
Abstract
Background
Although many physical activity (PA) programs have been implemented and tested for effectiveness, high participation levels are needed in order to achieve public health impact. This study aimed to determine participation levels of PA programs aimed to improve PA among community-dwelling older adults.
Methods
We searched five databases up until March 2013 (PubMed, PubMed publisher, Cochrane Library, EMBASE, and Web of Science) to identify English-written studies investigating the effect of PA programs on at least one component of PA (e.g. frequency, duration) among community-dwelling populations (i.e. not in a primary care setting and/or assisted living or nursing home) of persons aged 55 years and older. Proportions of participants starting and completing the PA programs (initial and sustained participation, respectively) were determined.
Results
The search strategy yielded 11,994 records of which 16 studies were included reporting on 17 PA programs. The number of participants enrolled in the PA programs ranged between 24 and 582 persons. For 12 PA programs it was not possible to calculate initial participation because the number of older adults invited to participate was unknown due to convenience sampling. Of the five remaining programs, mean initial participation level was 9.2% (±5.7%). Mean sustained participation level of all 17 programs was 79.8% (±13.2%).
Conclusions
Understanding how to optimize initial participation of older adults in PA programs deserves more attention in order to improve the population impact of PA programs for community-dwelling older adults.
Similar content being viewed by others

Background
The worldwide population is ageing rapidly. Between 2000 and 2050, the world’s population over 60 years will double from about 11% to 22% [1], and healthcare costs will rise substantially [2]. Participating in regular physical activity (PA) is important for older adults, since it has positive effects on muscle strength, flexibility, balance, falls risk, and occurrence of chronic diseases [3], and may prevent or delay loss of independent living [4]. Preventive measures aimed at increasing PA levels should focus on those aged 55 years and older since they have been found to be at increased risk of adverse outcomes such as frailty and disability [5, 6].
High initial and sustained participation in PA programs is important for achieving public health impact [7]. However, although many PA programs have been implemented and tested for effectiveness [8], strikingly little is known about the participation levels of these programs [9, 10]. For example, low-intensity programs with a small effect and high participation rates may have a higher overall impact as compared to high-intensity programs with large effects and low participation rates [11–13]. As such, the identification of PA programs with high levels of participation is important for the development of future PA programs. Therefore, a systematic review was conducted to determine participation levels of PA programs aimed to improve PA among community-dwelling older adults aged 55 years and older. Furthermore, it was investigated what program characteristics and characteristics of participants distinct PA programs with higher participation levels from PA programs with lower participation levels.
Methods
Search strategy
Specified search strategies were developed for five bibliographic databases up until March 2013: PubMed, PubMed publisher, Cochrane Library, EMBASE, and Web of Science. The full electronic search strategy for Pubmed was:
((aged NOT (boy* OR girl* OR child*OR month* OR middle)) OR elder* OR senior* OR (old* AND (adult* OR people*))) AND (((communit* OR home) AND (living OR dwell* OR residen* OR based OR population*)) OR (residential* NOT (care OR home OR facilit*)) OR in home OR at home OR domestic*))) AND (exerci* OR sports OR physical OR activity OR activities OR walking OR swimming OR cycling OR strength OR endurance OR power OR pedometer OR accelerometer) AND (program* OR intervention* OR experiment* OR (group AND lesson*) OR government*) AND (effectiv* OR evaluat* OR outcome* OR benefit*)
The search strategies for the other databases can be found in the Additional file 1.
Study selection
Studies were included when they were: 1) written in English; 2) conducted among community-dwelling populations (i.e. not in a primary care setting and/or assisted living or nursing home); 3) among persons aged 55 years and older; 4) described programs targeting at least one component of PA (e.g. walking group, exercise class); and 5) evaluating the effect of at least one component of PA (e.g. frequency, duration). Studies were excluded when these: exclusively targeted older adults with a specific medical condition (e.g. dementia, depression), focused on cost-effectiveness; and/or reported on study protocols only.
