
Abstract
Background
The success of adherence to combination antiretroviral therapy (ART) in sub-Saharan Africa is hampered by factors that are unique to this setting. Home based interventions have been identified as possible strategies for decentralizing ART care and improving access and adherence to ART. There is need for evidence at individual- or community-level of the benefits of home-based interventions in improving HIV suppression in African patients receiving ART.
Methods
We conducted a systematic review and meta-analysis of the literature to assess the effect of home-based interventions on virologic outcomes in adults receiving ART in Africa.
Results
A total of 260 publications were identified by the search strategy, 249 were excluded on initial screening and 11 on full review, leaving 5 publications for analysis. The overall OR of virologic suppression at 12 months after starting ART of home-based interventions to standard of care was 1.13 (95% CI: 0.51–2.52).
Conclusions
There was insufficient data to know whether there is a difference in HIV suppression at 12 months in the home-based arm compared with the standard of care arm in adults receiving ART in Africa. Given the few trials conducted from Africa, there is need for further research that measures the effects of home-based models on HIV suppression in African populations.
Similar content being viewed by others


Background
Successful HIV treatment programmes depend largely on adherence of patients to combination antiretroviral treatment (ART). Several studies have demonstrated that adherence to ART is an important predictor of viral suppression [1–4], antiretroviral resistance [1, 5, 6], progression to AIDS [1], and death [7, 8]. However, there are still challenges of improving adherence to ART in Africa [9]. Home based interventions have been identified as possible strategies of decentralizing ART care and promoting task shifting to improve access and adherence to ART. In this meta-analysis we searched for randomised trials from Africa that used home-based strategies to improve virologic outcomes in patients receiving ART to provide evidence on the feasibility of using this intervention on African populations. The reason for choosing studies from Africa is that unlike developed countries, the success of adherence to ART in sub-Saharan Africa is hampered by factors that are unique to this setting. The magnitude of HIV-related complications is becoming too great for existing clinic infrastructures in Africa. Most public health facilities in sub-Saharan Africa rely on self-presentation of patients to the ART clinic for group counselling on ART adherence and collection of monthly stocks of antiretroviral drugs (ARVs). This strategy risks failing because amidst the rapid scale-up of ART there are severe shortages of suitably skilled health professionals in public health facilities [10].
Existing systematic reviews and meta-analyses on home-based interventions [11] and directly observed therapy for ART [12, 13] have few studies from Africa. There are significant new data from trials in Africa on which to update these reviews. We perform a meta-analysis on the effect of home-based interventions on virologic outcomes in adults receiving ART in Africa.
Methods
Eligibility criteria
Articles were restricted to English language and included in this meta-analysis if they:
-
1.
were randomised controlled trials (RCT) or cluster randomised trials (CRT) of patients receiving ART, because these are considered the gold standard for assessing the effects of an intervention;
-
2.
included virologic outcomes, and
-
3.
reported on home-based interventions in Africa that used either family or lay and/or professional people to provide all forms of treatment, care or support in the HIV-infected person’s home, as compared with hospital or health facility-based care; even though (i) patients still had to visit the clinic from time to time and (ii) the clinic remained responsible for the prescription of anti-retroviral regimen and changing the therapy.
Search methods for identification of studies
The following data sources were searched in May 2010, September 2011 and the search repeated in December 2012 for updates: PubMed/Medline from 2001 to 2012 and EMBASE from 2001 to 2012. Additional studies not indexed in PubMed/Medline and EMBASE were searched from abstracts presented at the Conference on Retroviruses and opportunistic Infections (CROI) from 2001 to 2012 and the International AIDS Society/International AIDS (IAS/AIDS) conferences from 2000 to 2012. Also, cross references were searched from the published systematic reviews and meta-analyses discussed above.
The syntax and search terms were adapted from the “Cochrane Highly Sensitive Search Strategy for identifying randomised trials in PubMed/Medline: sensitivity-maximizing version (2008 revision)” filter [14]. The search terms for detecting randomised studies in EMBASE were adapted from Wong and colleagues’ “Best specificity terms” [15] (Table 1).
Data collection and analysis
Selection of studies
Search results were merged using EndNote X3 (Thomson Reuters, TX, USA) reference manager, and duplicate records removed. The titles and abstracts of the articles were then examined and reports that were not randomised studies and those that were not relevant were removed. Full-texts that were potentially relevant were then examined for compliance with eligibility criteria. Studies that did not meet the inclusion criteria were excluded; the remaining studies were included and data collection done. Information obtained for each study included:
-
1.
