
Abstract
Background
The present study assessed coverage, changes in condom use, and prevalence of HIV and other STIs among high-risk men who have sex with men (HR-MSM; highly visible, recruited from cruising sites/sex venues) and transgender (TG; male-to-female transgender persons, also called hijras) in the Indian state of Maharashtra.
Methods
Data from Avahan’s computerized management information system; two rounds of integrated behavioral and biological assessment (IBBA) surveys (Round 1 with 653 HR-MSM/TG and Round 2 with 652 HR-MSM/TG); and project-supported condom social marketing was used for the present analysis. Logistic regression models were used to assess changes in key indicators over these two rounds and to explore the association between exposure to Avahan interventions and condom use and STI prevalence in HR-MSM/TG.
Results
By December 2007, Avahan had reached about 90% of the estimated HR-MSM/TG population, and 83% of the estimated total population had visited STI clinics by March 2009. Free direct condom distribution by Avahan program NGOs and social marketing outlets in Maharashtra increased from about 2.7 million condoms in 2004 to 15.4 million in 2008. HR-MSM/TG were more likely to report higher consistent condom use (adjusted odds ratio [AOR]: 1.90; 95% confidence interval [CI] 1.01-3.58) with regular male partners (spouse/lover/boyfriend) in Round 2 of IBBA, compared to Round 1. HR-MSM/TG exposed to Avahan interventions were more likely to report consistent condom use with regular male partners (AOR: 2.46; CI 1.34-4.52) than those who were unexposed. Prevalence of reactive syphilis serology declined significantly from 8.8% in Round 1 to 1.1% in Round 2 (p = 0.001), while the observed change HIV prevalence (12.3% to 6.3%, p = 0.16) was insignificant.
Conclusion
The current evaluation provides evidence for successful scale up and coverage of target population by Avahan interventions in Maharashtra. The assessment findings showed improved accessibility to condoms and reduced risk behaviours with male sexual partners. Syphilis prevalence declined; however HIV prevalence did not change and is still a major concern. Continued strengthening of core programmatic strategies are needed to effectively improve condom use with all partner types and to help bring sustained reductions in HIV risk in HR-MSM/TG and its onward transmission.
Similar content being viewed by others

Background
An estimated 2.47 million people were living with HIV in India in 2008 [1]. HIV epidemic in India has been concentrated among female sex workers (FSWs); men who have sex with men (MSM), including transgender (TG) persons; and injecting drug users (IDUs) [2]. Though the epidemic in India is largely due to heterosexual transmission, studies across the country have shown that sexual activity between men is relatively common [3–6] and HIV among MSM/TG populations is increasingly becoming an important route of transmission [2]. In India male-to-male sexual behavior takes place in diverse contexts, and MSM are known to have multiple partners, use condoms selectively during anal sex with male and female partners, and have high consumption of alcohol and drugs [4, 5, 7–12]. Social stigma and clandestine behavior add to the vulnerability of MSM/TG, making them an important target group for HIV prevention interventions. Estimated HIV prevalence in MSM/TG in India stood at 4.4% in 2010–2011, down from 7.4% in 2007. However, HIV prevalence in Maharashtra (9.91%) is much higher than the national average, and in 2007, Maharashtra (11.8%) had the second largest burden of the HIV infected in India [13, 14]. Most studies have consistently found HIV prevalence in MSM/TG to be higher than 5% in Maharashtra. Notably, studies have shown that MSM/TG in the country’s metropolitan cities, such as Mumbai, Chennai, Pune, and Bangalore show higher HIV prevalence [4, 10, 11, 15, 16].
The country’s National AIDS Control Organisation (NACO) has, since 1992, implemented targeted interventions for high-risk groups such as FSWs and men attending STI clinics. Maharashtra was among the first states in India to initiate targeted interventions for MSM [17]. Avahan: the India AIDS Initiative, funded by the Bill & Melinda Gates Foundation, was launched in 2003 with the aim of reducing the spread of HIV; it has since played a major role in supporting prevention interventions in the country [18]. Avahan worked in 83 districts of the country’s six high-HIV prevalence states among high-risk groups. One of these six states was the western state of Maharashtra, where Avahan covered 15 districts out of the total 35 districts; in eight of these districts Avahan was the sole provider of interventions (Table 1). Avahan’s strategies were designed to achieve high coverage (80% of the total estimated target population) through delivery of a package of proven prevention services that would address proximal and distal determinants of HIV risk [19, 20]. The key elements of the combination prevention program for HR-MSM/TG included peer-led outreach to promote behavior change, clinical services to treat STIs, provision of commodities (condoms and lubricants) for safe sex, support for community mobilization, and advocacy to reduce structural barriers to safer sexual practices [17]. Avahan’s intervention focus was on highly visible HR-MSM/TG in high-risk locations (cruising sites/sex venues, such as parks, local train stations, and bus stops), who tend to have a large number of sexual partners and regularly practice receptive anal sex or sell sex. They are therefore referred to as high-risk MSM [17]. The present analysis, using multiple data sources, was conducted to assess the overall effect of the Avahan program on HIV prevention in Maharashtra’s HR-MSM/TG population. The specific objectives of this paper are to examine the scale-up and coverage of the Avahan program, changes in condom use patterns and prevalence of HIV and other STIs, and the association between these outcomes and exposure to Avahan program among HR-MSM/TG in Maharashtra.
