
Abstract
Background
Dental decay is the most common childhood disease worldwide and most of the decay remains untreated. In the Philippines caries levels are among the highest in the South East Asian region. Elementary school children suffer from high prevalence of stunting and underweight.
The present study aimed to investigate the association between untreated dental decay and Body Mass Index (BMI) among 12-year-old Filipino children.
Methods
Data collection was part of the National Oral Health Survey, a representative cross-sectional study of 1951 11-13-year-old school children using a modified, stratified cluster sampling design based on population classifications of the Philippine National Statistics Office. Caries was scored according to WHO criteria (1997) and odontogenic infections using the PUFA index. Anthropometric measures were performed by trained nurses. Some socio-economic determinants were included as potential confounding factors.
Results
The overall prevalence of caries (DMFT + dmft > 0) was 82.3% (95%CI; 80.6%-84.0%). The overall prevalence of odontogenic infections due to caries (PUFA + pufa > 0) was 55.7% (95% CI; 53.5%-57.9%) The BMI of 27.1% (95%CI; 25.1%-29.1%) of children was below normal, 1% (95%CI; 0.5%-1.4%) had a BMI above normal. The regression coefficient between BMI and caries was highly significant (p < 0.001). Children with odontogenic infections (PUFA + pufa > 0) as compared to those without odontogenic infections had an increased risk of a below normal BMI (OR: 1.47; 95% CI: 1.19-1.80).
Conclusions
This is the first-ever representative survey showing a significant association between caries and BMI and particularly between odontogenic infections and below normal BMI. An expanded model of hypothesised associations is presented that includes progressed forms of dental decay as a significant, yet largely neglected determinant of poor child development.
Similar content being viewed by others

Background
Dental decay (caries) is the most common childhood disease and the most frequent non-communicable disease worldwide [1, 2]. Most of the dental decay remains untreated with significant impacts on general health, quality of life, productivity, development and educational performance [3–6]. In the Philippines caries levels are among the highest in the South East Asian region, with a prevalence of 82% and a Decayed, Missing and Filled permanent Tooth index (DMFT) of 2.9 among 12-year-olds in 2006 [7, 8].
Besides, children in the Philippines as in many other low- and middle-income countries, suffer from a high burden of preventable diseases other than dental decay: diarrhoea and respiratory tract infections, the top killer diseases among children. Two-thirds of school children are infected with chronic soil-transmitted helminths (STH) [9]. Because of these poor health conditions children suffer from significant impacts on their development, growth, well-being, as well as their social and educational performance. With regard to growth development, low Body Mass Index (BMI) is very prevalent in the Philippines, like in many other low- and middle-income countries [10].
Despite the pandemic character of dental decay, particularly in children, there are only a few studies that have examined the relationship between the severity of dental decay and child weight. Previous research concluded that children with early childhood caries (ECC) who needed treatment for tooth extraction had lower mean weights than those without treatment need [11–13]. In larger surveys among 1-6-year-old non-hospital visitors, the relationship between caries and underweight remained inconclusive [14–19]. A recent large population-based prospective cohort study in the United Kingdom (UK) among 5-year olds reported that children with tooth decay had slightly smaller increases in weight and height in the previous years than children without tooth decay [20]. Virtually nothing is known about this association in older age groups.
The present study aimed to investigate the association between dental decay and low BMI, 2 highly prevalent conditions among 12-year-old Filipino children. The hypothesis was tested that an association between dental decay and low BMI in 12-year-old Filipino children did not exist. Weight, height, caries prevalence and caries experience as well as some demographic and socio-economic variables were included in a National Oral Health Survey (NOHS) undertaken in 2006.
Methods
Sample
The NOHS was conducted from November 2005 to February 2006 using a stratified cluster sampling design. All 17 regions of the country were included, in each region a rural and urban area were identified according to the criteria of the National Statistics Office. In total, 68 public elementary schools were selected for the survey, 2 in each stratum (n = 34). Inclusion criteria for schools were: a location in a secure area; access within an hour from the main road; and schools having more than 60 grade VI children. In each school 30 grade VI children aged 11-13 years were systematically sampled from a list of enrolled schoolchildren. This sample size was estimated on the presumption of a caries prevalence of 80%, a desired precision of ± 2% with a confidence level at 95%. Ethical approval was obtained from the Department of Education under whose authority this survey was undertaken.