Study design (RCT or CRT)
-
2.
The setting (primary or tertiary level of care) and type of intervention (including frequency and duration of the intervention) vs. the standard care at the clinic.
-
3.
The sample size of each trial
-
4.
Characteristics of the trial participants (including mean age distribution, gender and marital status)
-
5.
Virologic outcomes.
Data extraction and management
The data was extracted following the search terms. The outcome of interest for this meta-analysis was HIV suppression (dichotomous outcome) in adult Africans at 12 months after starting ART. Summary data was collected for each intervention group in a study and entered in STATA version 11 (STATA corp., Texas, USA).
Assessment of risk of bias in included studies
The risk of bias (methodological quality) of the extracted studies was assessed using the Cochrane Collaboration’s ‘Risk of bias’ tool [14]. This checks whether the trials reported on sequence generation, allocation of concealment, blinding, incomplete outcome data of patients lost to follow-up (i.e., missing at follow-up as equal to virologic failure) and other biases. The following were considered as other biases: (i) recruitment bias; (ii) baseline imbalances. In addition, the following were assessed in CRTs (iii) loss of clusters; and (iv) incorrect analysis; and comparability with individually randomised trials [14]. In CRTs, individual patient assignment of the intervention was assumed to be by the allocation of the intervention to the cluster in which the individuals resided. A ‘Risk of bias’ graph was then produced using RevMan version 5.0 (Copenhagen: The Nordic Cochrane Centre, the Cochrane Collaboration, 2008).
Measures of treatment effect and unit of analysis
The measure of effect is the odds ratio (OR) of HIV suppression in the home-based to the health facility-based group. If the data in the articles was measured using rate ratios, the rate ratio was used to estimate the OR [16]. In order to combine the effects of RCT and CRT, the OR of HIV suppression and the 95% confidence interval (CI) were used to calculate the log odds ratio (loge OR) and its standard error (SE (logeOR)). Because the unit of allocation in CRTs is a cluster, the cluster-adjusted risk ratio and rate ratios from each CRT were used as estimates of cluster-adjusted OR and the loge OR and the SE (loge OR).
Assessment of heterogeneity
The between-study heterogeneity variance of the loge ORs, tau-squared (I2), was used to measure heterogeneity between trials. An I2 ≥ 30% and χ2 p-value < 0.10 were used test for evidence of heterogeneity [14]. Also, a visual check of confidence intervals of individual studies (depicted by horizontal lines on the forest plot) was used; if the confidence intervals poorly overlapped, this would indicate presence of heterogeneity.
Assessment of reporting biases
A ‘funnel plot’ of standard error vs. effect size estimate of the intervention on virologic suppression was created to visually assess for asymmetry as an indication of publication bias.
Data synthesis
The loge OR and SE (loge OR) for the RCTs and CRTs were combined using the inverse-variance method for meta-analysis in metan (STATA corp. version 11, Texas, USA) to produce a forest plot. An OR > 1 indicated HIV suppression favouring the home-based group. All P-values were two sided; at 5% significance level (except in the testing for heterogeneity where a χ2 p-value of 10% was used as discussed above).
Sensitivity analyses
As a priori, a sensitivity analysis was going to be performed only when there was evidence of heterogeneity between studies. The sensitivity analysis would be performed by including and excluding studies based on indicators in the Cochrane Collaboration’s ‘Risk of bias’ tool listed above of reporting (i) sequence generation, (ii) allocation of concealment, (iii) blinding, (iv) incomplete outcome data of patients lost to follow-up (i.e., missing at follow-up as equal to virologic failure) and (v) other biases.
Results
Description of studies
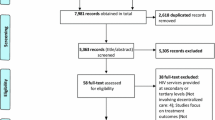
There were 260 articles identified after using the two search methods described above. These 260 articles included the trials from Africa identified in the earlier meta-analyses stated above. Out of these 260 articles, 249 were excluded after screening by title and abstract. The remaining 11 articles were assessed for eligibility by reading through the full-text; 5 articles were found to meet the inclusion criteria for this meta-analysis (Figure 1).