Methods
The Avahan program evaluation framework was adapted and used for this assessment (Table 2) [21]. We evaluated the impact of the program using this framework, based on the program logic model, and using data from two rounds of independent surveys and program monitoring data. The framework assesses the program in the following sequence: (1) program implementation fidelity to design (process and output indicators); (2) intermediate outcomes such as condom use and STIs in target populations, HIV prevalence in target population and general population; (3) role of high-risk interventions in any changes; and (4) Avahan’s contribution to these changes.
A. Data sources
Data from three sources were used in this analysis to build evidence to assess the effect of Avahan on key programmatic outcomes: Avahan’s computerized management information system (CMIS), two rounds of cross-section surveys among HR-MSM/TG, called the Integrated Behavioral and Biological Assessment (IBBA); and program-supported condom social marketing data [22–24].
CMIS
Avahan’s CMIS [24, 25] provided data on program inputs, infrastructure, outreach, clinical service utilization, and community mobilization. This data were generated at the implementing organization level (local NGOs) and submitted to Avahan’s central CMIS by state-level lead implementing partners (LIPs). It was consolidated at district, LIP, state, and pan-Avahan levels. The consolidated monthly data from January 2005 through March 2009 for the 15 districts of Maharashtra was used to assess trends in coverage and uptake of program services. The coverage indicators included whether a high-risk group member was ever contacted by peer educators and had ever visited a program STI clinic. Avahan’s target for saturated coverage (defined as providing services to at least 80% of the estimated total population) in selected districts/catchment areas, assessed through participatory mapping and site assessment, was the benchmark against which the adequacy of coverage was assessed. The estimated size of the HR-MSM/TG population as of March 2009 (10,240) was used as the denominator for analysis. The service indicators examined were monthly peer contacts and quarterly clinic visits against Avahan’s established targets [outreach: one contact per month; clinic visits: once per quarter). Measures of program intensity included ratio of program staff (peers and outreach workers) to target population (against a target of 1:50 HR-MSM/TG) [see Table 2 for additional indicator details]. Detailed description of CMIS indicators and estimation process is available elsewhere [24].
IBBA
The IBBA surveys were conducted to measure the major outcomes and impact of HIV interventions supported by Avahan, the India initiative. In IBBA, HR-MSM/TG were operationally defined as men identified at cruising points, aged 18 years and older, who had had any type of sex (oral, anal, manual) with another man in the past month. Two rounds of cross-sectional IBBA surveys were conducted among HR-MSM/TG in three districts of Maharashtra — Mumbai, Thane and Pune, chosen purposively based on the overall study design of IBBA. The respondents were selected using the time location cluster sampling method [23]. Mumbai and Thane are neighboring districts, but for the purposes of the survey they were considered one domain due to high mobility of individuals between the two districts. Field work was conducted during January–April 2007 (Round 1) and in December 2009 (Round 2). Information on demographics, sexual behaviors, condom use, and exposure to intervention was collected in these surveys through a questionnaire. The participants were also tested for presence of STIs, including HIV. Written informed consent was obtained from respondents before administration of questionnaire and collection of sample for biological tests. The field work was conducted by research agencies under the guidance and supervision of National AIDS Research Institute (NARI), and FHI 360 (trade name for Family Health International) provided the technical support. Further details of the methodology are available elsewhere [23, 26–28] and additional IBBA-related information can also be accessed at http://www.ibbainfo.in. Data collection for IBBA was approved by the Protection of Human Subjects Committee (of FHI 360) and the ethical committee of NARI, an Indian Council of Medical Research (ICMR) institute.
Condom social marketing data
Annual condom sales data from Avahan-supported condom social marketing program [22] in Maharashtra (2005–2008) was used to assess condom distribution by the project and gaps in condom availability.
B. Exposure and outcome variables
Four process and output indicators were assessed to inform the Avahan evaluation framework described above. These indicators were: (1) scale-up and intensity (programs reach and coverage) of Avahan coverage among HR-MSM/TG in Maharashtra; (2) reported consistent condom use; (3) prevalence of STIs, including HIV; and (4) associations between intermediate outcomes (condom use, prevalence of HIV/STIs) and exposure to the Avahan program (peer contacts, visits to NGO clinics and condom provision) [see Table 2 for indicator details].
Condom use
Self-reported condom use from the two rounds of IBBA was analyzed to assess changes in condom use patterns. Consistent condom use was defined as condom use during every act of anal intercourse with different types of male partners (such as, main regular male partners [lover/boyfriend/spouse], paying male partners [receiving cash or gifts when selling sex], paid male partners [giving cash or gifts to male partner or hijra when buying sex], and other casual male partners).