Oral examination
All children brushed their teeth prior to examination. Oral examinations were performed outside in the schoolyard with children lying in a supine position on a school bench or table with their heads on a pillow on the lap of the examiner who sat behind them. Cotton pellets were used for drying. A CPI ball-ended probe and a lighted mouth mirror (MIRRORLIGHT™, Kudos, Hong Kong) were used as examination tools to score caries according to standard procedures described by WHO (1997) [21]. Initial caries lesions and early stages of cavitation where the ball-ended probe could not enter were not scored as caries, unless a greyish appearance of enamel as a sign of an underlying dentine involvement with caries was noted.
In addition to data collection for DMFT/dmft (permanent and primary dentition) the PUFA/pufa index was used according to the standard procedure [22]. PUFA/pufa is an index used to assess the presence of oral conditions and infections resulting from untreated caries in the primary (pufa) and permanent (PUFA) dentition. The index is recorded separately from the DMFT/dmft and scores the presence of either a visible pulp (P/p), ulceration of the oral mucosa due to root fragments (U/u), a fistula (F/f) or an abscess (A/a). The PUFA/pufa index per child is calculated in the same cumulative way as the DMFT/dmft index and represents the number of teeth meeting the PUFA/pufa diagnostic criteria.
5 survey teams, each consisting of 2 dentists and 2 recorders underwent 2 days of theoretical and 3 days of clinical training in caries (DMFT/dmft) and PUFA/pufa diagnosis and calibration. During the entire survey, each examiner re-examined 7.5% of the children and reproducibility was assessed with Kappa values.
Anthropometric measures
All measurements were performed by trained school nurses according to standard guidelines [23]. The height of children, standing upright without shoes, was measured with a portable stadiometer (Seca®) to the nearest 0.5 cm. Weight was assessed with a portable electronic digital scales to the nearest 0.5 kg (Soehnle®). No adjustments were made for clothing, but children were only lightly dressed. The measuring equipment was re-calibrated daily. Height and weight were used to compute BMI (weight in kilograms divided by height in metres squared - weight (kg)/height (m2)) for age. The children were grouped in 3 categories of BMI with age and sex related cut-off points according to the criteria of WHO (Thinnes [24]), CDC (Thinnes [25]), Philippine NHANS I [26] and Cole (Thinnes grade 2 [27]). For further analyses, the 3 BMI categories according to the Philippine NHANS I criteria were used (Table 1).
Demographic and socio-economic parameters
Teachers provided information on place of residence, gender and age of the child. The child was asked about the number of siblings and whether there was a television set at home.
Statistical methods
The data were analysed with SAS 9.1 software. Examiner's reproducibility of oral conditions at tooth level was measured by Kappa statistics. The caries status (including odontogenic infections), caries prevalence and caries experience, were combined for the primary and permanent dentition. A regression equation between BMI and caries and between BMI and odontogenic infections (PUFA) was calculated and presented in a scatter plot. For further analysis, the variable caries status was dichotomised into caries free children versus children with caries. Children with odontogenic infections were dichotomised into those with odontogenic infections versus those without and into children with one odontogenic infection versus children with more than one odontogenic infection. BMI was the dependent variable in all analyses. Chi-square and Student-t-tests were used for comparison between groups. Since the number of children with a BMI above normal was small, the BMI was dichotomised into below normal BMI versus normal together with above normal BMI. In the logistic regression model only those explanatory variables were introduced that showed statistical significance (P < 0.05) in bi-variate analysis with low BMI as dependent variable.
Results
From a total of 2022 11-13-year-old children, 1951 (949 boys and 1002 girls) with a mean age 11.8 years were included in the analysis. Of the 71 excluded children due to incomplete data, 33 were boys and 38 were girls.