One reviewer (MvdD) performed the initial selection of titles and abstracts in the literature search. A second reviewer (AE) was consulted to screen a random sub-set, and in case of doubt to discuss until agreement was reached. All corresponding authors of included studies were contacted and reference lists of previously published systematic reviews were checked to make sure all relevant articles were captured. This extra search did not result in extra studies eligible for inclusion.
Data extraction
A data extraction form was used to collect information on participation levels (dependent variable) and characteristics of participants and program characteristics (independent variables). Characteristics of participants included sex distribution (% females) and mean age of the participants. The program characteristics included: sampling method (probability sampling vs. convenience); method of recruitment; location (home-based vs. group-based); content (e.g. walking group); duration (months); number of contacts; supervision (yes vs. no); and (maximal) group size. Probability sampling is a method of sampling that utilizes some form of random selection, whereas convenience sampling is a technique where subjects are selected because of their convenient accessibility and proximity to the researcher (e.g. inviting through advertisements). One reviewer (MvdD) performed the data extraction and a second reviewer (AE) verified all extracted data. In case of doubt, data were discussed until agreement was reached.
Participation levels
In order to calculate participation levels the following measures were used, numbers of persons that: 1) were invited to participate (i.e. available sample); 2) started the PA program; and 3) completed the PA program. By using these measures initial and sustained participation levels were calculated. Initial participation was defined as the number of participants that enrolled in the program divided by the number of persons invited to participate. Sustained participation was defined as the number of participants who completed the program divided by the number of participants that started the program [7].
Risk of bias
Studies reporting significant effects of PA programs on PA outcomes are more likely to be published as compared to studies in which no significant results were found. However, it is unlikely that this publication bias would affect our results since we focused on participation level as the main outcome, and no differences in participation level are to be expected between effective and non-effective PA programs.
Statistical analysis
Descriptive statistics (e.g. means, standard deviations, ranges) were used to summarize the results. Mean sustained participation level was calculated for all PA programs as well as for effective PA programs only. An effective PA program was defined as a program for which a significant effect on at least one PA outcome was reported. Pearson correlations were calculated in order to investigate the correlation between participation levels and: gender distribution of the participants; mean age of the participants; program duration; and group size.
Results
Literature search
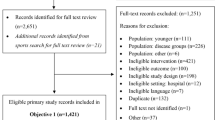
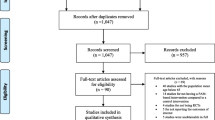
The search strategy yielded 11,994 records. After removing duplicates, 6,759 records remained which were screened based on title and abstract. Sixteen studies reporting on 17 PA programs, were included which were published between 2002 and 2013 since no studies prior to this time met the inclusion criteria (Figure 1).

PRISMA 2009 Flow Diagram.
Characteristics of participants and programs
The mean age of the participants ranged between 66 to 84 years (overall mean 73.8 ± 6.6 years). In three programs only females participated [14–16]. Of the remaining 14 PA programs, on average 70.2% (±13.3%) of the participants were females (range 47-89%).
Program characteristics that showed the most variation were the location at which the program took place and the content of the program. Six programs were home-based [14, 15, 17–20], five programs were group-based [16, 21–24], and six were both home- and group-based [25–29]. Three programs involved group-walking [14, 16, 18], seven programs involved multifaceted activities such as a combination of education and a training program [15, 17, 20, 22, 25, 27], and seven programs involved various PA such as a pedometer intervention or different exercise programs [19, 21, 23, 24, 26, 28, 29] (Table 1). PA outcomes that were evaluated were: general PA level (n = 9); walking (n = 6); and household and sports activities (n = 1).
Initial and sustained participation
The number of participants enrolled in the PA programs ranged between 24 and 582, with a mean of 174 (±165). It was not possible to calculate initial participation levels for 12 PA programs, because their applied sampling methods (e.g. convenience sampling) made it unclear how many older adults were invited to participate. The mean initial participation level of the five remaining PA programs was 9.2% (±5.7%), with a range between 1% [27] and 16% [17]. It was not possible to calculate correlations of characteristics of participants and programs with initial participation levels because of the low number of studies reporting initial participation levels.