Sexually transmitted infections and HIV
Blood and urine samples were tested for STIs. Syphilis serology was done using rapid plasma reagin (RPR; by Span Diagnostics Ltd.) and confirmed by Treponema pallidum hemagglutination assay (TPHA; by Syphagen). Nucleic acid amplification (Gen-Probe APTIMA COMBO 2 – Gen-Probe Inc. San Diego, California) tests on urine samples were done for chlamydia and gonorrhoea. HIV positivity was determined by a serial testing algorithm using two rapid tests (Microlisa-IV by J. Mitra & Co. Pvt. Ltd. and Genedia HIV ½ ELISA 3.0 by Greencross Life Sciences) [23].
Program exposure
Avahan exposed the HR-MSM/TG to a combination of prevention interventions. Therefore, a composite indicator of selected intervention exposure — ever been exposed to any three core program services: contact by Avahan peer educators, visit to a Avahan program clinic, and provision of condoms from peer educator — was created and used for this analysis. We estimated the association between this composite indicator and consistent condom use with different male partners and STIs (including HIV).
C. Data management and statistical analysis
Data from the two districts was combined and appropriate weights calculated and used for IBBA data analyses. All the analyses were performed in SPSS Version 15.01 (®IBM, New York). The proportions for categorical variables, means and 95% confidence intervals (CIs) for continuous variables were calculated. The difference between the proportions was tested using the Pearson chi-square test.
Logistic regression models were used to measure the association between exposure and outcome variables. We initially estimated the unadjusted associations between exposure and outcomes. Following this, we built multivariate models and adjusted for background characteristics and contextual variables related to geographical coverage that could confound results, such as district of interview, self-reported sexual identity, current age, literacy, place of residence, sex outside place of residence, and main source of income.
-
1.
The first set of logistic regression models estimated the association between consistent condom use and STIs (including HIV) as outcomes and the round of IBBA data collection as the primary explanatory variables.
-
2.
The next set of logistic models estimated the association between consistent condom use and STIs as outcomes and composite exposure to core program services of the Avahan intervention as explanatory variable.
-
3.
For the third set of logistic regression models, we pooled data from both rounds of IBBA and evaluated the association between exposure to the intervention and condom use. Thereafter, these were analysed separately for rounds 1 and 2 of IBBA for consistent condom use (as an outcome) with different types of male partners. We compared the odds ratios in these two rounds of IBBA using the methods described by Altman and Bland [29].
Results
A total of 1,305 HR-MSM/TG (653 in Round 1 and 652 in Round 2) were sampled. The mean age of HR-MSM/TG in Round 1 and Round 2 was 25.7 years (95% CI: 24.7 – 26.7) and 24.2 years (95% CI: 23.7 – 24.8), respectively (p = 0.001). HR-MSM/TG were more likely to be literate (96.4% vs. 89.4%, p = 0.01) and live locally (83.2% vs. 65.7%, p = 0.02) in Round 2 than in Round 1. Though HR-MSM/TG were less likely to report having had a paid male partner in Round 2 compared with Round 1 (8.6% vs. 29.9%, p = 0.001), they were more likely to have a non-commercial male/male-to-female transgender partner (71.9% vs. 51.3%, p = 0.001). HR-MSM/TG were less likely to report sex outside the place of current residence in Round 2 compared with Round 1 (33.3%vs. 23.2%, p = 0.04). HR-MSM/TG were more likely to identify themselves as bisexual (33.6% vs. 6.6%) and significantly fewer as panthi (locally used term for a male partner who mainly penetrates) in Round 2 compared with Round 1 (15.4% vs. 43.3%, p < 0.001). Select demographic characteristics, sexual behaviors, condom use, and exposure to the Avahan intervention in both rounds of IBBA are presented in Table 3.
Scale-up of Avahan program
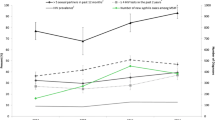
The Avahan program for HR-MSM/TG in Maharashtra began in late 2004 in three districts and scaled up to 15 districts by 2008 through 20 local implementing NGOs working under state LIPs. The CMIS data in December 2005 indicated that 22% of the estimated HR-MSM/TG had ever been contacted; however, scale-up increased this coverage to 90% by December 2007 and continued to increase consistently until March 2009. Those HR-MSM/TG who had ever visited STI clinics increased from 20% in mid-2006 to 83% in March 2009 (Figure 1a). The proportion of HR-MSM/TG contacted monthly by peer educators increased from 10% in early 2006 to about 79% in March 2009, and monthly STI clinic visits increased from 1% to 24% during the same period (Figure 1b). There was a considerable increase in the mean frequency of visits by HR-MSM/TG to STI clinics from 2005 (mean: 1.0) to 2009 (mean 3.9). About 42% of HR-MSM/TG reported four or more clinic visits in 2009 (Figure 1c).The number of active paid peer educators was low in the initial stages of the program (13 peer educators in mid-2005) but increased as the program was scaled up (192 by March 2009). Similarly, the number of outreach workers increased from 77 in early 2005 to 167 in March 2009 (Figure 1d). The ratio of HR-MSM/TG to peer educators was not optimal during the initial years but stabilized to a level of 1:53 by March 2009 (Figure 1d).