Inter-examiner Kappa values for caries detection assessed after the calibration session were in the range from 0.78 to 0.92, which can be judged as good. Throughout the NOHS, 7.5% of children were re-examined in order to assess intra-examiner consistency. Intra-examiner reproducibility varied between Kappa values of 0.80 to 0.98 for scoring DMFT/dmft and 0.80 to 0.97 for PUFA/pufa.
Caries
The frequency distributions of children with caries and odontogenic infections (PUFA) are presented (Figure 1). The mean prevalence of caries (DMFT + dmft > 0) is 82.3% (95%CI; 80.6%-84.0%) and the mean prevalence of odontogenic infections (PUFA + pufa > 0) is 55.7% (95% CI; 53.5%-57.9%). The prevalence data are summarised in Table 2 for gender, demography, and socio-economic determinants. There are no significant differences in the caries prevalence between the variables. The mean experience of caries (DMFT + dmft) is 3.12 and the mean experience of odontogenic infections (PUFA + pufa) is 1.15. The caries experience data are summarised in Table 3 for the same variables and no significant differences were found. The filled (F/f) component was close to zero and the missing (M) component (due to caries) was 7% of the total caries experience.

Distribution of caries lesions and caries lesion that progressed into the pulp (PUFA) of 11-13-year olds.
BMI
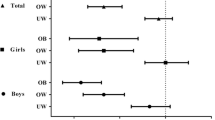
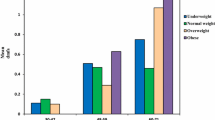
The frequency distributions of the 3 categories of BMI with sex and age related cut-off point according to WHO, CDC, Philippine NHANS I and Cole are presented in Figure 2. Figure 3 depicts the distribution of the 3 BMI categories, obtained with the Philippine NHANS I criteria, according to the number of DMFT and the number of odontogenic infections (PUFA). A scatter plot depicting each child for BMI and number of DMFT and a scatter plot showing each child for BMI and number of odontogenic infections (PUFA) are presented in Figure 4. The regression equation for the relation between BMI versus DMFT and BMI versus PUFA, are statistically significant (p < 0.001). The regression coefficient for BMI versus PUFA is larger than the one for BMI versus DMFT, indicating a stronger effect for PUFA on BMI. Table 4 gives the numbers and percentages of the 3 categories of BMI according to dichotomised explanatory variables. Of the child sample, 50% were children from rural areas, 38% of children lived in large families with more than 4 siblings and 74% had a TV set at home. The BMI of 27.1% (95%CI; 25.1%-29.1%) of children was below normal and 1% (95%CI; 0.5%-1.4%) had a BMI above normal. The prevalence of low BMI was similar for caries free children and children with caries, but the prevalence of low BMI was significantly higher in children with odontogenic infections (PUFA/pufa > 0) as compared with children without odontogenic infections. Associations were found between low BMI and gender, TV set at home, large families and odontogenic infections. The associated explanatory variables were introduced into a logistic regression model with low BMI as dependent variable. Table 5 depicts the results. Boys, children in large families (>4 siblings) and children with odontogenic infections (PUFA + pufa) were more likely to have a low BMI with an odds ratio (OR) of 1.52, 1.39 and 1.47, respectively.

Distribution of the 3 categories of BMI of the sample of 12-year-old boys and girls according to the cut-off points of the 11-, 12- and 13-year olds of WHO, CDC, Philippines (NHANS I) and Cole.

Distribution of the 3 BMI categories according to the number of caries lesions into the pulp (a) and the number of caries lesions (b).

Scatter plots presenting each child (*) with BMI and number of lesions into the pulp (PUFA) (a) and with BMI and number of DMFT (b) and regression line (formula).