Between 24 and 424 (mean 129 ± 117) participants completed the PA programs. The mean proportion of persons completing the program was 79.8% (±13.2%; n =17) ranging between 50.3% [25] and 100% [14, 19]. Of the 12 effective PA programs [14, 16–20, 22, 25, 27–29] the mean proportion of persons completing the program was 71.3% (±21.9%). Correlations showed that higher sustained participation levels were related to lower mean age of the participants (r = −.182), higher proportions of females (r = .279), lower duration of the program (r = −.137), and smaller group sizes (r = −.367), but none of these correlations reached significance.
Discussion
This systematic review identified 17 PA programs that aimed to improve PA among community-dwelling older adults. The mean proportion of participants starting the program (initial participation level) was 9.2%, but could only be calculated for five PA programs. The 17 PA programs had a mean sustained participation level of 79.8%. No significant correlations were found for participant or program characteristics with sustained participation level.
The mean initial participation level of 9.2% is difficult to interpret without additional information about the method of recruitment and effort or resources invested. For example 9.2% seems high when recruitment is done by putting up an advertisement in a community building, but low when mailing people personally and subsequently phoning them. Although for public health impact it is important to have insight into the number of older adults that would participate when providing a PA program [30], for 12 PA programs important information was missing. This is striking since information on initial participation gives insight into potential selective participation and in the external validity of the results. Furthermore, in the recent CONSORT statement it was emphasized to include information on the eligible participants in order to increase validity [31]. Thus, it is important that at least an indication of initial participation levels is reported when the effects of PA programs are studied. Therefore, for future studies it is highly recommended to include information regarding the number of persons that were invited to participate in the PA program. Although, none of the included PA programs in this current systematic review included online components, it is of interest to study the growing implementation of online PA programs [32] which potentially increase the ease of initial participation.
The overall mean sustained participation level of almost 80% found in the current systematic review was higher than expected, as lower participation levels have been found among children [33, 34], and for other types of health-behaviour programs for older adults [10]. The mean sustained participation level of effective PA programs was lower than the overall mean. This could imply that the effective programs have a smaller overall population impact when implemented on a larger scale as compared to programs with smaller effects but higher sustained participation levels [11–13].
No significant correlations were found for participant or program characteristics with sustained participation level which may be due to the small number of studies that were eligible for inclusion. Although the size of the correlations indicated that a low mean age of the participants, high proportions of females participating, short duration of the program, and a small group size are likely to increase levels of sustained participation, these factors should be investigated further as potential determinants of sustained participation. Jancey et al. (2007) showed that can be related to low socioeconomic status, overweight, low PA level at the start, low walking self-efficacy, and loneliness may also be related to low sustained participation levels of PA programs among older adults [35].
Conclusions
Calculating initial participation levels of PA programs aimed to improve PA levels among community-dwelling older adults is hindered by high levels of convenience sampling. Sustained participation among those who started participating in PA programs is high. A low mean age of participants, high proportions of females participating, short duration of program, and a small group size are likely to increase levels of sustained participation. In order to improve the population impact of PA programs among community-dwelling older adults, more knowledge is needed into how initial and sustained participation levels can be optimized.
References
World Health Organization: Aging and life course. http://www.who.int/ageing/en/,
Ministry of health, welfare, and sport: Constatering ‘We geven steeds meer uit aan zorg’. In report, De zorg: hoeveel extra is het ons waard?. 2012, Den Haag: Ministerie van Volksgezondheid, 6-11.
Nelson EM, Rejeski WJ, Blair SN, Duncan PW, Judge JO, King AC, Macer CA, Castaneda-Sceppa C: Physical activity and public health in older adults: recommendation from the American College of Sports Medicine and the American Heart Association. Med Sci Sports Exerc. 2007, 39 (Suppl 8): 1435-1445.
Boult C, Kane RL, Louis TA, Boult L, McCaffrey D: Chronic conditions that lead to functional limitation in the elderly. J Gerontol. 1994, 49 (Suppl 1): 28-36.
Etman A, Burdorf A, Van der Cammen TJ, Mackenbach JP, Van Lenthe FJ: Socio-demographic determinants of worsening in frailty among community-dwelling older people in 11 European countries. J Epidemiol Community Health. 2012, 66 (12): 1116-1121. 10.1136/jech-2011-200027.
