inequality [30] and high adult mortality rates, particularly from cardiovascular disease [31]. We have previously reported that Belarusian children of the most educated parents or non-manual households were taller at age 6.5 years than those of the least educated parents or manual households [17]. Here, we extend our earlier analysis to model individual length/height trajectories from birth to 7 years by maternal and paternal educational achievement, and parental occupation, in over 12,000 children. We examine when socioeconomic differences in length/height emerge, whether they change with age, and the effect of controlling for prolonged and exclusive breastfeeding, maternal smoking, the number of older siblings and mid-parental height to shed light on potential mechanisms generating socioeconomic differences in birth size and postnatal stature.
Methods
Study design and participants
The study cohort is based on 17,046 children and their mothers who were originally recruited during their postpartum hospital stay into the Promotion of Breastfeeding Intervention Trial (PROBIT) [32] in Belarus in 1996–1997. Briefly, 31 maternity hospitals and one each of their affiliated polyclinics (outpatient clinics for routine health care) were randomly assigned, within strata of urban/rural and East/West geographical location, to participate in a breastfeeding promotion intervention or to continue with prevailing practices. Inclusion criteria specified that the mothers were healthy and initiated breastfeeding, and that the infants at birth were full-term (≥37 weeks gestation) healthy singletons, weighed at least 2,500 g at birth and had a 5-minute Apgar score ≥5. Study staff estimated that only 1-2% of eligible women declined participation in the trial [33].
Follow-up from birth to 12 months of age
During the postpartum stay, the number of other children living together in the household, parental education and occupation and maternal smoking during pregnancy were reported by the mother, and infant birth length was abstracted from medical records [34]. The number of other children in the household was categorized as 0, 1 and 2 or more and used as a proxy for older siblings and overcrowding. Educational status was recoded from seven to three categories: initial or incomplete or common secondary; advanced secondary or partial university; and completed university, with ‘unknown’ coded as missing. Each parent’s occupation was classified as manual or non-manual and the highest household occupation determined [17]. Mother’s current smoking status and infant length was recorded by study paediatricians on scheduled study visits when the infant was aged 1, 2, 3, 6, 9 and 12 months; home visits were made when polyclinic visits were missed [34]. As differences in length/height gain were not major hypotheses of PROBIT, no attempt was made to standardise the measurement of length in infancy.
Follow-up between 12 months to 6.5 years
In 2002–2005, at the age of 6.5 years (interquartile range (IQR): 6.5-6.7, range: 5.6-8.5 years), 13,889 children (81% of those randomized) were examined at a research visit by one of 38 polyclinic paediatricians who received special training in anthropometry. Standing height was measured twice by a standardised protocol, using a stadiometre with a movable headboard (Medtechnika, Pinsk, Belarus) and the average of the two measurements used [35]. An audit of the height measures for 190 children at 5.3-32.6 months (mean 17.7 months) after the initial 6.5-year research examination, showed a test-retest correlation of 0.84. The study paediatricians also retrospectively abstracted height data from the medical records of each child, as height was routinely measured and documented at check-ups between 12 months and 6.5 years. Of 12,463 children with complete data, 10,389 children had 39,205 measurements (median, 5; IQR, 4–5; range, 1–6) abstracted from medical records between the 12-month and 6.5-year examinations. The observed length/height measurements were converted to age- and sex-adjusted z-scores according to World Health Organization (WHO) Child Growth Standards 2006, using the STATA command zanthro[36].
Parental height was obtained by interview with the parent who accompanied the child at the 6.5-year follow-up visit. Any parental height that was implausible (greater than +/- 4 standard deviations (SD) from the parent-specific mean) was recoded to “missing”. Mid-parental height was calculated as the average of the two parents’ heights. Maternal current smoking status was also recorded at the 6.5-year follow-up. All occasions when maternal smoking was recorded (i.e. during pregnancy, at clinic visits during the first-year of follow-up and at 6.5 year follow-up) were recoded to yes/no from the number of cigarettes smoked per day and combined to create a longitudinal measure of ‘maternal smoking’ categorised as unknown, ever or never.
Ethics
PROBIT was approved by the Belarusian Ministry of Health and received ethical approval from the institutional review board of the Montreal Children’s Hospital for both the original PROBIT trial and the 6.5-year follow-up. The participating parent/guardian signed consent forms in Russian at each phase.