Discussion
The data presented in this paper were collected using a systematic representative random sample from the Philippine National Oral Health Survey in 2006, which is one of a new generation of oral health surveys that, in addition to the traditional tooth-related indicators, take socio-economic and anthropometric parameters into account [8]. The survey was also the first to use the new PUFA index to assess the amount of odontogenic infection resulting from advanced untreated decay. The introduction of the PUFA index in this study examining possible associations between dental decay and low BMI appeared to be relevant, since it created a clear differentiation in the findings. Although a significant association existed between BMI and caries, only children with caries progression into the pulp (odontogenic infections) appeared to have an increased risk of a below normal BMI as compared to those without odontogenic infections. These findings imply that the null hypothesis was rejected with an added nuance that:
-
Children with caries had no increased risk of a below normal BMI as compared to caries free children; whereas
-
Children with caries into the pulp (odontogenic infections) had an increased risk of below normal BMI as compared to children without odontogenic infections.
Our study design is a cross-sectional study, which limits the ability to identify causative factors. A longitudinal design would be more adequate to reveal cause and effect relationships. There are indications from several longitudinal studies that treatment of severe caries resulted in weight gain [28–30]. If untreated caries progresses into the dental pulp there are possibly 3 main pathways for this association: 1) pain and discomfort result in reduced food intake; 2) reduced quality of life affects children's growth and development through restricted activity, reduced sleep, concentration deficits etc; and 3) odontogenic infections may result in cytokine release which might impact on growth. One study on inflammatory periodontal diseases reported an association with cytokine release [31], but this issue is yet highly speculative. Future research will hopefully provide a more complete picture of the causal relationships, of the nature of the relation over time from early childhood to adolescence, and of the impact of different oral care options on child development.
In contrast to reports from other countries with similar socio-economic status this survey did not find any significant differences between 12-yr-old children from rural and urban areas in terms of caries prevalence, caries experience (DMFT + dmft), odontogenic infections (PUFA + pufa) and BMI [32–36]. A possible explanation for a lack of stratification effects on the studied variables could be the absence of higher socio-economical classes in the present study, since private schools that are mainly located in urban areas were not included in the sample.
This study indicated a higher risk of low BMI for boys compared to girls and for children in large families as compared to children in smaller families, which cannot be attributed to the caries status (Table 2 and 3). The percentage of 31% for low BMI of boys being higher than the 23% for girls is in accordance with the last national update on nutritional status of children in 2005 [10]. Low BMI is a result of several complex factors. Lack of hygiene, lack of nutritious food, as well as respiratory and other infections could account for differences in BMI between boys and girls. Additional factors that may also be considered include for instance that males are more active in sports. For practical and resource reasons it was not possible to obtain stool samples to test for worm infestation. However, STH infections are highly prevalent in Filipino children with an average national prevalence of 82.3% [9]. The summarised results from studies on STH infections do not indicate a difference in the prevalence and severity between boys and girls [9, 37]. Given the high prevalence and the sample size of the survey it is not expected that a differing STH infection status affected the associations between dental decay and BMI found.
An expanded model of hypothesised relations
The contemporary scientific discourse among paediatricians, nutritionists and even international organisations and NGOs related to child health and development, has so far completely ignored the impact of untreated dental decay. Virtually all dental decay remains untreated and contributes to poor child development and educational performance. This may be a result of the still new and growing evidence about the relation between dental decay and child development, but it is also a result of a disconnection between dental researchers and the "mainstream" of child development research.
A recent model visualises the possible complex relationships between the many factors ranging from nutritional deficits to maternal depression, from infectious diseases to intrauterine factors [38]. In order to bridge the gap between the "scientific niche" of oral-health-related research and child development we present a modified model for the hypothesised causal relationships leading to poor education performance of children (Figure 5). It builds on the research already published and adds the dimension of a specific and highly prevalent chronic disease, dental decay, particularly dental decay that has progressed into the pulp and highlights pathways of interaction with all of the established factors contributing to poor child development. By placing dental decay in the centre of the diagram we do not imply that untreated caries and the resulting chronic infections are the most important factor for suboptimal child development; we rather wanted to highlight the complexity of interrelations among the various factors.

Hypothesised relations between determinants of poor child development, poor school achievement and odontogenic infections.