Scale and coverage of different components of the Avahan programme in high-risk men who have sex with men and transgendered persons (HR-MSM/TG) Maharashtra, India 2005-2009. a) Exposure to Avahan program; b) Monthly contact by program staff and visit to the STI clinic; c) Frequency of visits to Avahan STI clinic; d) Peer educators / Outreach workers from Avahan districts.
Free direct condom distribution by Avahan program NGOs in Maharashtra increased from about 0.37 million condoms in 2005 to 1.8 million in 2008. During the same period, condoms distributed by Avahan-supported social marketing outlets in program districts increased from more than 2.6 million in 2004 to about 14.4 million in 2008. The monthly ratio of free condoms distributed directly to HR-MSM/TG covered by the program increased from two condoms per HR-MSM/TG per month in 2005 to 15 per HR-MSM/TG per month in 2008.
Condom use
The HR-MSM/TG were significantly more likely to report last time (last instance of) condom use (adjusted odds ratio [AOR]: 5.15; confidence interval [CI] 2.68-9.90) as well as consistent condom use (AOR: 1.90; CI 1.01-3.58) with regular male partners in Round 2 of the IBBA than in Round 1. Similarly, HR-MSM/TG were more likely to report condom use during last sex act with a paying partner in Round 2 of IBBA than in Round 1 (AOR: 13.23; CI 2.84-61.92). Although in univariate analysis HR-MSM/TG were less likely to use condoms during last sex act with a paid male/hijra partner in Round 2 compared with Round 1, this difference was not significant (AOR: 0.91; CI 0.27-3.10) after adjustment for potential confounders. Consistent condom use with a regular female partner was low in both rounds of IBBA (33.6% in Round 1 and 25.2% in Round 2, p = 0.39). Information on condom use with different types of male partners is presented in Tables 3 and 4.
Furthermore, HR-MSM/TG who were exposed to various components of the Avahan intervention were significantly more likely to report consistent condom use with regular male partners (AOR: 2.46; CI 1.34-4.52), non-commercial male/hijra partners (AOR: 3.41; CI 1.56-7.50), and paid male/hijra partners (AOR: 3.15; CI 1.37-7.25), compared to those who had not been exposed to the intervention (Table 5).
STIs
Overall, prevalence of reactive syphilis serology declined from 8.8% in Round 1 of IBBA to 1.1% in Round 2 (p = 0.001); a similar decline was also observed in high-titre syphilis (3.8% in Round 1 vs. 0.2% in Round 2). Prevalence of urethral chlamydial (3.7% in Round 1 vs. 1.1% in Round 2) and gonococcal infection (0.3% in Round 1 vs. 0.0% in Round 2), was low in Round 1 and reduced further in Round 2; no cases of urethral gonorrhoea were reported in Round 2. The observed change in HIV prevalence was not statistically significant (12.3% in Round 1 vs. 6.3% in Round 2, p = 0.16).
In terms of district-wise data, prevalence of syphilis declined in Pune from 14.6% to 5.0% (p = 0.001) as did HIV prevalence, from 17.4% in Round 1 to 8.2% in Round 2 (p = 0.01). Similarly, in the combined domain of Mumbai and Thane, prevalence of syphilis reduced from 6.5% in Round 1 to 0.5% in Round 2 (p = 0.001). However, the observed change in HIV prevalence in Mumbai-Thane was not statistically significant (10.2% in Round 1 vs. 6.0% in Round 2, p = 0.36).
Discussion
This paper is the first to present findings from a large-scale assessment of HR-MSM/TG in Maharashtra, following Avahan’s HIV-prevention interventions. The Avahan intervention was able to achieve the targeted 80% coverage of the HR-MSM/TG population in Maharashtra. The effect of this exposure to prevention interventions was evident in the target group. A significantly higher proportion of HR-MSM/TG reported attending the STI clinic in 2009, compared to 2006. Self-reported consistent condom use with regular male partners was significantly higher in 2009 than in 2006. HR-MSM/TG who were exposed to the Avahan intervention were more likely to report consistent condom use with various types of male partners than those who were not exposed to the intervention. Prevalence of reactive syphilis serology reduced significantly in 2009 compared with 2006; however HIV prevalence did not change over time.
The findings suggest that Avahan was successful in accessing the HR-MSM/TG population in selected districts, increasing the number of outreach workers and peer-led contacts with HR-MSM/TG, improving outreach, and increasing the distribution and access of condoms for this group. It is important to mention here that not only were these targets achieved but they were also sustained for the duration. A higher than 100 percent coverage, as reflected in the CMIS data, may likely be due to the highly mobile nature of the population; the denominator was fixed to the estimated population in March 2009 whereas the numerator (members of population) was cumulative, reflecting individual HR-MSM/TG contacted over the course of the intervention (this included members who are currently present or who may have been present at an earlier time but subsequently left the area). Similar high coverage was observed among FSWs in Avahan implementation districts of Maharashtra [30]. Indeed, in Andhra Pradesh a similar successful scale-up of the HR-MSM/TG intervention has also been reported [31]. In both these scenarios, the target reached was much higher than the global average of 31% outreach documented for low and middle-income countries [32]. However, we would like to state here that Avahan attempted to cover the visible MSM, who are presumably at a high risk and reachable; the percent coverage may thus be higher than the global percentage. Nonetheless, the high coverage in this group is important given the fact that targeted interventions had started as late as 1999–2000 among the MSM population in Maharashtra.