Statistical methods
Summarizing individual length/height gain trajectories
We chose the maximum age of 7 years (84 months) as our upper age cut-off, as this was the oldest age with sufficient data to describe the growth trajectory. Length/height growth velocity was predicted for each child by a linear spline multilevel model with 3 knots at 3, 12 and 34 months, the knots were chosen that best fitted the data. Full details of the model selection process have been published elsewhere [37, 38]. The knot points generated four splines, estimating different length/height growth rates between 0–3 months, 3–12 months, 12–34 months and 34–84 months; designated as ‘early infancy’, ‘late infancy’ , ‘early childhood’ and ‘late childhood’ , respectively. The model assumes piecewise linear growth and is therefore a simplification of the underlying growth process. Although a linear spline model is an approximation of the true growth function; its coefficients are easily interpretable and have been shown to produce good model fit in this and several other cohorts [18, 23, 37–40]. Furthermore, analyses in four other cohorts in different settings have resulted in similar knot points, providing some face validity that the growth periods identified represent meaningful distinct periods of growth that are similar across children from different ethnic and socioeconomic backgrounds [18, 23, 37–40]. Individual- and occasion-level residuals were approximately normally distributed. Our approach assumes that residuals are uncorrelated and that any missing outcome data are missing at random. However, even if the autocorrelation assumption is violated, the fixed effects, which we report, are likely to be unbiased [41]. The advantage of this method of growth modelling is that the model allows for the change in scale and variance of length/height over time; each child is included in the analysis; all measurements are included, regardless of when the measurements were taken (however irregularly spaced); and the actual age at measurement is taken into account. The multilevel model was fitted for three levels: i) the measurement occasion; ii) the individual child; and iii) hospital/polyclinic site where the child was examined.
The growth trajectories were modelled for all children with at least two measures of length/height (N = 16,861) and then modelled restricted to those with complete data on all covariables (N = 12,463). As findings did not differ substantively between these two datasets, we present results for those with complete data only.
Crude and multiple analysis of growth
The coefficients from the models were used to predict length/height measurements at various ages by socioeconomic position and to calculate the absolute difference between extreme categories of socioeconomic position (See Additional file 1: supplementary information). To allow comparison of length/height differences in Belarus with an international growth standard, we report the absolute difference in terms of standard deviations of the WHO Child Growth Standards [42], calculated by dividing the absolute difference (cm) by the standard deviation (cm) of the WHO reference length/height measurement of the same age and sex. As length/height variance widens with age, reporting findings as standard deviations also allows a comparison of the differences on the same relative scale.
Three multivariable multilevel models were fitted for growth trajectories by categories of socioeconomic position. Model 1 adjusted for urban/rural and East/West location as these geographical variables were used to stratify the original randomization and may confound the associations examined. Model 2 additionally adjusted for mid-parental height, a proxy for genetic and environmental factors that influenced the parents’ own growth [14, 19–21, 43–45], while model 3 also adjusted for trial intervention arm (as an unbiased measure of prolonged and exclusive breastfeeding), maternal smoking, and number of older siblings (because previous studies have shown these factors [19–21, 46–48] to be associated with both statural growth and socioeconomic position [49, 50]). These latter factors could be conceptualized as mediators, as poorer socioeconomic circumstances are associated with reduced breastfeeding [51], increased maternal smoking both pre- and postnatally [49, 50] and larger family size [19]. In addition, breastfeeding is associated with rapid linear growth in the first 3 months of life and less rapid growth to 12 months [48]. Maternal smoking, particularly during pregnancy, [20] is associated with shorter offspring stature. Ovecrowding or having older siblings may also increase the frequency of childhood infection [19], lead to a sharing of resources (both material and psychosocial [47]) and affect the childhood environment and conditions, all of which may impact growth adversely.
We included trial randomisation arm as the best assessment of the mediating effect of breastfeeding on child length/height [48]. The proportion of women who were exclusively breastfeeding was seven-fold higher in the intervention arm at 3 months compared to the control arm (43.3 vs. 6.4%) and more than 12-fold higher at 6 months (7.9 vs. 0.6%) [34]. To separate the effects of each parent’s height on socioeconomic differences in growth, we also replaced mid-parental height in the final model with either maternal or paternal height.
We found strong statistical evidence of a difference in the growth trajectory between girls and boys (p < 0.001), hence we present results for girls and boys separately. However, there was no evidence that the association between maternal education and the length/height growth trajectory differed in girls compared to boys (p for sex-interaction = 0.45). We tested the assumption of a linear relationship between categories of the socioeconomic exposures and length/height trajectory using likelihood ratio tests based on the fully adjusted models. As evidence against the assumption of linearity was weak (p = 0.13 for girls and p = 0.09 for boys) we present linear models. Because of the large quantity of data, and patterns that were similar across socioeconomic groups, we present the results for maternal education in detail and provide the results for paternal education and highest household occupation as supplementary Web Tables. Analyses were conducted in STATA version 13.1 (Stata Corporation, Texas) and using the runmlwin command [52] in MLwiN (Version 2.30) [53].
Results
Table 1 compares the 16,861 children with at least two measures of length/height to those 12,463 with complete data and reveals little difference in the proportions of each covariable between the two data sets. Those with missing data were more likely among children of mothers with no more than a secondary school education compared to those of mothers educated to advanced secondary, partial university or completed university. Those with incomplete data were slightly shorter and lighter at birth and were more likely to come from urban or Eastern areas, be in the breastfeeding promotion (intervention) arm of the trial and be first born.