Although the extent of the negative effect of odontogenic infections compared to other determinants in this context still needs to be quantified by further research, early results from ongoing studies and previous research indicate that removing odontogenic infection has a significant positive effect on subsequent child growth and development. In addition, simple and cost-effective measures for preventing dental decay exist, which could easily be applied comprehensively and on a mass scale in school health programmes [39]. We suggest that the absence of odontogenic infections (PUFA + pufa = 0) can be considered as an important outcome indicator for (oral) health programme planning, monitoring and evaluation.
In the context of increased efforts to achieve the United Nation's Millennium Development Goals (MDG), and more specifically Goals 1 and 2 related to hunger and education, it would seem to be important to address the determinants of child development, nutrition status and educational performance comprehensively and from different perspectives. Good oral health is closely related to all MDG goals [40]. Poor oral health is the result of neglect of oral hygiene as respiratory and intestinal infections are the result of lack of general hygiene (of hands). Given that most other determinants of poor child development are rather complex, the relatively simple interventions for improving oral and general hygiene health of the world's disadvantaged children should be among the priority choices for health planners. Looking for quick, comparatively easy and cost-effective measures to contribute to the timely achievement of the MDGs, the 'Fit for School' programme in the Philippines, that addresses hygiene-related diseases, worm diseases and dental decay in a simple and cost-effective package, is a good and realistic example [39].
Conclusions
This is the first-ever representative survey showing a significant association between caries and BMI and particularly between odontogenic infections and below-normal BMI. The data of this cross-sectional study indicate that children with odontogenic infection have an increased risk of below normal BMI as compared to children without odontogenic infections.
Abbreviations
- STH:
-
Soil-transmitted helminths
- DMFT/dmft:
-
Decayed, Missing and Filled Tooth (Permanent/primary dentition)
- PUFA/pufa:
-
Presence of oral conditions and infections resulting from untreated caries (Permanent/primary dentition)
- BMI:
-
Body Mass Index
- ECC:
-
Early Childhood Caries
- NOHS:
-
National Oral Health Survey
- OR:
-
Odds ratio
- P/p:
-
Visible pulp
- U/u:
-
Ulceration of the oral mucosa due to root fragments
- A/a:
-
Abscess
- F/f:
-
Fistula
- M/m:
-
Missing
- MDGs:
-
Millennium Development Goals.
References
Edelstein BL: The dental caries pandemic and disparities problem. BMC Oral Health. 2006, 6 (Suppl 1): S2-10.1186/1472-6831-6-S1-S2.
Petersen PE, Bourgeois D, Ogawa H, Estupinan-Day S, Ndiaye C: The global burden of oral diseases and risks to oral health. Bull World Health Organ. 2005, 83: 661-669.
Slade GD: Epidemiology of dental pain and dental caries among children and adolescents. Community Dent Health. 2001, 18: 219-227.
Thomas CW, Primosch RE: Changes in incremental weight and well being of children with rampant caries following complete dental rehabilitation. Pediatric Dent. 2002, 24: 109-113.
Sheiham A: Dental caries affects body weight, growth and quality of life in pre-school children. Br Dent J. 2006, 201: 625-626. 10.1038/sj.bdj.4814259.
Sheller B, Churchill SS, Williams BJ, Davidson B: Body mass index of children with severe early childhood caries. Pediatr Dent. 2009, 31: 216-221.
Beaglehole R, Benzian H, Crail J, Mackay J: The Oral Health Atlas: mapping a neglected global health issue. 2009, Geneva & Brighton: FDI World Dental Education Ltd & Myriad Editions
Department of Education, Health and Nutrition Center: National oral health survey among the public school population in the Philippines. 2008, Manila: Department of Education
Belizario V, de Leon WU, Lumampao YF, Anastacio MB, Tai CM: Sentinel surveillance of soil-transmitted helminthiasis in selected local government units in the Philippines. Asia Pacific J Publ Health. 2009, 21: 26-42. 10.1177/1010539508327245.