Odding E, Valkenburg HA, Stam HJ, Hofman A: Determinants of locomotor disability in people aged 55 years and over: the Rotterdam study. Eur J Epidemiol. 2001, 17 (11): 1033-1041. 10.1023/A:1020006909285.
Robroek SJW, van Lenthe FJ, van Empelen P, Burdorf A: Determinants of participation in worksite health promotion programs: a systematic review. Int J of Behav Nutr Phys Act. 2009, 6: 26-10.1186/1479-5868-6-26.
Kahn EB, Ramsey LT, Brownson RC, Heath GW, Howze EH, Powell KE, Stone EJ, Rajab MW, Corso P: The effectiveness of interventions to increase physical activity A systematic review. Am J Prev Med. 2002, 22 (Suppl 4): 73-102.
Des Jarlais DCLC, Crepaz N: Improving the reporting quality of nonrandomized evaluations of behavioural and public health interventions: the TREND statement. Am J Public Health. 2004, 94: 361-366. 10.2105/AJPH.94.3.361.
Patten SBLF, Cook T: Irritable bowel syndrome: are incentives useful for improving survey response rates?. J Clin Epidemiol. 2003, 56: 256-261. 10.1016/S0895-4356(02)00586-3.
Vogt TM, Hollis JF, Lichtenstein E, Stevens VJ, Glasgow R, Whitlock E: The medical care system and prevention: the need for a new paradigm. HMO Pract. 1998, 12: 6-14.
Kristein MM, Arnold CB, Wynde EL: Health economics and preventive care. Science. 1977, 195: 457-462. 10.1126/science.402026.
Hatziandrew EJ, Sacks J, Brown R, Taylor WR, Rosenberg ML, Graham JD: The cost-effectiveness of three programs to increase use of bicycle helmets among children. Public Health Rep. 1995, 110: 251-259.
Shaw KL, Page C: A pilot community-based walking-for-exercise program for senior women. Top Geriatr Rehabil. 2008, 24 (4): 315-324. 10.1097/TGR.0b013e31818cd005.
Bonnefoy M, Boutitie B, Mercier C, Gueyffier F, Carre C, Guetemme G, Ravis B, Laville M, Cornu C: Efficacy of a home-based intervention programme on the physical activity level and functional ability of older people using domestic services: a randomized study. J Nutr Health Aging. 2012, 16 (4): 370-377. 10.1007/s12603-011-0352-6.
Michael YL, Carlson NE: Analysis of individual social-ecological mediators and moderators and their ability to explain effect of a randomized neighborhood walking intervention. Int J Behav Nutr Phys Act. 2009, 6: 49-60. 10.1186/1479-5868-6-49.
Burke L, Lee AH, Jancey J, Xiang L, Kerr DA, Howat PA, Hills AP, Anderson AS: Physical activity and nutrition behavioural outcomes of a home-based intervention program for seniors: a randomized trial. Int J Behav Nutr Phys Act. 2013, 10: 14-10.1186/1479-5868-10-14.
Cheng SP, Tsai TI, Lii YK, Yu S, Chou CL, Chen IJ: The effects of a 12-week walking program on community-dwelling elderly. Res Q Exerc Sport. 2009, 80 (3): 524-532. 10.1080/02701367.2009.10599590.
Koizumi D, Rogers NL, Rogers ME, Islam MM, Kusonoki M, Takeshima N: Efficacy of an accelerometer-guided physical activity intervention in community-dwelling older women. J Phys Act Health. 2009, 6: 467-474.
Croteau KA, Richeso NE, Farmer BC, Jones DB: Effect of a pedometer-based intervention on daily step counts of community-dwelling older adults. Res Q Exerc Sport. 2007, 78 (Suppl 5): 401-406.
Fujita K, Nagatomi R, Hozawa A, Ohkubo T, Sato K, Anza Y, Sauvaget C, Wanatabe Y, Tamagawa A, Tsuij I: Effects of exercise training on physical activity in older people: a randomized controlled trial. J Epidemiol. 2003, 13 (2): 120-126. 10.2188/jea.13.120.