Flow of articles selected for meta-analysis; adapted from the PRISMA statement. CROI, Conference on Retroviruses and Opportunistic Infections. IAS, International AIDS Society/International AIDS Conference on HIV Pathogenesis, Treatment and Prevention. *Matovu, 2011 [17]. **Konate, [18]; Gusdal, [19]; Igumbor, [20]; Nglazi, [21]; Kipp, [22]; Wouters, [23]; Wouters, [24]; Shacham, [25]; Idoko, [26]; Nachega, [27]; Weidle, [28]. ‡ Naidoo, [29]. § Lester, [30]; Sarna, [31]; Fairall, [32]; Naidoo, [29]. † Stubbs, [33]; Pearson, [34].
Characteristics of included studies
Five randomised trials were included; three were RCTs [17, 35, 36] and two CRTs [37, 38] (Table 2). One study was conducted in a Prevention of Mother to Child Transmission of HIV (PMTCT) programme with women only who were attending ante-natal clinic while the rest of the studies included men and women. All five trials reported on the effect of a home-based intervention on virologic outcomes in adults at 12 months (48 weeks) of starting ART. The duration of the studies ranged from 12 months to 36 months. The number of participants analysed in each study ranged from 85 to 1 212. The combined sample size of patients analysed was 2 688; 1 614 patients were in the intervention (home-based) arm and 1 074 patients in the control (standard- , facility-, clinic-based) arm.
Risk of bias in included studies
The methodological qualities of the included trials were assessed using the ‘Risk of bias’ tool (Table 3). One study reported on blinding of study personnel, though this was only restricted to the study pharmacist. It is not clear in the four other studies whether laboratory personnel measuring the viral load outcomes were blinded. Three studies excluded missing data from the analysis of virologic outcomes. Two studies were not free of other problems that could put them at risk of bias (trial terminated early and contamination).
The study by Matovu and colleagues showed the highest risk of bias because it failed to meet most of the criteria, including lack of information on adequate allocation of concealment and blinding of outcome assessment. It also showed high risk of bias on blinding of participants and personnel; incomplete outcome data of patients lost to follow-up was excluded from the analysis, and ‘other biases’ of baseline imbalance in viral loads between the intervention groups (Figure 2).

Summary of risk of bias: judgement on each included study.
The proportion of studies with each of the judgements (‘Yes’, ‘No’, ‘Unclear’) for each entry in the ‘Risk of bias’ tool were examined (Figure 3). The risk of bias in the included studies was highest from lack of blinding of participants and study personnel, and lowest from adequate random sequence generation and free of selective reporting.

Graph of risk of bias: judgement about each risk of bias item presented as percentages across all included studies.
Effect of intervention
The overall OR at 12 months of starting ART of home-based to standard-based care was 1.13 (95% CI: 0.51 to 2.52, p = 0.757) (Figure 4).

Odds ratios of home-based to health facility-based HIV care of HIV suppression. The trials were arranged according to study design; CRT, cluster randomized trial; RCT, Randomized controlled trial.
The I2 showed no heterogeneity between trials (I2 = 0.0%, p = 0.998). Therefore no sensitivity analyses were performed to assess differences in the studies.
Detecting publication bias
A funnel plot was used to ascertain publication bias (Figure 5). The plot was symmetrical indicating the absence of publication bias. The effect of the small study by Matovu and colleagues [17] is at the bottom of the graph showing a wide spread, while the effect of the larger study by Jaffar and colleagues [37] is at the top of the graph showing a narrow spread (increased precision). The effects of all five studies are close to the true intervention odds ratio of 1.13.

Funnel plot of five randomised trials comparing home-based interventions with health facility-based care in Africa. The vertical line in the funnel plot represents the fixed effects summary estimate (using inverse-variance weighting), while the sloping lines represents the expected 95% confidence intervals for a given standard error (assuming no heterogeneity between studies).
No statistical tests for funnel plot asymmetry were performed because at least 10 studies are required to be included in the meta-analysis for these tests to be performed. When there are few studies, the power of the tests is too low to distinguish chance from real asymmetry [14].
Discussion
Summary of results
Neither superiority nor non-inferiority of the home-based interventions compared with standard of care has been clearly demonstrated with existing interventions to date. Based on the overall 95% confidence interval in this meta-analysis, it is conceivable that the effect of the home-based care does lead to an almost 2-fold worse outcome of unsuppressed HIV (OR 0.51) or that it is a lot better than the clinic-based care (OR 2.52) - but this meta-analysis is underpowered (by the few studies included) to demonstrate superiority of the home-based over the clinic-based care model. In addition, the home-based model in practice depends on clinic-based activities (including laboratory tests, monitoring of drug toxities and changing of ART regimen). Despite one study (by Jaffar and colleagues) being an equivalence trial, another (by Matovu and colleagues) being a non-inferiority trial and the other three being superiority trials, this did not affect the overall result (i.e. no evidence of heterogeneity).