Food and Nutrition Research Institute: Nutritional status of Filipino children and selected population groups: 2005 Update. 2005, Manila: Department of Science and Technology, [http://www.fnri.dost.gov.ph/files/fnri%20files/facts2005/content.pdf]
Miller J, Vaughan-Williams E, Furlong R, Harrison L: Dental caries and children's weights. J Epidemiol Community Health. 1982, 36: 49-52. 10.1136/jech.36.1.49.
Acs G, Lodolini G, Kaminsky S, Cisneros GJ: Effect of nursing caries on body weight in a pediatric population. Pediatr Dent. 1992, 14: 302-305.
Ayham H, Suskan E, Yildirim S: The effect of nursing caries or rampant caries on height, body weight and head circumference. J Clin Pediatr Dent. 1996, 20: 209-212.
Cleaton-Jones P, Sinwell R, Mogotsi M, Richardon BD, Granath L, Fatti LP, Walker AR: Nutritional status and dental caries in a large sample of 4-and 5-year-old South African children. SA J Clin Nutr. 2000, 90: 631-635.
Abolfotouh MA, Hassan KH, Khattab MS, Youssef RM, Sadek A, El-Sehaiei M: Dental caries experience in relation to wasting and stunted growth among schoolboys in Abha, Saudi Arabia. Ann Saudi Med. 2000, 20: 360-363.
Cameron FL, Weaver LT, Wright CM, Welbury RR: Dietary and social characteristics of children with severe tooth decay. Scott Med J. 2006, 51: 26-29. 10.1258/rsmsmj.51.3.26.
Oliviera LB, Sheiham A, Bönecker M: Exploring the association of dental caries with social factors and nutritional status in Brazilian preschool children. Eur J Oral Sci. 2008, 116: 37-43. 10.1111/j.1600-0722.2007.00507.x.
van Gemert-Schriks MCM, van Amerongen EW, Aartman IHA, Wennink JMB, Ten Cate JM, de Soet JJ: The influence of dental caries on body growth in prepubertal children. Clin Oral Investig. 2011, 15: 141-149. 10.1007/s00784-010-0380-3.
Ngoenwiwatkul Y, Leela-Adisorn N: Effects of dental caries on nutritional status among first-grade primary school children. Asia Pacific J Publ Health. 2009, 21: 177-183. 10.1177/1010539509331787.
Kay EJ, Northstone K, Ness A, Duncan K, Crean SJ: Is there a relationship between birthweight and subsequent growth on the development of dental caries at 5 years of age. A cohort study. Community Dent Oral Epidemiol. 2010, 38: 408-414. 10.1111/j.1600-0528.2010.00548.x.
World Health Organization: Oral Health Surveys: Basic methods. 1997, Geneva: WHO, 4
Monse B, Heinrich-Weltzien R, Benzian H, Holmgren C, van Palenstein Helderman W: PUFA - An index of clinical consequences of untreated dental caries. Community Dent Oral Epidemiol. 2010, 38: 77-82. 10.1111/j.1600-0528.2009.00514.x.
Lohmann TG, Roche AF, Martorelli R: Anthropometric standardization reference manual. 1988, Chamaign, IL: Human Kinetics
de Onis M, Onyango AW, Borghi E, Siyam A, Nishida C, Siekmann J: Development of a WHO growth reference for school-aged children and adolescents. Bull World Health Organ. 2007, 85: 649-732.
Kuczmarski RJ, Ogden CL, Grummer-Strawn LM, Flegal KM, Guo SS, Wei R, Mei Z, Curtin LR, Roche AF, Johnson CL: CDC growth charts: United States. Adv Data. 2000, 314: 1-27.
Department of Education, Health and Nutrition Center: International reference standards (IRS) growth tables in nutritional assessment of school children. 2003, Food and Nutrition Research Institute, Reference data based on the NHANES I using the cutoffs of Must A, Dallal GE, Dietz WH: Reference data for obesity: 85th and 95th percentiles of body mass index (wt/ht2) and triceps skinfold thickness. AM J Clin Nutr 1991, 53:839-846.