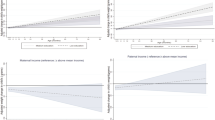
Our study sample consisted of 12,463 individuals (73% of the original cohort) with complete data on all covariables, with 133,934 measurements (median, 12; IQR, 10–13; range, 3–14). Figure 1 shows the scatterplot of length/height measurements by child’s age; each black dot represents a single data point. Additional file 1: Table S1 shows the observed lengths/heights in cm and in WHO length/height-for-age z-score, by category of maternal education. For girls aged between 6.8 and 7 years, those of the least educated mothers had a mean z-score of 0.22 (SD: 0.94), while for girls of the most educated mothers, the mean z-score was 0.61 (SD: 0.93); for boys the respective z-scores were 0.08 (SD: 0.90) and 0.64 (SD: 1.00). Predicted offspring lengths/heights per category of maternal education and age are shown in Table 2. A linear relationship across the three maternal education categories is apparent for birth length and length/height at all ages, for both girls and boys. The absolute difference in birth length between infants in the highest versus the lowest category of maternal education was 0.43 cm (95% CI: 0.28, 0.58) for girls and 0.30 cm (95% CI: 0.15, 0.46) for boys. Absolute differences in length/height between the highest versus the lowest category of maternal education increased with age, such that by age 7 years, the absolute difference was 1.92 cm (95% CI: 1.47, 2.36) among girls and 1.95 cm (95% CI: 1.53, 2.37) among boys. Table 2 also shows the absolute differences in length/height by maternal education in terms of standard deviations of WHO length/height-for-age reference; at age 7 years, this is equivalent to 0.35SD (95% CI: 0.27, 0.43) among girls and 0.37 SD (95% CI: 0.29, 0.45) among boys. The absolute SD differences in length/height between the highest versus the lowest education categories showed some widening with age. Figure 2 illustrates the absolute difference in length/height in cm, with 95% confidence interval, between the highest and lowest categories of maternal education for girls and boys.

Length/height measurements with age.

Absolute difference in length/height, cm (95% confidence interval) between highest and lowest categories of maternal education.
Table 3 shows the change in length/height rate per category of mother’s education during early infancy (birth to 3 months) was 0.31 cm/year (95% CI: -0.03, 0.65; p for trend = 0.08) for girls and 0.83 cm/year (95% CI: 0.48, 1.17; p for trend < 0.001) for boys. However, in late infancy (3–12 months) and late childhood (34–84 months) we found only weak evidence that growth rates varied between categories of maternal education for both girls and boys (all p-values for trend ≥0.25). In early childhood (12–34 months) we found strong evidence that growth rates were higher per category of mother’s education: for girls by 0.31 cm/year (95% CI: 0.18, 0.43; p for trend < 0.001); and for boys by 0.23 cm/year (95% CI: 0.11, 0.35; p for trend <0.001).
Controlling for urban/rural and East/West area of residence attenuated the association of maternal education with growth between birth and 3 months (model 1). Additionally controlling for mid-parental height (model 2), attenuated associations of birth length and length/height velocity with maternal education for all growth periods, amongst both girls and boys. However, further controlling for prolonged and exclusive breastfeeding, maternal smoking and the number of older siblings (model 3) made little difference to the results. The models were used to calculate the absolute height difference between the highest versus lowest categories of maternal education at age 7 years. For the unadjusted model, the absolute difference in height at 7 years was 1.92 cm (95% CI: 1.47, 2.36) taller among girls and 1.95 cm (95% CI: 1.53, 2.37) among boys; after controlling for urban/rural and East/West area of residence (model 1), this difference remained at 1.86 cm (95% CI: 1.42, 2.31) among girls and 1.89 cm (95% CI: 1.47, 2.31) among boys. Height differences at age 7 years attenuated by 40% after controlling for mid-parental height; the difference was 1.10 cm (95% CI: 0.69, 1.52) among girls and 1.16 cm (95% CI: 0.77, 1.55) among boys (model 2). On adjustment for prolonged and exclusive breastfeeding, maternal smoking and the number of older siblings (model 3), the difference remained [1.11 cm (95% CI: 0.69, 1.53) among girls and 1.08 cm (95% CI: 0.68, 1.47) among boys]; the fully adjusted differences in terms of WHO height-for-age standard deviations among girls was attenuated to 0.20 SD (95% CI: 0.13, 0.28) and to 0.20 SD (95% CI: 0.13, 0.28) among boys. However, even in the fully adjusted model, differences in growth between categories of maternal education persisted for birth length and growth in early childhood. Adjusting for mother’s height did not result in greater attenuation of the association of mother’s education with child’s growth trajectory compared to adjusting for father’s height (results not shown).
Findings for categories of paternal education (Additional file 1: Table S2) and highest household occupation (Additional file 1: Table S3) were similar to those for maternal education. Generally, among girls and boys, growth per category of paternal education or household occupation showed evidence of a difference in length/height growth rates in the unadjusted models at 0–3 and 12–34 months. The fully-adjusted models were used to calculate the absolute difference in height between the highest versus lowest categories of paternal education and non-manual versus manual household occupation at age 7 years; for girls, the height differences were 0.47 cm (95% CI: 0.06, 0.89) and 0.19 cm (95% CI: -0.10, 0.47), respectively; for boys, the differences were 0.15 cm (95% CI: -0.23, 0.54) and 0.42 cm (95% CI: 0.15, 0.69), respectively. The difference in terms of WHO height-for-age standard deviations among girls by paternal education was 0.09 SD (95% CI: 0.01, 0.16), and by highest household occupation was 0.03 SD (95% CI: -0.02, 0.09); the corresponding differences for boys were 0.03 SD (95% CI: -0.04, 0.10) and 0.08 SD (95% CI: 0.03, 0.13), respectively.