Overall completeness and applicability of evidence
The studies included in this meta-analysis were conducted in sub-Saharan countries; where the challenge of shortages of health workers and increased demand for care at the clinic is apparent. Home-based interventions for ART may still have the potential of complementing existing health facility-based care in reducing the burden of HIV care. Home based interventions can potentially be delivered with minimum laboratory tests at the clinic. This is substantiated by a randomised non-inferiority trial conducted in Uganda and Zimbabwe that demonstrated that ART can still be delivered safely without routine laboratory monitoring at the clinic of toxic ART effects [41].
However, for home-based interventions to be successfully rolled out in an African setting, there would still be need for long-term management of HIV patients using culturally acceptable approaches that promote adherence to ART; that can also be easily integrated into public health models of ART care [42]. As demonstrated by Chang and colleagues in 2009 and 2010 [38, 43] and recently by Arem and colleagues in 2011 [40], this can be achieved through training of HIV patients (nominated by fellow patients) to provide HIV care in homes. Consequently, this may provide long-term benefits of adherence to ART and retention in care [37].
Jaffar and colleagues in 2009 demonstrated that the costs of health services for ART care is similar in the home-based intervention and the health facility-based group (US$793 in the home-based intervention group and US$838 in the health facility-based group) [37]. However, for the home-based intervention to be sustainable, there is need for ongoing support, training and consistent remuneration for the home-based workers from existing health systems [44].
Quality of the evidence
Only five trials were found to have met the study inclusion criteria and the combined sample size analysed was 2 688. Each study was assessed for its methodological limitation. The study by Matovu and colleagues [17] showed the highest risk of bias due to failure of this study to meet most of the criteria in the ‘Risk of bias’ assessments.
Two [35, 36] of the five studies included used intention-to-treat analyses with losses to follow-up treated as virologic failures. Like most prospective studies, losses-to-follow-up can be a source of selection bias; as it is not known what the true outcome of those lost to follow-up is i.e. whether they died as a result failing treatment or as a result of another competing cause of death or were still alive at the end of follow-up but moved out of study site and were thus not available for measuring the outcome at the end of the study. With such losses to follow-up it was hard to ascertain with certainty what the true outcomes were at study completion for the patients in these trials. For example, in the trial by Taiwo and colleagues, 14 out of 248 in the home-based group and 34 out of 251 in the health facility-based group were not found at the end of the study and were treated as failures [36]. These 14 losses in the home-based group and 34 in health facility-based group might have influenced the results differently in the Taiwo and colleagues’ study. Also, after an evaluation of the CRT by Chang and colleagues [38], Arem and colleagues [40] contended that direct and indirect contamination in the health facility-based arm could have reduced the ability of the CRT to detect home-based intervention effects, and may explain why no differences were seen in early virologic outcomes between arms or in cumulative risk of virologic outcomes. Direct contamination occurred when some patients in the health facility-based arm started volunteering to take up tasks that were similar to those of the peer health workers in the home-based intervention arm. Indirect contamination occurred through task shifting which resulted in overall gains in the quality of the ART program during the study period [40].
Potential biases in the review process
The search for studies was performed in MEDLINE and EMBASE. Additional articles were identified from abstracts presented at the CROI and IAS conferences. It is likely that all relevant articles from Africa were identified and that there are few randomised studies that have been conducted in Africa on the effect of home-based interventions on virologic outcomes in patients receiving ART.
Agreements and disagreements with other studies or reviews
The meta-analysis by Ford and colleagues [12] also found a lack of effect of the directly observed ART intervention; the risk ratio was 1.04 (95% CI: 0.91 to 1.20). As noted by Hart and colleagues [13] this effect estimate in the study by Ford and colleagues was smaller than their finding of RCTs despite also not being significant; risk ratio 1.18 (95% CI: 0.99 to 1.42). This was also the case in this meta-analysis where we found the overall risk OR to be higher than that of Ford and colleagues’, though with wider 95% confidence intervals; risk OR 1.13 (95% CI: 0.51 to 2.52). The reason for this difference may be that Ford and colleagues included estimates from the post intervention period; during which the efficacy of the intervention may have waned [13], unlike in this meta-analysis where the duration considered for the analysis was shorter .i.e., 12 months from starting ART. If the effects of directly observed ART intervention are not durable .i.e., once people graduate from the directly observed ART intervention there is no benefit on adherence to ART, there may be need for directly observed ART interventions that are repetitive [45, 46] or ongoing [47].
