
Abstract
Background
Hearing difficulties is a large public health problem, prognosticated to be the ninth leading burden of disease in 2030, and may also involve large consequences for work capacity. However, research regarding sickness absence and disability pension in relation to hearing difficulties is scarce. The aim was to gain knowledge about hearing difficulties or other ear-related diagnoses and sickness absence and disability pension through conducting a systematic literature review of published studies.
Methods
Studies presenting empirical data on hearing difficulties or ear-related diagnoses and sick leave or disability pension, published in scientific peer-reviewed journals, were included. Studies were sought for in three ways: in literature databases (Pub-Med, Embase, PsycInfo, SSCI, and Cochrane) through March 2011, through scrutinising lists of references, and through contacts. Identified publications were assessed for relevance and data was extracted from the studies deemed relevant.
Results
A total of 18 studies were assessed as relevant and included in this review, regardless of scientific quality. Fourteen studies presented empirical data on hearing difficulties/ear diagnoses and sick leave and six on these conditions and disability pension. Only two studies presented rate ratios or odds ratios regarding associations between hearing difficulties and sick leave, and only two on hearing difficulties and risk of disability pension. Both measures of hearing difficulties and of sick leave varied considerable between the studies.
Conclusions
Remarkably few studies on hearing difficulties in relation to sickness absence or disability pension were identified. The results presented in them cannot provide evidence for direction or magnitude of potential associations.
Similar content being viewed by others


Background
Hearing difficulties is a major public health concern [1–5], estimated to be the ninth leading burden of disease worldwide in the year 2030 [4]. Partial or complete hearing loss as well as other ear-related diagnoses such as vertigo or tinnitus can have consequences for work capacity. Sick leave or permanent marginalization from the labour market in terms of disability pension due to these diagnoses are, however, not much discussed or studied, although interventions regarding this are warranted and need to be based on scientific knowledge [6].
Known causes of hearing difficulties include various factors such as age, noise exposure, heredity, infections, health, and socio-economic factors [7, 8]. Hearing difficulties as well as other ear-related diagnoses such as tinnitus, may lead to increased levels of stress, partly through the limited possibilities to be involved in ordinary conversions and the constant strain to hear [9]. This could potentially affect the risk of sickness absence and/or disability pension. Vertigo, balance related difficulties are also an important health problem that might lead to sick leave and exclusion from the labor market [10].
There are several indications of gender differences in the occurrence of hearing difficulties [9] as well as in sickness absence [11], why, gender stratified data regarding these aspects would be of interest.
Sickness absence has a large impact on society, employers, work sites, as well as on the individual and his or her family [6, 12]. As most individuals with a disease or an injury can work, sickness absence is seldom a good measure of morbidity on a population level [6], however, it is a good measure of the social consequences of morbidity in terms of work incapacity [6, 13]. In order to take adequate measures to prevent marginalisation among people with hearing difficulties, knowledge regarding the magnitude of such sickness absence and disability pension, is needed. Therefore, the aim of this study was to establish the current knowledgebase on hearing difficulties and other ear-related diagnoses and sickness absence and/or disability pension though conducting a systematic literature review of such studies.
Methods
The systematic literature review was conducted in accordance to the PRISMA guidelines [14], in the following five steps; searches for studies, assessment of relevance of identified publications, data extraction, categorization of studies and synthesis of results from included studies. The following inclusion criteria were applied: Studies presenting empirical data on hearing difficulties or other ear-related diagnoses as well as on sick leave or disability pension published in scientific peer-reviewed journals. Both self-reported difficulties as well as ear-related diagnoses were included, to provide a wide inclusion and try to capture disorders and difficulties, which if diagnosed, would fall in the chapter of “Diseases of the ear and mastoid process” according to the “International Statistical Classification of Diseases and Related Health Problems, Tenth Revision” (ICD-10) [15].
Studies were sought for in the following three ways, no language or time restrictions were imposed:
-
1.)