In addition to the improved infrastructure for HIV prevention for HR-MSM/TG, changes in risk behaviors are also evident. Study findings reveal that HR-MSM/TG reported higher condom use during the last sex act with a regular and paying male partner in the second round of IBBA. Furthermore, HR-MSM/TG who were exposed to the Avahan intervention were more likely to report consistent condom use with a regular male partner. The increased availability of condoms during the same period supports this finding. Although condom use during sex may be dependent on factors other than accessibility (such as negotiation and breakage), access to condoms does form an important component of HIV interventions [33]. However, decline in both condom use with paid partners during last sex and consistent condom use was observed; similarly, consistent condom use with female partners was low in both rounds of IBBA. An important risk factor associated with unprotected sex was mobility of the individual; MSM who were mobile were more likely to report unprotected sex with male partners compared with non-mobile MSM [34]. Thus, further analysis and studies are needed to better understand the factors affecting HR MSM’ and TGs’ condom use patterns with different partners, which would help HIV prevention programs develop more effective behavior change communication strategies. Low condom use with female partners, reported by other studies as well [4, 11], is an important area of concern for HIV prevention programs working with MSM/TG. Given that a sizable proportion of the MSM population has female partners, low condom use has significant implications for HIV transmission to general population [11]; HIV prevention programs must therefore take this into consideration when planning targeted interventions. Decline in condom use with paid partners could have been due to non-usage of condoms by kothis (locally used term for self-identified MSM who are generally feminine and receptive partners during anal sex) and bisexuals, who were the majority in Round 2. Also, bisexuals are usually difficult to identify and not covered by prevention programs. Thus, future programs targeting risk reduction should be more tailored to the local dynamics of MSM/TG, cover all MSM irrespective of their sexual identities, and be sensitive and culturally acceptable.
Another important finding was the reduction in syphilis prevalence over the three years’ duration. Focussed STI-prevention measures and proper management of STIs through dedicated clinics may have led to this decline in prevalence. Improved access to STI clinics is important for HIV prevention since prompt treatment of ulcerative and non-ulcerative STIs are useful in reducing the transmission of HIV in this high-risk group [35, 36]. Furthermore, STI clinics serve as an entry point for counselling, behavioral change, and health care access in general. A recent study also reported that a structured intervention (which included risk reduction counselling and self-acceptance among MSM) has also been useful in reduction of incident bacterial STIs [37]. Thus, this entry point becomes particularly relevant for marginalized populations like MSM/TG, who may have poor health care access due to stigma and discrimination [33, 38].
While, the HIV prevalence remained unchanged, the estimated prevalence among HR-MSM/TG reported here is lower than that reported by earlier studies [10, 15, 39] and the data is comparable to national HIV surveillance (2008–09) [40]. In one of the earliest reports (mid-1990s), Nandi and co-workers found HIV prevalence to be 21% in a sample of MSM in Mumbai [39]. Several factors influence HIV prevalence and it is a short period of time between the two IBBA surveys to plausibly associate any change in HIV following programmatic interventions.
Nonetheless, the present study does have a number of limitations. The first round of IBBA was conducted one year after the initiation of the Avahan intervention and therefore not a true baseline. Avahan’s evaluation design did not include a control group, given the ethical considerations to be applied for large-scale public health programs. However, the used evaluation framework did follow program logic, and data from multiple sources (both program monitoring and independent survey data) was used to suggest plausible evidences for the effectiveness of the intervention, as alternative to randomised controlled trials, which are now considered less suitable for large public health interventions [41–44]. Although Avahan was a pan-Maharashtra intervention, the IBBA surveys were restricted to three districts; while the CMIS data shows the scale up and coverage of the program across all districts, the IBBS data provides outcomes in a sample of districts, providing confidence on validity of the monitoring data. Another limitation in IBBA was that gonorrhoea and chlamydia were tested based on urethral samples, as rectal samples could not be collected in the given field conditions. Other studies from India, where throat or rectal swabs were collected, prevalence of oropharyngeal and rectal gonorrhoea was 4.7% and 7.4%, respectively [45]. Other limitations include those applicable to cross-sectional studies. For example, there were changes in population profile over the two rounds of the survey; however, these were accounted for by controlling for changes in multivariate models. Social desirability bias for self-reported behaviors (such as condom use) is a limitation, but it was presumed that such bias was similar for both rounds of IBBA.
In spite of these limitations, this assessment has several strengths. It is one of the first assessments of a large public health intervention for HR-MSM/TG in Maharashtra. The analysis was based on Avahan’s evaluation framework and evidence presented along the program logic model, examining a sequence of infrastructure, intermediate outcomes (behavior change and STIs), and the role of the intervention in these changes, thereby providing congruency of expected trends.