Conclusions
There was insufficient data to know whether there is a difference in HIV suppression at 12 months in the home-based arm compared with the standard care arm in adults receiving ART in Africa. However, given the high shortages of health workers in public health facilities in Africa, home-based interventions for ART, in addition to other approaches that have been proven to be effective such as use of mobile phone short message service [30, 48] and use of “buddies” to provide adherence support [49], may complement existing health facility-based care in reducing the burden of care. By task shifting HIV care to peer workers in the community that visit, provide ARVs and witness the dosing of ARVs, adherence can be promoted and this would not lead to poorer virologic response to ART in African settings.
Despite a thorough literature search, only five studies were identified to have met the inclusion criteria in this meta-analysis. This shows that there are few randomized trials on home-based interventions on HIV suppression that have been conducted and reported in Africa. There is need for further research in Africa that measures the effects of home-based models on HIV suppression at population level.
References
Bangsberg DR, Hecht FM, Charlebois ED: Adherence to Protease inhibitors, HIV-1 viral load, and development of drug resistance in an indigent population. AIDS. 2000, 14: 357-366. 10.1097/00002030-200003100-00008.
Paterson DL, Swindells S, Mohr J: Aherence to protease inhibitor therapy and outcomes in patients with HIV infection. Ann Intern Med. 2000, 133: 21-30.
Arnsten JH, Demas PA, Farzadegan H, Grant RW, Gourevitch MN, Cahng CJ, Buono D, Eckholdt H, Howard AA, Schoenbaum EE: Antiretroviral therapy adherence and viral suppression in HIV-infected drug users: comparison of self report and electronic monitoring. Clin Infec Dis. 2001, 33 (8): 1417-1423. 10.1086/323201.
McNabb J, Ross JW, Abriola K, Turley C, Nightingale CH, Nicolau DP: Adherence to highly active antiroviral therapy predicts virologic outcome at an inner-city human immunodeficiency virus clinic. Clin Infec Dis. 2001, 33: 700-705. 10.1086/322590.
Bangsberg DR, Charlebois ED, Grant RM: High levels of adherence do not prevent accumulation of HIV drug resistance mutations. AIDS. 2003, 17: 1925-1932. 10.1097/00002030-200309050-00011.
Walsh JC, Mandalia S, Gazzard BG: Responses to a 1 month self-report on adherence to antiretroviral therapy are consistent with electronic data and virological treatment outcome. AIDS. 2002, 16: 269-277. 10.1097/00002030-200201250-00017.
Hogg RS, Heath K, Bangsberg D: Intermittent use of triple-combination therapy is predictive of mortality at baseline and after 1 year of follow-up. AIDS. 2002, 16: 1051-1058. 10.1097/00002030-200205030-00012.
Garcia De Olalla P, Knobel H, Carmona A, Guelar A, Lopez-Colomes JL JAC: Impact of adherence of and highly active antiretroviral therapy on survival in HIV-infected patients. J Acquir Immune Defic Syndr. 2002, 30: 105-110. 10.1097/00042560-200205010-00014.
Jaffar S, Munderi P, Grosskurth H: Aherence to antiretroviral therapy in Africa: how high is it really?. Trop Med Int Health. 2008, 13 (9): 1096-1097. 10.1111/j.1365-3156.2008.02131.x.
Marchal B, Kegels G, De Brouwere V: Human resources in scaling up HIV/AIDS programmes: just a killer assumption or in need of new paradigms?. AIDS. 2004, 18 (15): 2103-2105. 10.1097/00002030-200410210-00023.
Young T, Busgeeth K: Home-based care for reducing morbidity and mortality in people infected with HIV/AIDS. Cochrane Database Syst Rev. 2010, 1: CD005417-
Ford N, Nachega JB, Engel ME, Mills EJ: Directly observed antiretroviral therapy: a systematic review and meta-analysis of randomised clinical trials. Lancet. 2009, 374: 2064-2071. 10.1016/S0140-6736(09)61671-8.
Hart JE, Jeon CY, Ivers LC, Behforouz HL, Caldas A, Drobac PC, Shin SS: Effect of directly observed therapy for highly active antiretroviral therapy on virologic, immunologic, and adherence outcomes: a meta-analysis and systematic review. J Acquir Immune Defic Syndr. 2010, 54 (2): 167-179.