Searches, through March 2011, of the literature databases Pub-Med, Embase, PsycINFO, SSCI (Social Sciences Citation Index), and Cochrane using combinations of the following keywords: "sick leave" OR "sick-leave" OR "sickness absence" OR "sickness absent" OR "absenteeism" OR "return to work" OR "return-to-work" OR "disability pension" OR "work ability" OR "work inability" OR "work capacity" OR "work incapacity" OR "sickness benefit" OR "incapacity benefit" OR “work disability” OR “disability leave” OR “work disabled” AND "hearing" OR "deaf" OR "tinnitus" OR “vertigo” OR “auditory”. The combination of the sick-leave and hearing terms gave a total of 1229 hits (duplicates included) in PubMed (sick-leave terms and: hearing 607; deaf 160: tinnitus 46; vertigo 96; auditory 320), 2436 in Embase (sick-leave terms and: hearing 1012; deaf 443; tinnitus 101; vertigo 300; auditory 580), 51 in PsycINFO (including book chapters) (sick-leave terms and: hearing 10; deaf 8; tinnitus 0; vertigo 0; auditory 33), 1101 in SSCI (sick-leave terms and: hearing 163; deaf 119; tinnitus 38; vertigo 49; auditory 732), and 737 in Cochrane (sick-leave terms and: hearing 225; deaf 15; tinnitus 46; vertigo 66; auditory 385).
-
2.)
Scrutinising lists of references of all studies deemed relevant. This gave two additional studies.
-
3.)
Through contacts, i.e. asking other researchers if they knew about possible relevant studies. One additional study was identified.
The searches were conducted independently by two persons (E. Friberg and K. Gustafsson). All identified publications were assessed for relevance according to the above inclusion criteria. Titles and abstracts were read independently by at least two authors. In case of uncertainty or disagreement, the full article was read and, if needed discussed until consensus was reached. All relevant studies were included, irrespective of their scientific quality. Information regarding study design, population, measures, data collection, analyses performed, and relevant results (where applicable, the most adjusted result was extracted) were extracted from the included studies. Thereafter, the studies were categorized with regard to study design, type of study group (i.e. population, employees, or patients), and outcome. Finally, results from the included studies were compiled.
Results
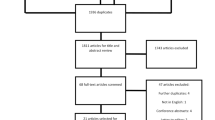
When excluding double hits from different databases, a total of 2663 publications were identified, of which 18 were assessed as relevant (Figure 1), that is, they disclosed data on hearing difficulties or other ear-related diagnoses and on sick leave [10, 16–28] and/or disability pension [17, 18, 29–32] (Table 1). The included studies were conducted in eight different countries (Sweden, USA, UK, Germany, Netherland, France, Norway and Poland, Table 1). All included studies were published in English and only three were published before the year 2000 (Figure 2). The majority (56%) of the studies had a cohort design, five (28%) had a cross-sectional design, and three were intervention studies (Table 2).

Number of identified publications and excluded, included, and relevant studies.

Number of studies published, by year.
There was considerable heterogeneity between the studies. Only four studies used population data, eight studies evaluated employed individuals, while six reported data on patients (Table 2). The hearing diagnoses/symptoms explored varied considerably between studies, including; sudden sensorineural hearing loss, otoaudiological diagnoses, unilateral vestibular loss, tinnitus, hearing impairment, Ménière’s disease, otitis media, vestibular vertigo, post-lingual hearing loss, vertigo, and ear and mastoid diagnoses. Data on hearing difficulties were in many of the studies self reported [10, 16, 19–21, 28]. Outcome variables in the studies were different types of measures of sick leave and disability pension. Only four studies presented associations (i.e. rate ratios or odds ratios) between hearing difficulties and sick leave [20, 23] or disability pension [17, 18], respectively. Five studies presented data for patient groups [16, 19, 25–27] without any control or comparison group. Several studies were based on very small samples, for example, only six studies included more than 1000 individuals [10, 17, 18, 29, 30, 32] and five studies included less than 100 individuals [19, 22, 24–26] (Table 1). The mean number of participants was 3926. Only two studies presented data stratified by sex [17, 18] while six studies only included men [23, 25, 28–31]. A majority of the studies presented data for all-cause sick leave instead of diagnoses-specific sick leave whereas half of the studies on disability pension assessed diagnoses-specific disability pension (Table 3).