Cole TJ, Flegal KM, Nicholls D, Jackson AA: Body mass index cut offs to define thinness in children and adolescents: international survey. BMJ. 2007, 335: 194-204. 10.1136/bmj.39238.399444.55.
Acs G, Lodolini G, Shulman R, Chussid S: The effect of dental rehabilitation on the body weight of children with failure to thrive: case reports. Compend Contin Educ Dent. 1998, 19: 164-171.
Acs G, Shulman R, Ng MW, Chussid S: The effect of dental rehabilitation on the body weight of children with early childhood caries. Pediatr Dent. 1999, 21: 109-113.
Malek Mohammadi TM, Wright CM, Kay EJ: Childhood growth and dental caries. Community Dent Health. 2009, 26: 38-42.
Seymour GJ, Ford PJ, Cullinan MP, Leishman S, Yamazaki K: Relationship between periodontal infections and systematic disease. Clin Microbiol Infect. 2007, 13 (Suppl 4): 3-10.
Jürgensen N, Petersen PE: Oral health and the impact of socio-behavioural factors in a cross sectional survey of 12-year old school children in Laos. BMC Oral Health. 2009, 9: 29-10.1186/1472-6831-9-29.
Walker SP, Wachs TD, Gardner JM, Lozoff B, Wasserman GA, Pollitt E, Carter JA, International Child Development Steering Group: Child development: risk factors for adverse outcomes in developing countries. Lancet. 2007, 369: 145-157. 10.1016/S0140-6736(07)60076-2.
Shen T, Habicht JP, Chang Y: Effect of economic reforms on child growth in urban and rural areas of China. N Engl J Med. 1996, 335: 400-406. 10.1056/NEJM199608083350606.
Ministry of Health: Department of health services annual report 20059/59 (2001/2002). 2003, Kathmandu: His Majesty's Government of Nepal, Ministry of Health
Hobdell MH, Oliveira ER, Bautista R, Myburgh NG, Lalloo R, Narendran S, Johnson NW: Oral diseases and socio-economic status (SES). Br Dent J. 2003, 194: 91-96. 10.1038/sj.bdj.4809882.
Baldo E, Belizario V, de Leon W, Kong H, Chung D: Infection status of intestinal parasites in children living in residential institutions in Metro Manila, the Philippines. Korean J Parasitology. 2004, 2: 67-70.
Grantham-McGregor S, Cheung YB, Cueto S, Glewwe P, Richter L, Strupp B: Developmental potential in the first 5 years for children in developing countries. Lancet. 2007, 369: 60-70. 10.1016/S0140-6736(07)60032-4.
Monse B, Naliponguit E, Belizario V, Benzian H, van Palenstein Helderman W: Essential health care package for children - the "Fit for School" program in the Philippines. Int Dent J. 2010, 60: 1-9.
Bueno RE, Moyses SJ, Moyses ST: Millennium development goals and oral health in cities in southern Brazil. Community Dent Oral Epidemiol. 2010, 38: 197-205. 10.1111/j.1600-0528.2010.00531.x.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2458/11/558/prepub
Acknowledgements and Funding
Data collection was part of the National Oral Health Survey, which was financed by the German Federal Ministry for Economic Cooperation & Development (Title 685.01, through InWent Capacity Building, Bonn, Germany).
The funding entity had no involvement in 1) study design; 2) the collection, analysis, and interpretation of data; 3) the writing of the report; and 4) the decision to submit the manuscript for publication.
None of the authors received any funding for writing the paper.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
BM and RH supported the data collection in the field, JM performed the statistical data analysis, WvP and MH contributed to the critical interpretation of the data. HB drafted the first version of the paper, and was involved in the data collection and its interpretation. All authors contributed equally to the final version of the paper and have read as well as approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Benzian, H., Monse, B., Heinrich-Weltzien, R. et al. Untreated severe dental decay: a neglected determinant of low Body Mass Index in 12-year-old Filipino children. BMC Public Health 11, 558 (2011). https://doi.org/10.1186/1471-2458-11-558
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2458-11-558