Higgins JPT, Green S: Cochrane Handbook for Systematic Reviews of Interventions. 2009, West Sussex, England: John Wiley & Sons Ltd
Wong SS, Wilczynski NL, Haynes RB: Developing optimal search strategies for detecting clinically sound treatment studies in EMBASE. J Med Libr Assoc. 2006, 94 (1): 41-47.
Greenberg RS, Daniels SR, Flanders WD, Eley JW, Boring JR: Medical Epidemiology. 2001, London: Lange Medical Books, 3
Matovu F, Wabwire D, Nakibuuka J, Mubiru M, Bagenda D, Musoke P, MG F: Efficacy of Using Peer Counselors and Nurses to Support Adherence to HAART among HIV-1-infected Patients at the Prevention of MTCT Program, Mulago Hospital, Kampala, Uganda: A Randomized Non-inferiority Interventional Trial. 18th Conference on Retroviruses and Opportunistic Infections. 2011, Boston, USA: International AIDS Society
Konate I, Traore L, Ouedraogo A, Sanon A, Diallo R, Ouedraogo JL, Huet C, Millogo I, Andonaba JB, Mayaud P, Van de Perre P, Nagot N: Linking HIV prevention and care for community interventions among high-risk women in Burkina Faso–the ARNS 1222 "Yerelon" cohort. J Acquir Immune Defic Syndr. 2011, 57 (Suppl 1): S50-S54.
Gusdal AK, Obua C, Andualem T, Wahlstrom R, Chalker J, Fochsen G, INRUD-IAA project: Peer counselors' role in supporting patients' adherence to ART in Ethiopia and Uganda. AIDS Care. 2011, 23 (6): 657-662. 10.1080/09540121.2010.532531.
Igumbor JO, Scheepers E, Ebrahim R, Jason A, Grimwood A: An evaluation of the impact of a community-based adherence support programme on ART outcomes in selected government HIV treatment sites in South Africa. AIDS Care. 2011, 23 (2): 231-236.
Nglazi MD, Lawn SD, Kaplan R, Kranzer K, Orrell C, Wood R, Bekker LG: Changes in programmatic outcomes during 7 years of scale-up at a community-based antiretroviral treatment service in South Africa. J Acquir Immune Defic Syndr. 2011, 56 (1): e1-e8. 10.1097/QAI.0b013e3181ff0bdc.
Kipp W, Konde-Lule J, Saunders LD, Alibhai A, Houston S, Rubaale T, Senthilselvan A, Okech-Ojony J, Kiweewa F: Results of a community-based antiretroviral treatment program for HIV-1 infection in Western Uganda. Curr HIV Res. 2010, 8 (2): 179-185. 10.2174/157016210790442722.
Wouters E, Van Damme W, Van Loon F, van Rensburg D, Meulemans H: Public-sector ART in the Free State Province, South Africa: community support as an important determinant of outcome. Soc Sci Med. 2009, 69 (8): 1177-1185. 10.1016/j.socscimed.2009.07.034.
Wouters E, Van Damme W, van Rensburg D, Meulemans H: Impact of baseline health and community support on antiretroviral treatment outcomes in HIV patients in South Africa. AIDS. 2008, 22 (18): 2545-2548. 10.1097/QAD.0b013e32831c5562.
Shacham E, Reece M, Ong'or WO, Omollo O, Monahan PO, Ojwang C: Characteristics of psychosocial support seeking during HIV-related treatment in western Kenya. AIDS Patient Care STDS. 2008, 22 (7): 595-601. 10.1089/apc.2007.0213.
Idoko JA, Agbaji O, Agaba P, Akolo C, Inuwa B, Hassan Z, Akintunde L, Badung B, Muazu M, Danang M, Imade G, Sankale JL, Kanki P: Direct observation therapy-highly active antiretroviral therapy in a resource-limited setting: the use of community treatment support can be effective. Int J STD AIDS. 2007, 18 (11): 760-763. 10.1258/095646207782212252.
Nachega JB, Knowlton AR, Deluca A, Schoeman JH, Watkinson L, Efron A, Chaisson RE, Maartens G: Treatment supporter to improve adherence to antiretroviral therapy in HIV-infected South African adults. A qualitative study. J Acquir Immune Defic Syndr. 2006, 43 (Suppl 1): S127-S133.