Sickness absence
In all, 45 850 individuals were included in the studies presenting data on sickness absence, 44 278 with known sex, of these 47% were men. The measures of sick leave were often self-reported, only in five studies were register data used [17, 18, 24, 26, 28].
Measures of sick leave varied considerably between studies, the following measures were used: proportion of patients on sick leave and grade (full or part time) of sick leave [16], sick leave >7 days due to otoaudiological diagnoses from national registers [17], number of individuals on long-term sick leave (>8 weeks) due to vertigo or dizziness [18], sick leave yes/no [19, 27], sick leave due to hearing difficulties: yes, no, do not remember [21], absent from work more than one month due to tinnitus [26], number of days and periods of sickness benefit [28], number of days having to stay at home, leave work, or cancel a planned schedule, being bedridden or largely incapacitated during that day [22], number of absence days during a 3-year period before and after treatment from the national registers [24], absence from work due to health or due to hearing impairment [25], reported sick leave among persons with dizziness [10], self-reported number of absence days in the last 12 months and reason for sick leave [20], sick leave more than 60 days reported by physician [23].
Both studies [20, 23] that presented data on associations between hearing difficulties and sick leave observed increased risks (OR 4.6; 95% confidence interval 1.3-16.5 and 1.52 (no confidence interval reported), respectively).
Disability pension
In all, 66 610 individuals were included in the studies with information about disability pension, 63 382 with information on sex, of these 64% were men. The measure of disability pension varied somewhat, both all-cause disability pension [17, 18, 32] and diagnosis-specific disability pension [29–31] were evaluated. Disability pension was also called ill health retirement [29, 31]. The following measures of disability pension were used: granted disability pension [17, 18], granted ill health retirement due to hearing loss [29], proportions of pensions compensating for hearing loss [30], ill health retirement [31], and number of granted disability pensions among different occupational diseases [32].
The two studies presenting data on associations between hearing diagnoses as the reason for sick leave [17] or vertigo [18] and disability pension both observed an increased risk (RR 1.42; 95% CI 1.23-1.64 and RR 1.5; 95% CI 1.1-1.9, respectively).
Discussion and conclusions
The aim of this literature review was to summarize research results from published studies that present empirical data on hearing difficulties or other ear-related diagnoses and sick leave or disability pension. The most striking finding from this literature review is the low number of published studies about sickness absence or disability pension due to hearing difficulties/diagnoses, considering how prevalent such hearing difficulties are. Secondly, the vast incongruity of the results, which partly can be explained by the large amount of different exposures, outcomes and measures examined in the different studies. We could only identify 18 relevant studies to include in this review, in spite of using several different search methods. Moreover, there are remarkable few relevant studies published on associations (i.e. rate ratios or odds ratios), between hearing difficulties and sick leave [20, 23] or disability pension [17, 18], however, all the four studies with such data, reported positive associations. Only two studies reported data stratified by gender, both showing a higher risk of disability pension among women with sick-leave due to audiological [17] or vertigo [18] diagnoses compared to men. We found no studies that assessed hearing difficulties as an outcome, after, for example, sick-leave or disability pension. The extremely large variation of data on hearing difficulties and on sickness absence and disability pension means that, at this stage, it is not constructive to compare results from the different studies regarding risks for sick leave or disability pension.
The strengths of this study are the systematic approach in searching and assessing studies, including a large number of keywords and the employing of a wide search strategy in well-known literature databases. Another strength is that two researchers independently conducted the searches. The very wide search made it possible to identify studies about hearing difficulties or other ear-related diagnoses, sick leave, and disability pension from different scientific disciplines. However, we cannot rule out that we might have missed studies; some scientific journals are not included in the literature databases; for example, newly established scientific journals. Moreover, several studies only reported the information without this being the actual aim of the study in question, which increase the risk that we might have missed some studies. Furthermore, the risk of publication bias cannot be ignored, small studies showing no associations or inverse associations might not have been published at all. Nevertheless, the number of retrieved publications with this wide search strategy resulted in very few relevant studies which indicate that sick leave and disability pension with hearing difficulties or other ear-related diagnoses have not been widely studied in scientific contexts.