Discussion
Amongst over 12,000 healthy, term infants from the Republic of Belarus, a middle-income former Soviet country, children born to the most educated parents were longer at birth and grew faster in stature in early infancy and early childhood than those born to the least educated parents, with some widening of socioeconomic differences with age. Findings were similar on comparing children from households with non-manual occupations to those from households with manual occupations. After adjusting for confounders, controlling for mid-parental height moderately attenuated these associations. However, controlling for prolonged and exclusive breastfeeding, maternal smoking and older siblings did not substantially alter the associations between maternal education and growth.
The parents of the PROBIT children were born under the communist system, in which education (including universities) was universal and free. Our findings of a positive relationship between parental education or highest household occupation and length/height growth are broadly consistent with some [18, 23, 26–28, 54] but not all [24] studies in various settings. Previous studies have used different statistical methods [26–28, 54] from ours and/or alternative measures of socioeconomic position [26, 27]. Two recent papers have modelled growth trajectories using the same methods as the present study. One contemporary British cohort (Avon Longitudinal Study of Parents and Children, ALSPAC) found that birth length was shortest amongst children of the least educated women, with a small widening of differences up to 10 years of age [23]. In Southern Brazil, amongst infants born and followed for 4 years, maternal education was similarly positively associated with birth length and also positively associated with growth rates [18]. Although these studies were set in countries with different economies (the U.K. is a high- and Brazil a middle-income country), both observed that children from the most educated mothers were longer at birth-as we did in Belarus. In Brazil, children of the highest-educated mothers grew faster than the children of the lowest-educated mothers, with a widening of differences with age: from 0.2 SD of birth length to 0.7 SD of height at age 4 years. In Belarus, the difference between extreme categories of maternal education was approximately 0.2 SD at birth and 0.4 SD at age 4 years (in WHO SD). Our findings in Belarus are thus similar to those from Brazil, but a greater widening of socioeconomic differences was reported at age 4 years in Brazil.
Few studies have examined the effect of possible mediators/confounders on the association of socioeconomic position with birth length and rate of growth in children. We observed an average 40% further reduction in socioeconomic height differences after adjustment for mid-parental height, beyond the reduction due to adjustment for confounders. Using similar methods to our study and with comparable findings, the Brazilian cohort also found that adjusting for maternal height (rather than mid-parental height) attenuated socioeconomic differences in birth length and (as in our study) growth rates in early infancy and early childhood [18]. Another study from the ALSPAC cohort found the socioeconomic difference in offspring height change was attenuated after controlling for mid-parental height [54], whilst others have reported that adding maternal and paternal height with other covariables resulted in greater socioeconomic differences [24].
The mechanisms leading to socioeconomic differences in growth require further research. The literature suggests that maternal education may influence offspring length/height trajectories through the educated mother’s environment, income and behaviour, including the ability to access and utilise health care information and services during pregnancy and postnatally [55]. As described above, we found mid-parental height explained some of the socioeconomic differences in length/height trajectories. The final attained height of each parent reflects a complex combination of his or her accumulated inherited genetic material and the fetal, infant and childhood environment in which they grew up [14]. In turn, these factors may also play a part in the offspring’s growth trajectory with any genetic height potential only being reached if the environment allows. Length/height differences widen from birth to 3 months, but on adjustment for mid-parental height, the differences were reduced substantially, suggesting that parental height explains some of the differences in growth rates during this period. Height differences also widen notably between 1–3 years; while mid-parental height explains some of the difference, other factors related to socioeconomic position, such as family diet and exposure to illness/infection, may influence offspring health and hence height growth during this period. Our findings suggest that public health interventions to improve socioeconomic conditions in early childhood, such as promoting healthy diets, educating parents about improving uptake of immunisations, preventing illness/infection and seeking early medical care in case of illness might have a beneficial impact on later height and health.
We are continuing to assess growth in this cohort as the children progress through puberty and into adulthood to determine the most important periods of growth associated with adult attained height and mortality. Further studies could also determine important modifiable factors, which may suggest interventions applied at suitable ages, aimed at reducing socioeconomic differences in height. Our findings may not be generalizable to other settings, for example, our height differences were fairly modest compared to those seen in the Brazilian cohort [18], mentioned above. Further investigation of longitudinal cohorts in other middle-income populations with similar or different economic histories would add to our understanding of socioeconomic differences in childhood growth.