Conclusions
The Avahan program in Maharashtra for HR-MSM/TG was successfully scaled up to achieve its targets through outreach, condom distribution and STI clinical services. The current evaluation shows that Avahan program effectively covered the target group, improved accessibility to condoms and reduced risk behaviours with male sexual partners. Syphilis prevalence declined; however HIV prevalence did not change and therefore a major concern. However, the evaluation also suggests that additional tailored and innovative behaviour change interventions are required to increase condom use behaviours with all types of partners, so as to reduce risk among HR-MSM/TG. Continued strengthening of core programmatic strategies will help bring sustained reductions in HIV risk in HR-MSM/TG and check its onward transmission.
Abbreviations
- HIV:
-
Human immunodeficiency virus
- STI:
-
Sexually transmitted infection
- HR-MSM/TG:
-
High-risk men who have sex with men and transgender
- FSW:
-
Female sex worker
- IDU:
-
Injecting drug user
- NACO:
-
National AIDS Control Organisation
- CMIS:
-
Computerized management information system
- IBBA:
-
Integrated behavioral and biological assessment
- NGO:
-
Non-governmental organization
- LIP:
-
Lead implementing partners
- NARI:
-
National AIDS Research Institute
- PHSC:
-
Protection of Human Subjects Committee
- ICMR:
-
Indian Council of Medical Research.
References
Country Progress Report India. 2008, [http://data.unaids.org/pub/Report/2008/india_2008_country_progress_report_en.pdf]
National AIDS Control Organisation: Annual Report 2011-12. 2013, New Delhi, India: Department of AIDS Control, Ministry of Health and Family Welfare
Chandrasekaran P, Dallabetta G, Loo V, Rao S, Gayle H, Alexander A: Containing HIV/AIDS in India: the unfinished agenda. Lancet Infect Dis. 2006, 6 (8): 508-521.
Dandona L, Dandona R, Gutierrez JP, Kumar GA, McPherson S, Bertozzi SM: Sex behaviour of men who have sex with men and risk of HIV in Andhra Pradesh, India. AIDS. 2005, 19 (6): 611-619.
Hernandez AL, Lindan CP, Mathur M, Ekstrand M, Madhivanan P, Stein ES, Gregorich S, Kundu S, Gogate A, Jerajani HR: Sexual behavior among men who have sex with women, men, and Hijras in Mumbai, India–multiple sexual risks. AIDS Behav. 2006, 10 (4 Suppl): S5-S16.
Solomon SS, Srikrishnan AK, Sifakis F, Mehta SH, Vasudevan CK, Balakrishnan P, Mayer KH, Solomon S, Celentano DD: The emerging HIV epidemic among men who have sex with men in Tamil Nadu, India: geographic diffusion and bisexual concurrency. AIDS Behav. 2010, 14 (5): 1001-1010.
Dandona R, Dandona L, Radhakrishnan S, Kumar GA, Gutiérrez JP, Asci FPPT, Alliance REU, SM B: Barriers to Condom use for Anal Sex among Men Who have Sex with Men in Andhra Pradesh, India: WeOrC1332. The XV International AIDS Conference: Oral Abstract Session. 2004, Bangkok
Mimiaga MJ, Thomas B, Mayer KH, Reisner SL, Menon S, Swaminathan S, Periyasamy M, Johnson CV, Safren SA: Alcohol use and HIV sexual risk among MSM in Chennai, India. Int J STD AIDS. 2011, 22 (3): 121-125.
Setia MS, Brassard P, Jerajani HR, Bharat S, Gogate A, Kumta S, Row-Kavi A, Anand V, Boivin JF: Men who have sex with men in India: a systematic review of the literature. J LGBT Health Res. 2008, 4 (2–3): 51-70.
Setia MS, Lindan C, Jerajani HR, Kumta S, Ekstrand M, Mathur M, Gogate A, Kavi AR, Anand V, Klausner JD: Men who have sex with men and transgenders in Mumbai, India: an emerging risk group for STIs and HIV. Indian J Dermatol Venereol Leprol. 2006, 72 (6): 425-431.
Setia MS, Sivasubramanian M, Anand V, Row-Kavi A, Jerajani HR: Married men who have sex with men: the bridge to HIV prevention in Mumbai, India. Int J Public Health. 2010, 55 (6): 687-691.
World Health Organization: HIV/AIDS among Men Who have Sex with Men and Transgender Populations in South-East Asia: The Current Situation and National Responses. 2010, Geneva: WHO, 1-149.
National AIDS Control Organisation: HIV Sentinel Surveillance 2010-11: A Technical Brief. Edited by: Department of AIDS Control MoHFW, Government of India. 2012, New Delhi
HIV Sentinel Surveillance and HIV Estimation. 2007, [http://naco.gov.in/upload/Publication/M&E%20Surveillance,%20Research/HIV%20Sentinel%20Surveillance%20and%20HIV%20Estimation%202007_A%20Technical%20Brief.pdf], : A Technical Brief
Gupta A, Mehta S, Godbole SV, Sahay S, Walshe L, Reynolds SJ, Ghate M, Gangakhedkar RR, Divekar AD, Risbud AR, Mehendale SM, Bollinger RC: Same-sex behavior and high rates of HIV among men attending sexually transmitted infection clinics in Pune, India (1993-2002). J Acquir Immune Defic Syndr. 2006, 43 (4): 483-490.