In areas where more studies have been conducted, usually only studies that have a minimum level of scientific quality are included in systematic reviews. It became evident that the number of conducted studies in this field did not allow for excluding studies of lower scientific quality. Instead, the aim was to use all available studies to gain knowledge, why all studies identified were included, irrespective of quality.
In conclusion, there are remarkably few studies published on associations between hearing difficulties or other ear-related diagnoses and sick leave and/or disability pension and there are very large variations between the studies regarding design, study groups, analyses, and outcome measures. Nevertheless, all studies that disclosed results on associations between hearing difficulties or other ear-related diagnoses and sick leave or disability pension reported positive associations. However, at this stage, these results cannot be considered to provide enough evidence for such associations. This finding warrants further attention and not only are more, but also better studies needed before any conclusions can be made. There is an overall lack of prospective studies with long follow-up investigating the risk of diagnosis specific sick leave and disability pension among individuals with hearing difficulties or other ear-related diagnoses. Also intervention studies targeting the workplaces more directly would be of great interest.
References
Kochkin S, Trak M VII: Hearing loss population tops 31 million people. Hearing-impaired population continues to increase - along with satisfaction ratings for hearing instruments. Hearing Review. 2005, 12: 16-29.
Wallhagen MI, Strawbridge W, Cohen RD, Kaplan GA: An increasing prevalence of hearing impairment and associated risk factors over three decades of the Alameda County Study. Am J Public Health. 1997, 87: 440-442.
Agrawal Y, Platz EA, Niparko J: Prevalence of hearing loss and differences by demographic characteristics among US adults: data from the National Health and Nutrition Examination Survey, 1999–2004. Arch Intern Med. 2008, 168: 1522-1530.
Mathers CD, Loncar D: Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006, 3: 2011-2030.
Sorri M, Roine R: Age-adjusted prevalence of hearing impairment has significantly increased during the last two decades. Scand Audiol Suppl. 2001, 54: 5-7.
Alexanderson K, Norlund A: Swedish Council on Technology Assessment in Health Care (SBU). Chapter 2. Methods used for the systematic literature search and for the review of relevance, quality, and evidence of studies. Scand J Public Health Suppl. 2004, 63: 31-35.
Rosenhall U, Jonsson R, Soderlind O: Self-assessed hearing problems in Sweden: a demographic study. Audiology. 1999, 38: 328-334.
Hasson D, Theorell T, Westerlund H, Canlon B: Prevalence and characteristics of hearing problems in a working and non-working Swedish population. J Epidemiol Community Health. 2010, 64: 453-460.
Hörselskadades Riksförbund. Årsrapport. (The Swedish Association of Hard of Hearing People, yearly report). (In Swedish). 2008, http://www.hrf.se/templates/kampanj.aspx?id=2284&baseRef=2284. Accessed September 2012
Neuhauser HK, Radtke A, von Brevern M, Lezius F, Feldmann M, Lempert T: Burden of dizziness and vertigo in the community. Arch Intern Med. 2008, 168: 2118-2124.
Alexanderson K, Norlund A: Sickness absence - causes, consequences, and physicians sickness cerification practice. A systematic literature review by the Swedish Council on Technology Assessment in Health Care. Scand J Public Health. 2004, 32 (Suppl 63): 1-263.
Marmot M, Feeney A, Shipley M, North F, Syme SL: Sickness absence as a measure of health status and functioning: from the UK Whitehall II study. J Epidemiol Community Health. 1995, 49: 124-130.
Alexanderson K: Work and Ill-health among Women and Men in Sweden. Worklife and Health in Sweden 2000. Edited by: Marklund S. 2001, Stockholm: National Institute for Working Life
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JP, Clarke M, Devereaux PJ, Kleijnen J, Moher D: The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009, 6: e1000100-
International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10).World Health Organization (WHO). 1992, http://apps.who.int/classifications/icd10/browse/2010/en. Accessed September 2012.
Carlsson PI, Hall M, Lind KJ, Danermark B: Quality of life, psychosocial consequences, and audiological rehabilitation after sudden sensorineural hearing loss. Int J Audiol. 2011, 50: 139-144.