The main strength of the study was our large sample size with many measures of length/height over a long period; a growth modelling strategy which utilized all of the available data; analysis that was not restricted to individuals with complete data at all time points or data measured at exactly the same ages for all individuals; and allowed for the change in size and variation of length/height with age. One limitation of our study is that measurements in infancy and childhood were based on routine child health records (only measurements at the 6.5-year follow-up were standardised and audited), so associations may have been attenuated by measurement error. We are unable to assess the reliability of the routinely-collected length/height measurements in Belarus. We combined length and height measurements, even though they are measured differently. Recumbent length can be very difficult to measure accurately and tends to be longer than standing height; the difference between these two measurement methods in children aged 2–3 years can be as much as 0.47 cm [56]. We were unable to control for method of length/height measurement (whether recumbent or standing) as this was not recorded; therefore associations may be attenuated by this measurement error. The difference between the 16,861 children with at least two measures of length/height compared to those 12,463 with complete data, showed that those with missing data were more likely to have less educated mothers and more likely to be slightly shorter at birth. These differences should not, however, affect the associations we observed between socioeconomic status and growth trajectories. We found adjustment for breastfeeding (by study trial arm), maternal smoking and older siblings did not alter the association between maternal education and offspring growth substantively. This suggests that either maternal education does not mediate its effect on offspring growth through these factors, or that by controlling for a mediator we have induced another association (e.g. induced confounding) which masks the effect of the mediator.
Conclusion
In summary, despite low reported levels of income inequality [30], socioeconomic differences in length/height growth amongst children from Belarus were present at birth and widened through early infancy and early childhood. These differences were partly explained by mid-parental height, suggesting that factors influencing the parents’ growth during their own childhood have a bearing on these socioeconomic differences. Our findings suggest that public health interventions aimed at improving socioeconomic conditions in early childhood might help reduce socioeconomic differences in length/height in this setting.
References
Sorensen HT, Sabroe S, Rothman KJ, Gillman M, Steffensen FH, Fischer P, Serensen TIA: Birth Weight and Length as Predictors for Adult Height. Am J Epidemiol. 1999, 149 (8): 726-729. 10.1093/oxfordjournals.aje.a009881.
Silventoinen K, Sammalisto S, Perola M, Boomsma DI, Cornes BK, Davis C, Dunkel L, De LM, Harris JR, Hjelmborg JV, Luciano M, Martin NG, Mortensen J, Nisticò L, Pedersen NL, Skytthe A, Spector TD, Stazi MA, Willemsen G, Kaprio J: Heritability of adult body height: a comparative study of twin cohorts in eight countries. Twin Res. 2003, 6 (5): 399-408. 10.1375/136905203770326402.
D Wormser E, D Angelantonio S, Kaptoge AM, Wood P, Gao Q, Sun G, Walldius R, Selmer WMM, Verschuren HB, Bueno-de-Mesquita G, Engstrm PM, Ridker I, Njlstad H, Iso I, Holme S, Giampaoli H, Tunstall-Pedoe JM, Gaziano E, Brunner F, Kee A, Tosetto C, Meisinger H, Brenner P, Ducimetiere PH, Whincup RW, Tipping I, Ford P, Cremer A, Hofman L, The Emerging Risk Factors Collaboration, et al: Adult height and the risk of cause-specific death and vascular morbidity in 1 million people: individual participant meta-analysis. Int J Epidemiol. 2012, 41 (5): 1419-1433.
Lee CMY, Barzi F, Woodward M, Batty GD, Giles GG, Wong JW, Jamrozik K, Lam TH, Ueshima H, Kim HC, Gu DF, Schooling M, Huxley RR, Asia Pacific Cohort Studies Collaboration: Adult height and the risks of cardiovascular disease and major causes of death in the Asia-Pacific region: 21 000 deaths in 510 000 men and women. Int J Epidemiol. 2009, 38 (4): 1060-1071. 10.1093/ije/dyp150.
Davey Smith G, Hart C, Upton M, Hole D, Gillis C, Watt G, Hawthorne V: Height and risk of death among men and women: aetiological implications of associations with cardiorespiratory disease and cancer mortality. J Epidemiol Community Health. 2000, 54 (2): 97-103. 10.1136/jech.54.2.97.
Batty GD, Barzi F, Woodward M, Jamrozik K, Woo J, Kim HC, Ueshima H, Huxley RR, for the Asia Pacific Cohort Studies Collaboration: Adult height and cancer mortality in Asia: the Asia Pacific Cohort Studies Collaboration. Ann Oncol. 2010, 21 (3): 646-654. 10.1093/annonc/mdp363.
Webb E, Kuh D, Peasey A, Pajak A, Malyutina S, Kubinova R, Topor-Madry R, Denisova D, Capkova N, Marmot M, Bobak M: Childhood socioeconomic circumstances and adult height and leg length in central and eastern Europe. J Epidemiol Community Health. 2008, 62 (4): 351-357. 10.1136/jech.2006.056457.
Wadsworth MEJ, Hardy RJ, Paul AA, Marshall SF, Cole TJ: Leg and trunk length at 43 years in relation to childhood health, diet and family circumstances; evidence from the 1946 national birth cohort. Int J Epidemiol. 2002, 31 (2): 383-390. 10.1093/ije/31.2.383.