Weidle PJ, Wamai N, Solberg P, Liechty C, Sendagala S, Were W, Mermin J, Buchacz K, Behumbiize P, Ransom RL, Bunnell R: Adherence to antiretroviral therapy in a home-based AIDS care programme in rural Uganda. Lancet. 2006, 368 (9547): 1587-1594. 10.1016/S0140-6736(06)69118-6.
Naidoo A, Naidoo K, Abdool Karim S, Padayatchi N, Gengiah T, Singh A, Khan M, Yende N, Murrman M, Friedland G: Impact of integrating TB and HIV care on adherence to anti-TB therapy and antiretroviral therapy, results from the Starting Tuberculosis and Anti-Retroviral Therapy - START study. 5th IAS Conference on HIV Pathogenesis, Treatment and Prevention. 2009, Cape Town, South Africa: International AIDS Society
Lester RT, Ritvo P, Mills EJ, Kariri A, Karanja S, Chung MH, Jack W, Habyarimana J, Sadatsafavi M, Najafzadeh M, Marra CA, Estambale B, Ngugi E, Ball TB, Thabane L, Gelmon LJ, Kimani J, Ackers M, Plummer FA: Effects of a mobile phone short message service on antiretroviral treatment adherence in Kenya (WelTel Kenya1): a randomised trial. Lancet. 2010, 376 (9755): 1838-1845. 10.1016/S0140-6736(10)61997-6.
Sarna A, Luchters S, Geibel S, Chersich MF, Munyao P, Kaai S, Mandaliya KN, Shikely KS, Temmerman M, Rutenberg N: Sort- and long-term efficacy of modified directly observed antiretroviral treatment in Mombasa, Kenya: a randomized trial. J Acquir Immune Defic Syndr. 2008, 48 (5): 611-619. 10.1097/QAI.0b013e3181806bf1.
Fairall LR, Bachmann MO, Zwarenstein MF, Lombard CJ, Uebel K, van Vuuren C, Steyn D, Boulle A, Bateman ED: Streamlining tasks and roles to expand treatment and care for HIV: randomised controlled trial protocol. Trials. 2008, 9: 21-10.1186/1745-6215-9-21.
Stubbs BA, Micek MA, Pfeiffer JT, Montoya P, Gloyd S: Treatment partners and adherence to HAART in Central Mozambique. AIDS Care. 2009, 21 (11): 1412-1419. 10.1080/09540120902814395.
Pearson CR, Micek MA, Simoni JM, Hoff PD, Matediana E, Martin DP, Gloyd SS: Randomized control trial of peer-delivered, modified directly observed therapy for HAART in Mozambique. J Acquir Immune Defic Syndr. 2007, 46 (2): 238-244. 10.1097/QAI.0b013e318153f7ba.
Nachega JB, Chaisson RE, Goliath R, Efron A, Chaudhary MA, Ram M, Morroni C, Schoeman H, Knowlton AR, Maartens G: Randomized controlled trial of trained patient-nominated treatment supporters providing partial directly observed antiretroviral therapy. AIDS. 2010, 24: 1273-1280.
Taiwo BO, Idoko JA, Welty LJ, Otoh I, Job G, Iyaji PG, Agbaji O, Agaba PA, Murphy RL: Assessing the viorologic and adherence benefits of patient-selected HIV treatment partners in a resource-limited setting. J Acquir Immune Defic Syndr. 2010, 54 (1): 85-92. 10.1097/01.qai.0000371678.25873.1c.
Jaffar S, Amuron B, Foster S, Birungi J, Levin J, Namara G, Nabiryo C, Ndembi N, Kyomuhangi R, Opio A, Bunnell R, Tappero JW, Mermin J, Coutinho A, Grosskurth H, Jinja Trial Team: Rates of virological failure in patients treated in a home-based versus a facility-based HIV-care model in Jinja, southeast Uganda: a cluster-randomised equivalence trial. Lancet. 2009, 374 (9707): 2080-2089. 10.1016/S0140-6736(09)61674-3.
Chang LW, Kagaayi J, Nakigozi G, Ssempijja V, Packer AH, Serwadda D, Quinn TC, Gray RH, Bollinger RC, Reynolds SJ: Effect of Peer Health Workers on AIDS Care in Rakai, Uganda: a cluster-randomized trial. PLos ONE. 2010, 5 (6): e10923-10.1371/journal.pone.0010923.
Amuron B, Coutinho A, Grosskurth H, Nabiryo C, Birungi J, Namara G, Levin J, Smith PG, Jaffar S: A cluster-randomised trial to compare home-based with health facility-based antiretroviral treatment in Uganda: study design and baseline findings. Open AIDS J. 2007, 1: 21-27. 10.2174/1874613600701010021.