Gustafsson K, Backenroth-Ohsako G, Rosenhall U, Ternevall-Kjerulf E, Ulfendahl M, Alexanderson K: Future risk for disability pension among people with sickness absence due to otoaudiological diagnoses: a population-based cohort study with a 12-year follow-up. Scand J Public Health. 2011, 39: 501-507.
Skooien AK, Wilhelmsen K, Gjesdal S: Occupational disability caused by dizziness and vertigo: a register-based prospective study. British Journal of General Practice. 2008, 58: 619-623.
Bjerlemo B, Kollén L, Boderos I, Kreuter M, Möller C: Recovery after early vestibular rehabilitation in patients with acute unilateral vestibular loss. Audiological Medicine. 2006, 4: 117-123.
Kramer SE, Kapteyn TS, Houtgast T: Occupational performance: comparing normally-hearing and hearing-impaired employees using the Amsterdam checklist for hearing and work. Int J Audiol. 2006, 45: 503-512.
Hagberg M, Thiringer G, Brandstrom L: Incidence of tinnitus, impaired hearing and musculoskeletal disorders among students enrolled in academic music education–a retrospective cohort study. Int Arch Occup Environ Health. 2005, 78: 575-583.
Gates GA, Green JD, Tucci DL, Telian SA: The effects of transtympanic micropressure treatment in people with unilateral Meniere's disease. Arch Otolaryngol Head Neck Surg. 2004, 130: 718-725.
Chau N, Gauchard GC, Siegfried C, Benamghar L, Dangelzer JL, Francais M, Jacquin R, Sourdot A, Perrin PP, Mur JM: Relationships of job, age, and life conditions with the causes and severity of occupational injuries in construction workers. Int Arch Occup Environ Health. 2004, 77: 60-66.
Bjorne A, Agerberg G, Bjorne A, Agerberg G: Reduction in sick leave and costs to society of patients with Meniere's disease after treatment of temporomandibular and cervical spine disorders: a controlled six-year cost-benefit study. Cranio. 2003, 21: 136-143.
Joore MA, Brunenberg DEM, Chenault MN, Anteunis LJC: Societal effects of hearing aid fitting among the moderately hearing impaired. International Journal of Audiology. 2003, 42: 152-160.
Holgers KM, Erlandsson SI, Barrenas ML: Predictive factors for the severity of tinnitus. Audiology. 2000, 39: 284-291.
Andersson G: Longitudinal follow-up of occupational status in tinnitus patients. Int Tinnitus J. 2000, 6: 127-129.
Rudin R, Svardsudd K: Otitis media and well-being in a male population in Gothenburg. The study of men born in 1913. Acta Otolaryngol. 1987, 104: 454-462.
Ide C: Hearing loss, accidents, near misses and job losses in firefighters. Occup Med (Lond). 2007, 57: 203-209.
Sewell RK, Song C, Bauman NM, Smith RJ, Blanck P: Hearing loss in Union Army veterans from 1862 to 1920. Laryngoscope. 2004, 114: 2147-2153.
Ide CW: Failing firefighters: a survey of causes of death and ill-health retirement in serving firefighters in Strathclyde, Scotland from 1985–94. Occup Med (Lond). 1998, 48: 381-388.
Starzynski Z, Izycki J: Occupational diseases in Poland during the years 1984–1992. Pol J Occup Med Environ Health. 1993, 6: 299-308.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2458/12/772/prepub
Acknowledgement
This study was financed by the Swedish Council for Working Life and Social Research (FAS by Swedish acronym) Center program Hearing Disabilities in Working Life and Society. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interest
The authors declare that they have no conflict of interest.
Authors’ contributions
Study concept and design: EF, KA. Systematic literature search: EF, KG. Interpretations of data: EF, KG, KA. Drafting of the manuscript: EF. Critical revision of the manuscript for important intellectual content: KG, KA. All authors have read and approved final version of manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
{kind=link}
{kind=link}
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Friberg, E., Gustafsson, K. & Alexanderson, K. Hearing difficulties, ear-related diagnoses and sickness absence or disability pension - a systematic literature review. BMC Public Health 12, 772 (2012). https://doi.org/10.1186/1471-2458-12-772
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2458-12-772