Whitley E, Gunnell D, Davey Smith G, Holly JMP, Martin RM: Childhood circumstances and anthropometry: the Boyd Orr cohort. Ann Hum Biol. 2008, 35 (5): 518-534. 10.1080/03014460802294250.
Barros AJD, Victora CG, Horta BL, Goncalves HD, Lima RC, Lynch J: Effects of socioeconomic change from birth to early adulthood on height and overweight. Int J Epidemiol. 2006, 35 (5): 1233-1238. 10.1093/ije/dyl160.
Wright CM, Parker L: Forty years on: the effect of deprivation on growth in two Newcastle birth cohorts. Int J Epidemiol. 2004, 33 (1): 147-152. 10.1093/ije/dyg187.
Turrell G: Socio-economic position and height in early adulthood. Aust N Z J Public Health. 2002, 26 (5): 468-472. 10.1111/j.1467-842X.2002.tb00349.x.
Subramanian SV, Ozaltin E, Finlay JE: Height of Nations: A Socioeconomic Analysis of Cohort Differences and Patterns among Women in 54 Low- to Middle-Income Countries. PLoS One. 2011, 6 (4): e18962-10.1371/journal.pone.0018962.
Cavelaars AE, Kunst AE, Geurts JJ, Crialesi R, Grotvedt L, Helmert U, Lahelma E, Lundberg O, Mielck A, Rasmussen NK, Regidor E, Spuhler T, Mackenbach JP: Persistent variations in average height between countries and between socio-economic groups: an overview of 10 European countries. Ann Hum Biol. 2000, 27 (4): 407-421. 10.1080/03014460050044883.
Li L, Manor O, Power C: Are inequalities in height narrowing? Comparing effects of social class on height in two generations. Arch Dis Child. 2004, 89 (11): 1018-1023. 10.1136/adc.2003.035162.
Batty GD, Leon DA: Socio-economic position and coronary heart disease risk factors in children and young people: evidence from UK epidemiological studies. Eur J Public Health. 2002, 12 (4): 263-272. 10.1093/eurpub/12.4.263.
Patel R, Lawlor DA, Kramer MS, Davey Smith G, Bogdanovich N, Matush L, Martin RM: Socioeconomic inequalities in height, leg length and trunk length among children aged 6.5 years and their parents from the Republic of Belarus: evidence from the Promotion of Breastfeeding Intervention Trial (PROBIT). Ann Hum Biol. 2011, 38 (5): 592-602. 10.3109/03014460.2011.577752.
Matijasevich A, Howe LD, Tilling K, Santos IS, Barros AJD, Lawlor DA: Maternal education inequalities in height growth rates in early childhood: 2004 Pelotas birth cohort study. Paediatr Perinat Epidemiol. 2012, 26: 236-249. 10.1111/j.1365-3016.2011.01251.x.
Silventoinen K: Determinants of variation in adult body height. J Biosoc Sci. 2003, 35 (2): 263-285. 10.1017/S0021932003002633.
Leary S, Davey Smith G, Ness A: Smoking during pregnancy and components of stature in offspring. Am J Hum Biol. 2006, 18 (4): 502-512. 10.1002/ajhb.20518.
Rona RJ, Chinn S, Florey CD: Exposure to cigarette smoking and children's growth. Int J Epidemiol. 1985, 14 (3): 402-409. 10.1093/ije/14.3.402.
Kuh D, Wadsworth M: Parental Height: Childhood Environment and Subsequent Adult Height in a National Birth Cohort. Int J Epidemiol. 1989, 18 (3): 663-668. 10.1093/ije/18.3.663.
Howe LD, Tilling K, Galobardes B, Davey Smith G, Gunnell D, Lawlor DA: Socioeconomic differences in childhood growth trajectories: at what age do height inequalities emerge?. J Epidemiol Community Health. 2012, 66 (2): 143-148. 10.1136/jech.2010.113068.
Silva LM, van Rossem L, Jansen PW, Hokken-Koelega ACS, Moll HA, Hofman A, Mackenbach JP, Jaddoe VWV, Raat H: Children of Low Socioeconomic Status Show Accelerated Linear Growth in Early Childhood; Results from the Generation R Study. PLoS One. 2012, 7 (5): e37356-10.1371/journal.pone.0037356.
Smith AM, Chinn S, Rona RJ: Social factors and height gain of primary schoolchildren in England and Scotland. Ann Hum Biol. 1980, 7 (2): 115-124. 10.1080/03014468000004131.
Li L, Manor O, Power C: Early environment and child-to-adult growth trajectories in the 1958 British birth cohort. Am J Clin Nutr. 2004, 80 (1): 185-192.
Lourenco B, Villamor E, Augusto R, Cardoso M: Determinants of linear growth from infancy to school-aged years: a population-based follow-up study in urban Amazonian children. BMC Public Health. 2012, 12 (1): 265-10.1186/1471-2458-12-265.
Grjibovski AM, Bygren LO, Yngve A, Sjostrom M: Social variations in infant growth performance in Severodvinsk, Northwest Russia: community-based cohort study. Croat Med J. 2004, 45 (6): 757-763.