Sarkisian CA, Probaska TR, Davis C, Weiner B: Pilot test of an attribution retraining intervention to raise walking levels in sedentary older adults. J Am Geriatr Soc. 2007, 55: 1842-1846. 10.1111/j.1532-5415.2007.01427.x.
Hernandes NA, Probst VS, Da Silva Jr RA, Januario RSB, Pitta F, Teixeira DC: Physical activity in daily life in physically independent elderly participating in community-based exercise program. Braz J Phys Ther. 2013, 17 (Suppl 1): 57-63.
De Vreede PL, van Meeteren NL, Samsom MM, Wittink HM, Duursma SA, Verhaar HJ: The effect of functional tasks exercise and resistance exercise on health-related quality of life and physical activity. Gerontology. 2007, 53: 12-20. 10.1159/000095387.
Hopman-Rock M, Westhoff MH: Development and evaluation of ‘aging well and healthily’: a health-education and exercise program for community-living older adults. J Aging Phys Act. 2002, 10: 364-381.
Rosenberg DE, Kerr J, Sallis JF, Norman GJ, Calfas K, Patrick K: Promoting walking among older adults living in retirement communities. J Aging Phys Act. 2012, 20: 379-394.
Rydwik E, Frandin K, Akner G: Effects of a physical training and nutritional intervention program in frail elderly people regarding habitual physical activity level and activities of daily living- a randomized controlled pilot study. Arch Gerontol Geriatr. 2010, 51: 283-289. 10.1016/j.archger.2009.12.001.
Opdenacker J, Boen F, Coorevits N, Delecluse C: Effectiveness of a lifestyle intervention and a structured exercise intervention in older adults. Prev Med. 2008, 46: 518-524. 10.1016/j.ypmed.2008.02.017.
Helbostad JL, Sletvold O, Moe-Nilssen R: Home training with and without additional group training in physically frail old people living at home: effect on health-related quality of life and ambulation. Clin Rehabil. 2004, 18: 498-508. 10.1191/0269215504cr761oa.
Glasgow RE, Vogt TM, Boles SM: Evaluating the public health impact of health promotion interventions: The RE-AIM framework. Am J Public Health. 1999, 89 (9): 1322-1327. 10.2105/AJPH.89.9.1322.
Moher D, Schulz KF, Altman DG: The CONSORT statement: revised recommendations for improving the quality of reports of parallel group randomized trials. Lancet. 2001, 357 (9263): 1191-1194. 10.1016/S0140-6736(00)04337-3.
Vandelanotte C, Spathonis KM, Eakin EG, Owen N: Website-delivered physical activity interventions: a review of the literature. Am J Prev Med. 2007, 33 (1): 54-64. 10.1016/j.amepre.2007.02.041.
Gortmaker SL, Peterson K, Wiecha J, Sobol AM, Dixit S, Fox MK, Lair N: Reducing obesity via school-based interdisciplinary intervention among youth. Ach Pediatr Adolesc Med. 1999, 153: 409-418. 10.1001/archpedi.153.4.409.
Doak CM, Visscher TLS, Renders CM, Seidell JC: The prevention of overweight and obesity in children and adolescents: a review of interventions and programs. Obes Rev. 2006, 7: 11-136.
Jancey J, Lee A, Howat P, Clarke A: Reducing attrition in physical activity programs for older adults. J Aging Phys Acty. 2007, 15: 152-165.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2458/14/1301/prepub
Acknowledgements
Many thanks to Wichor Bramer, a librarian of the Erasmus University MC who helped establishing the key-words and databases. This study was financially supported by the Erasmus University MC in Rotterdam.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
MvdD conducted the analysis and wrote together with AE the manuscript while being supervised by FJvL. CBMK critically reviewed the manuscript. All the authors have read and approved the final version to be published.
Electronic supplementary material
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
van der Deijl, M., Etman, A., Kamphuis, C.B.M. et al. Participation levels of physical activity programs for community-dwelling older adults: a systematic review. BMC Public Health 14, 1301 (2014). https://doi.org/10.1186/1471-2458-14-1301
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2458-14-1301