Arem H, Nakyango N, Kagaayi J, Mulamba J, Nakigozi G, Serwadda D, Quinn TC, Gray RH, Bollinger RC, Reynolds SJ, Chang LW: Peer Health Workers and AIDS Care in Rakai, Uganda: a mixed methods operations research evaluation of a clluster-randomized trial. AIDS Patient Crae and STDs. 2011, 25 (12): 719-724. 10.1089/apc.2010.0349.
Mugyenyi P, Walker AS, Hakim J, Munderi P, Gibb DM, Kityo C, Reid A, Grosskurth H, Darbyshire JH, Ssali F, Bray D, Katabira E, Babiker AG, Gilks CF, Kabuye G, Nsibambi D, Kasirye R, Zalwango E, Nakazibwe M, Kikaire B, Nassuna G, Massa R, Fadhiru K, Namyalo M, Zalwango A, Generous L, Khauka P, Rutikarayo N, Nakahima W, Mugisha A, et al: Routine versus clinically driven laboratory monitoring of HIV antiretroviral therapy in Africa (DART): a randomised non-inferiority trial. Lancet. 2010, 375 (9709): 123-131.
Myers JE, Tsiouris SJ: Is there a place for directly observed therapy in HAART?. Lancet. 2009, 374: 2030-2032. 10.1016/S0140-6736(09)61991-7.
Chang LW, Alamo S, Guma S, Christopher J, Suntoke T, Omasete R, Montis JP, Quinn TC, Juncker M, Reynolds SJ: Two Year Virologic Outcomes of an Alternative AIDS Care Model: Evaluation of a Peer Health Worker and Nurse-Staffed Community-Based Program in Uganda. J Acquir Immune Defic Syndr. 2009, 50 (3): 276-282. 10.1097/QAI.0b013e3181988375.
Wringe A, Cataldo F, Stevenson N, Fakoya A: Delivering comprehensive home-based care programmes for HIV: a review of lessons learned and challenges ahead in the era of antiretroviral therapy. Health Policy Plann. 2010, 25 (5): 352-362. 10.1093/heapol/czq005.
Guidelines for the use of antiretroviral agents in HIV-infected adults and adolescents. [http://aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL04232001006.pdf]
Turner BJ: Adherence to antiretroviral therapy by human immunodeficiency virus-infected patients. J Infect Dis. 2002, 185 (Suppl 2): S143-151.
Farmer P, Leandre F, Mukherjee J, Gupta R, Tarter L, Kim JY: Community-based treatment of advanced HIV disease: introducing DOT-HAART (directly observed therapy with highly active antiretroviral therapy). Bull World Health Organ. 2001, 79 (12): 1145-1151.
Collier AC, Ribaudo H, Mukherjee AL, Feinberg J, Fischl MA, Chesney M, Adult AIDS Clinical Trials Group 746 Substudy Team: A randomized study of serial telephone call support to increase adherence and thereby improve virologic outcome in persons initiating antiretroviral therapy. J Infect Dis. 2005, 192 (8): 1398-1406. 10.1086/466526.
Birbeck GL, Chomba E, Kvalsund M, Bradbury R, Mang'ombe C, Malama K, Kaile T, Byers PA, Organek N, RAAZ Study Team: Antiretroviral adherence in rural Zambia: the first year of treatment availability. Am J Trop Med Hyg. 2009, 80 (4): 669-674.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2458/14/239/prepub
Acknowledgements
This article is an output from a PhD that was supported by projects funded by the UK Department for International Development (DFID) for the benefit of developing countries, and the Bill and Melinda Gates Foundation (Grant No. 19790.01). The views expressed in this article are not necessarily those of DFID or the Bill and Melinda Gates Foundation.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
NC, HA, PGF and KF were involved in the conception of the study. NC did the literature search, reviewed the titles, abstract and full-text, and performed the analysis. NC wrote the first draft of the manuscript and all authors revised it critically for intellectual content. All authors gave final approval of the version to be published.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited.
About this article
Cite this article
Chishinga, N., Godfrey-Faussett, P., Fielding, K. et al. Effect of home-based interventions on virologic outcomes in adults receiving antiretroviral therapy in Africa: a meta-analysis. BMC Public Health 14, 239 (2014). https://doi.org/10.1186/1471-2458-14-239
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2458-14-239