Annual Report. 2009, [http://www.performance.gov.in/sites/default/files/departments/aids-control/Annual%20Report%202009-10.pdf], -10
Bill & Melinda Gates Foundation: Breaking through Barriers: Avahan’s Scale-Up of HIV Prevention among High-Risk MSM and Transgenders in India. 2010, New Delhi: Bill & Melinda Gates Foundation
Bill & Melinda Gates Foundation: Avahan - The India AIDS Initiative: The business of HIV prevention at scale. 2008, New Delhi, India: Bill & Melinda Gates Foundation
Bill & Melinda Gates Foundation: Avahan Common Minimum Program for HIV Prevention in India. 2010, New Delhi: Bill & Melinda Gates Foundation
Boerma JT, Weir SS: Integrating demographic and epidemiological approaches to research on HIV/AIDS: the proximate-determinants framework. J Infect Dis. 2005, 191 (Suppl 1): S61-S67.
Chandrasekaran P, Dallabetta G, Loo V, Mills S, Saidel T, Adhikary R, Alary M, Lowndes CM, Boily MC, Moore J: Evaluation design for large-scale HIV prevention programmes: the case of Avahan, the India AIDS initiative. AIDS. 2008, 22 (Suppl 5): S1-S15.
Piot B, Mukherjee A, Navin D, Krishnan N, Bhardwaj A, Sharma V, Marjara P: Lot quality assurance sampling for monitoring coverage and quality of a targeted condom social marketing programme in traditional and non-traditional outlets in India. Sex Transm Infect. 2010, 86 (Suppl 1): i56-i61.
Saidel T, Adhikary R, Mainkar M, Dale J, Loo V, Rahman M, Ramesh BM, Paranjape RS: Baseline integrated behavioural and biological assessment among most at-risk populations in six high-prevalence states of India: design and implementation challenges. AIDS. 2008, 22 (Suppl 5): S17-S34.
Verma R, Shekhar A, Khobragade S, Adhikary R, George B, Ramesh BM, Ranebennur V, Mondal S, Patra RK, Srinivasan S, Vijayaraman A, Paul SR, Bohidar N: Scale-up and coverage of Avahan: a large-scale HIV-prevention programme among female sex workers and men who have sex with men in four Indian states. Sex Transm Infect. 2010, 86 (Suppl 1): i76-i82.
Bill & Melinda Gates Foundation: Use it or Lose it: How Avahan Used Data to Shape its HIV Prevention Efforts in India. 2008, New Delhi
Indian Council of Medical Research & Family Health International: National Interim Summary Report – India (October 2007), Integrated Behavioral and Biological Assessment (IBBA) -Round I: 2005–2007. 2007, New Delhi: Indian Council of Medical Research & Family Health International
Indian Council of Medical Research & Family Health International: National Summary Report – India (July 2011) Integrated Behavioral and Biological Assessment (IBBA) – Round 2: 2009–2010. 2011, New Delhi: Indian Council of Medical Research & Family Health International
Ramesh BM, Moses S, Washington R, Isac S, Mohapatra B, Mahagaonkar SB, Adhikary R, Brahmam GN, Paranjape RS, Subramanian T, Blanchard JF: Determinants of HIV prevalence among female sex workers in four south Indian states: analysis of cross-sectional surveys in twenty-three districts. AIDS. 2008, 22 (Suppl 5): S35-S44.
Altman DG, Bland JM: Interaction revisited: the difference between two estimates. BMJ. 2003, 326 (7382): 219-
Mainkar MM, Pardeshi DB, Dale J, Deshpande S, Khazi S, Gautam A, Goswami P, Adhikary R, Ramanathan S, George B, Paranjape RS: argeted interventions of the Avahan program and their association with intermediate outcomes among female sex workers in Maharashtra, India. BMC Public Health. 2011, 29: 1471-2458. (Electronic)
Goswami P, Rachakulla HK, Ramakrishnan L, Mathew S, Ramanathan S, George B, Adhikary R, Kodavalla V, Rajkumar H, Paranjape RS, Brahmam GNV: An assessment of a large-scale HIV prevention programme for high-risk men who have sex with men and transgenders in Andhra Pradesh, India: using data from routine programme monitoring and repeated cross-sectional surveys. BMJ Open. 2013, 3 (4): doi:10.1136/bmjopen-2012-002183
Adam PC, de Wit JB, Toskin I, Mathers BM, Nashkhoev M, Zablotska I, Lyerla R, Rugg D: Estimating levels of HIV testing, HIV prevention coverage, HIV knowledge, and condom use among men who have sex with men (MSM) in low-income and middle-income countries. J Acquir Immune Defic Syndr. 2009, 52 (Suppl 2): S143-S151.