World Bank: http://data.worldbank.org/ (accessed 15/04/2013)
Pan American Health Organization: Measuring health inequalities: Gini coefficient and concentration index. Epidemiol Bull. 2001, 22 (1): 3-4.
World Health Organization, Noncommunicable diseases and mental health: 2010, http://www.who.int/nmh/countries/blr_en.pdf (last accessed 4/9/2013)
Kramer MS, Chalmers B, Hodnett ED, Sevkovskaya Z, Dzikovich I, Shapiro S, Collet JP, Vanilovich I, Mezen I, Ducruet T, Shishko G, Zubovich V, Mknuik D, Gluchanina E, Dombrovsky V, Ustinovitch A, Ko T, Bogdanovich N, Ovchinikova L, Helsing E: Promotion of breastfeeding intervention trial (PROBIT): a cluster-randomized trial in the Republic of Belarus. Design, follow-up, and data validation. Adv Exp Med Biol. 2000, 478: 327-345.
Patel R, Oken E, Bogdanovich N, Matush L, Sevkovskaya Z, Chalmers B, Hodnett ED, Vilchuck K, Kramer MS, Martin RM: Cohort Profile: The Promotion of Breastfeeding Intervention Trial (PROBIT). Int J Epidemiol. 2014, 43 (3): 679-690. 10.1093/ije/dyt003. first published online March 2013 doi:2010.1093/ije/dyt2003
Kramer MS, Chalmers B, Hodnett ED, Sevkovskaya Z, Dzikovich I, Shapiro S, Collet JP, Vanilovich I, Mezen I, Ducruet T, Shishko G, Zubovich V, Mknuik D, Gluchanina E, Dombrovskiy V, Ustinovitch A, Kot T, Bogdanovich N, Ovchinikova L, Helsing E, PROBIT Study Group (Promotion of Breastfeeding Intervention Trial): Promotion of Breastfeeding Intervention Trial (PROBIT): a randomized trial in the Republic of Belarus. JAMA. 2001, 285 (4): 413-420. 10.1001/jama.285.4.413.
Kramer MS, Matush L, Vanilovich I, Platt RW, Bogdanovich N, Sevkovskaya Z, Dzikovich I, Shishko G, Collet JP, Martin RM, Davey Smith G, Gillman MW, Chalmers B, Hodnett E, Shapiro S, PROBIT Study Group: Effects of prolonged and exclusive breastfeeding on child height, weight, adiposity, and blood pressure at age 6.5 y: evidence from a large randomized trial. Am J Clin Nutr. 2007, 86 (6): 1717-1721.
Vidmar SI, Cole TJ, Pan H: Standardizing anthropometric measures in children and adolescents with functions for egen: Update. Stata Journal. 2013, 13 (2): 366-378.
Tilling K, Davies NM, Nicoli E, Ben-Shlomo Y, Kramer MS, Patel R, Oken E, Martin RM: Associations of growth trajectories in infancy and early childhood with later childhood outcomes. Am J Clin Nutr. 2011, 94 (6 Suppl): 1808S-1813S.
Howe LD, Tilling K, Matijasevich A, Petherick ES, Santos AC, Fairley L, Wright J, Santos IS, Barros AJD, Martin RM, Kramer MS, Bogdanovich N, Matush L, Barros H, Lawlor DA: Linear spline multilevel models for summarising childhood growth trajectories: A guide to their application using examples from five birth cohorts. Stat Methods Med Res. 2013, doi:10.1177/0962280213503925
Anderson EL, Fraser A, Martin RM, Kramer MS, Oken E, Patel R, Tilling K: Associations of postnatal growth with asthma and atopy: the PROBIT Study. Pediatr Allergy Immunol. 2013, 24 (2): 122-130. 10.1111/pai.12049.
Fairley L, Petherick ES, Howe LD, Tilling K, Cameron N, Lawlor DA, West J, Wright J: Describing differences in weight and length growth trajectories between white and Pakistani infants in the UK: analysis of the Born in Bradford birth cohort study using multilevel linear spline models. Arch Dis Child. 2013, 98 (4): 274-279. 10.1136/archdischild-2012-302778.
Taylor JM, Cumberland W, Sy J: A stochastic model for analysis of longitudinal AIDS data. J Am Stat Assoc. 1994, 89 (427): 727-736. 10.1080/01621459.1994.10476806.
The World Health Organisation Child Growth Standards. 2014, http://www.who.int/childgrowth/standards/en/ (accessed 16/6/2014)
Merchant KM, Villar , Kestler E: Maternal height and newborn size relative to risk of intrapartum caesarean delivery and perinatal distress. BJOG. 2001, 108 (7): 689-696.
Judge TA, Cable DM: The effect of physical height on workplace success and income: preliminary test of a theoretical model. J Appl Psychol. 2004, 89 (3): 428-441.
Voss LD, Mulligan J, Betts PR: Short stature at school entry–an index of social deprivation? (The Wessex Growth Study). Child Care Health Dev. 1998, 24 (2): 145-156. 10.1046/j.1365-2214.1998.00051.x.
Li L, Power C: Influences on childhood height: comparing two generations in the 1958 British birth cohort. Int J Epidemiol. 2004, 33 (6): 1320-1328. 10.1093/ije/dyh325.
Lawson DW, Mace R: Sibling configuration and childhood growth in contemporary British families. Int J Epidemiol. 2008, 37 (6): 1408-1421. 10.1093/ije/dyn116.
Kramer MS, Guo T, Platt RW, Shapiro S, Collet JP, Chalmers B, Hodnett E, Sevkovskaya Z, Dzikovich I, Vanilovich I, PROBIT Study Group: Breastfeeding and infant growth: biology or bias?. Pediatrics. 2002, 110 (2 Pt 1): 343-347.
Lynch JW, Kaplan GA, Salonen JT: Why do poor people behave poorly? Variation in adult health behaviours and psychosocial characteristics by stages of the socioeconomic lifecourse. Soc Sci Med. 1997, 44 (6): 809-819. 10.1016/S0277-9536(96)00191-8.
Mohsin M, Bauman AE: Socio-demographic factors associated with smoking and smoking cessation among 426,344 pregnant women in New South Wales, Australia. BMC Public Health. 2005, 5: 138-10.1186/1471-2458-5-138.
Yang S, Platt RW, Dahhou M, Kramer MS: Do population-based interventions widen or narrow socioeconomic inequalities? The case of breastfeeding promotion. Int J Epidemiol. 2014, 43 (4): 1284-1292. 10.1093/ije/dyu051.
Leckie G, Charlton C: runmlwin - A Program to Run the MLwiN Multilevel Modelling Software from within Stata. J Stat Softw. 2013, 52 (11): 1-40.
Rasbash J, Charlton C, Browne WJ, Healy M, Cameron B: MLwiN Version 2.30. 2014, Bristol, UK: Centre for Multilevel Modelling, University of Bristol
Galobardes B, McCormack VA, McCarron P, Howe LD, Lynch J, Lawlor DA, Davey Smith G: Social Inequalities in Height: Persisting Differences Today Depend upon Height of the Parents. PLoS One. 2012, 7 (1): e29118-10.1371/journal.pone.0029118.
Thomas D, Strauss J, Henriques M-H: How Does Mother's Education Affect Child Height?. J Hum Resour. 1991, 26 (2): 183-211. 10.2307/145920.
Buyken AE, Hahn S, Kroke A: Differences between recumbent length and stature measurement in groups of 2- and 3-y-old children and its relevance for the use of European body mass index references. Int J Obes (Lond). 2005, 29 (1): 24-28. 10.1038/sj.ijo.0802738.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2458/14/932/prepub
Acknowledgements
We are grateful to the cohort members and their parents for their generous participation in the study, to the maternity hospital staff and polyclinic paediatricians who examined all the children and ensured a very high follow-up rate, and to the dedication of the members of the Belarusian team who ensured that this trial could start and who continue to support and guide the study through all stages of PROBIT. Funding: Supported by a grant from the Canadian Institutes of Health Research (to MSK) and from the European Union's project on Early Nutrition Programming: Long-term Efficacy and Safety Trials (grant code: FOOD-DT-2005-007036 to RMM). RMM, KT, DAL & LDH work in a Unit that receives funding from the UK Medical Research Council (Grant code: MC_UU_12013/5 and MC_UU_12013/9). DALs contribution to this work is supported by a Wellcome Trust grant (grant code: WT094529MA). LDH is funded by a UK Medical Research Council Population Health Scientist award (G1002375). The NIHR Bristol Nutrition Biomedical Research Unit is funded by the National Institute for Health Research (NIHR) and is a partnership between University Hospitals Bristol NHS Foundation Trust and the University of Bristol. None of the funding bodies influenced the data collection, analysis or its interpretation for this paper. The views expressed are those of the authors and not necessarily any funding body.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interest.
Authors’ contributions
The hypotheses were developed by RP, RMM and DAL; RP performed the statistical analysis, wrote the first draft, and co-coordinated completion of the paper; KT, LDH and EN developed the multilevel models; NB and LM coordinated fieldwork. RP had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. All authors critically commented on, edited earlier drafts, and approved the final version of the paper.
Electronic supplementary material
12889_2013_7090_MOESM1_ESM.docx
Additional file 1: Table S1: Observed mean length/height measurements (cm) and mean World Health Organization (WHO) child growth standards z-score by sex, age, and maternal education. Table S2. Crude & multiple analysis of mean growth rate per category of paternal education, N = 12,203 Table S3. Crude & multiple analysis of growth rate in manual versus non-manual highest household occupation, N = 11,761. Supplementary information. (DOCX 43 KB)
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Patel, R., Tilling, K., Lawlor, D.A. et al. Socioeconomic differences in childhood length/height trajectories in a middle-income country: a cohort study. BMC Public Health 14, 932 (2014). https://doi.org/10.1186/1471-2458-14-932
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2458-14-932