Sullivan PS, Carballo-Dieguez A, Coates T, Goodreau SM, McGowan I, Sanders EJ, Smith A, Goswami P, Sanchez J: Successes and challenges of HIV prevention in men who have sex with men. Lancet. 2012, 380 (9839): 388-399.
Ramesh S, Mehrotra P, Mahapatra B, Ganju D, Nagarajan K, Saggurti N: The effect of mobility on sexual risk behaviour and HIV infection: a cross-sectional study of men who have sex with men in southern India. Sex Transm Infect. 2014, doi:10.1136/sextrans-2013-051350 [Epub ahead of print]
Gilson L, Mkanje R, Grosskurth H, Mosha F, Picard J, Gavyole A, Todd J, Mayaud P, Swai R, Fransen L, Mabey D, Mills A, Hayes R: Cost-effectiveness of improved treatment services for sexually transmitted diseases in preventing HIV-1 infection in Mwanza Region, Tanzania. Lancet. 1997, 350 (9094): 1805-1809.
Mayaud P, Mosha F, Todd J, Balira R, Mgara J, West B, Rusizoka M, Mwijarubi E, Gabone R, Gavyole A, Grosskurth H, Hayes R, Mabey D: Improved treatment services significantly reduce the prevalence of sexually transmitted diseases in rural Tanzania: results of a randomized controlled trial. AIDS. 1997, 11 (15): 1873-1880.
Safren SA, Thomas BE, Mayer KH, Biello KB, Mani J, Rajagandhi V, Periyasamy M, Swaminathan S, Mimiaga MJ: A Pilot RCT of an Intervention to Reduce HIV Sexual Risk and Increase Self-acceptance Among MSM in Chennai, India. AIDS Behav. 2014, [Epub ahead of print]
Beyrer C, Sullivan PS, Sanchez J, Dowdy D, Altman D, Trapence G, Collins C, Katabira E, Kazatchkine M, Sidibe M, Mayer KH: A call to action for comprehensive HIV services for men who have sex with men. Lancet. 2012, 380 (9839): 424-438.
Nandi J, Kamat H, Bhavalkar V, Banerjee K: Detection of human immunodeficiency virus antibody among homosexual men from Bombay. Sex Transm Dis. 1994, 21 (4): 235-236.
National Institute of Health and Family Welfare & National AIDS Control Organisation: Annual HIV Sentinel Surveillance: Country Report 2008–09. 2011, New Delhi: Ministry of Health & Family Welfare
Bennett S, Boerma JT, Brugha R: Scaling up HIV/AIDS evaluation. Lancet. 2006, 367 (9504): 79-82.
Bryce J, Victora CG: Ten methodological lessons from the multi-country evaluation of integrated Management of Childhood Illness. Health Policy Plan. 2005, 20 (Suppl 1): i94-i105.
Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M: Developing and evaluating complex interventions: the new medical research council guidance. BMJ. 2008, 337: a1655-
Pettifor AE, MacPhail C, Bertozzi S, Rees HV: Challenge of evaluating a national HIV prevention programme: the case of loveLife, South Africa. Sex Transm Infect. 2007, 83 (Suppl 1): i70-i74.
National AIDS Control Organisation: National AIDS Control Programme III: Report on Mid-Term Review of Sexually Transmitted Infection Services. 2009, New Delhi
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2458/14/784/prepub
Acknowledgements
The authors wish to thank the Maharashtra State AIDS Control Society, Avahan’s state implementation partners, and NGOs in the respective districts for their co-operation in implementing IBBA. We thank Dr. Maninder Setia and Ms. Kavita Sharma for reviewing and editing the manuscript. We also thank Guy Morineau from FHI 360, Asia Pacific Regional Office, Bangkok, Thailand, for his inputs in finalization of the manuscript. Finally, we extend our thanks to the MSM and TG community for their participation in the study.
Disclaimer
This research was funded by the Bill & Melinda Gates Foundation. The views expressed herein are those of the authors and do not necessarily reflect the official policy or position of the Bill & Melinda Gates Foundation.
Data sources
IBBA data are available to outside investigators through application.
See website
http://www.nari-icmr.res.in/pdf/IBBA/Agreement-for-accessing-raw-IBBA%20_R1-&-R2_data.pdf. Other IBBA related documents are available at http://www.ibbainfo.in.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
SR, SD, AG and LR contributed to the conception, design, writing and finalization of the manuscript. PG contributed in data analysis and interpretation, while MM was the key person who coordinated the study and contributed to concept development and analysis. DP was involved in the data collection and provided insights from field work. RP, BG and RA contributed to framework design, review and finalization of the manuscript. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Ramanathan, S., Deshpande, S., Gautam, A. et al. Increase in condom use and decline in prevalence of sexually transmitted infections among high-risk men who have sex with men and transgender persons in Maharashtra, India: Avahan, the India AIDS Initiative. BMC Public Health 14, 784 (2014). https://doi.org/10.1186/1471-2458-14-784
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2458-14-784