
Abstract
Background
Birth weight is negatively associated with cardiovascular diseases and diabetes, but the associations are less well-established in developing populations where birth weight is often unavailable. We studied the association of birth weight and cardiovascular risk, using birth rank as an instrumental variable, in Southern China.
Methods
We used published data on birth weight by birth rank from an appropriate population and baseline data from the Guangzhou Biobank Cohort Study phases 2 & 3 (2005-8) to examine the adjusted associations, using instrumental variable analysis, of birth weight with clinically measured cardiovascular risk factors and the metabolic syndrome in older (≥ 50 years) men (n = 5,051) and women (n = 13,907).
Results
Estimated birth weight was associated with lower blood pressure (systolic -0.25 mm Hg 95% confidence interval (CI), -0.53 to 0.03 and diastolic -0.33 mm Hg 95% CI -0.48 to -0.18 per standard deviation higher birth weight), but had little association with glucose, lipids, waist-hip ratio, body mass index or the metabolic syndrome, adjusted for age, sex, early environment and number of offspring.
Conclusion
Birth weight may impact blood pressure; however associations of birth weight with other cardiovascular risk factors may not be related to foetal exposures, but speculatively could be an historical co-incidence, with corresponding implications for prevention.
Similar content being viewed by others


Background
Lower birth weight is associated with higher risk of cardiovascular diseases (CVD) [1, 2], hypertension [3], diabetes [4, 5], and perhaps poor lipids in adulthood [6, 7], although maternal diabetes in pregnancy and fetal over growth may also be implicated in diabetes [8]. Moreover some of the effects are fairly small, and the underlying causative exposure(s) and mechanism(s) driving the association between lower birth weight and adult cardiovascular diseases are not, as yet, fully understood, possibly because other aspects of fetal development, such as body composition at birth [9], are more important. Maternal adiposity may contribute to higher birth weight [10]. Perhaps because of the difficulty of manipulating birth weight [11], as well as potential ethical problems, almost all the evidence concerning humans comes from observational studies, which may be inherently open to uncontrollable biases. There are many experimental animal studies investigating the impact of pre-natal under-nutrition on CVD risk, whether these generalize to humans, where maternal supplementation has little effect on CVD risk [12], remains unclear [13], although the effects of over-nutrition may be clearer [14, 15]. Moreover, most of these observations come from studies in long-term industrialised populations, where it is difficult to disentangle the effects of birth weight from its social context including previous inter-generational exposures and subsequent exposures across the life course, including growth and final size. In developing populations birth weight is typically lower than in long-term industrialised countries, and thus may be a relatively more important contributor to the growing epidemic of non-communicable chronic diseases, and hence also an important intervention target. However, there is increasing evidence that some associations between life course exposures and cardiovascular disease or its risk factors are epidemiological stage specific [16–18], perhaps because of epigenetic influences, making evidence from non-western settings valuable for developing effective interventions.
In developing populations birth weight, was not until recently, routinely measured and evidence concerning the association of birth weight with adult cardiovascular disease or its risk factors is mainly based on young people [18] or on small samples of inevitably atypical, hospital births with high attrition rates [18–22]. Given the long latency period following up a new cohort today could take decades to produce any evidence. In addition, associations between birth weight and cardiovascular disease or its risk factors may only be evident in adulthood or may amplify with age, making associations observed in childhood difficult to interpret.
Using birth rank as an instrumental variable for birth weight provides an alternative approach to observational studies for elucidating the contribution of birth weight to adult cardiovascular disease in general. Such an approach also provides a means of assessing the association in developing populations within a reasonable time frame. Birth rank has been observed to be consistently associated with birth weight in many different settings at various epidemiological stages [23–30]. On the other hand there is little reason to believe that birth rank is causally associated with cardiovascular disease or its risk factors [31, 32]. To clarify the association of birth weight with cardiovascular disease risk factors in general and outside of long-term developed western settings, we used birth rank as an instrumental variable in a large study of older southern Chinese.
Methods
Sources of data
The Guangzhou Biobank Cohort Study is a collaboration amongst the Guangzhou No. 12 Hospital, the Universities of Hong Kong and Birmingham, and has been described in detail [33]. Recruitment of participants draws from "The Guangzhou Health and Happiness Association for the Respectable Elders", a community social and welfare association unofficially aligned with the municipal government where membership is open to anyone aged 50 years or older for a monthly, nominal fee of 4 Yuan (50 US cents). Recruitment for phase 2 took place from April 2005 to May 2006 and for phase 3 from September 2006 to January 2008. About 7% of permanent Guangzhou residents aged 50 years and over are members of "The Guangzhou Health and Happiness Association for the Respectable Elders", of whom 22% enrolled for phase 2 or 3 recruitment, constituting 65.9% of the total recruitment, and were included if they were capable of consenting, ambulatory, and not receiving treatment modalities which if omitted may result in immediate life threatening risk, such as chemotherapy or radiotherapy for cancer, or dialysis for renal failure. Participants underwent a half-day detailed medical interview, including disease history, and physical examination. In phases 2 and 3 the questionnaire was extended to include more questions concerning the participants' early life, including the question "How many children did your mother give birth to including you? And "How many of these were older than you"? The Guangzhou Medical Ethics Committee of the Chinese Medical Association approved the study and all participants gave written, informed consent before participation.
The detailed methods of measurement have been reported [33]. In brief, standing height was measured without shoes to the nearest 0.1 centimetre. Weight was measured in light clothing to the nearest 0.1 kilogram. Hip circumference was measured at the greatest circumference round the buttocks below the iliac crest. Waist circumference was measured horizontally around the smallest circumference between the ribs and iliac crest, or at the level of the naval for obese participants. Body mass index (BMI) was calculated as the weight in kilograms divided by the square of height in metres. Seated blood pressure was recorded as the average of the last two of three measurements, using the Omron 705CP sphygmomanometer. Fasting HDL-cholesterol, triglyceride, total cholesterol and glucose levels were determined by the Shimadzu CL-8000 Clinical Chemical Analyzer.
Instrumental variable
The instrumental variable for birth weight was birth rank. We used published equations relating birth rank (of order 1 to 10+) to birth weight for 18,425 live born Chinese infants from poor families in Singapore from 1950 to 1951 [23]. This study represents 25% of all births in Singapore in the period, of which a summary is provided in Additional File 1 for easy reference. We used this source because it provides a large sample of Chinese from the relevant historic time. Moreover, the association between birth rank and birth weight is similar across populations, even though mean birth weight may differ. To illustrate this Figure 1 shows the association between birth rank and birth weight in the mid 20th century from a variety of locations, including Singapore [23–27]. In addition, we also repeated our analysis using the association between birth rank and birth weight from all these studies combined. In Singapore in the mid 20th century, the male infants were slightly heavier (mean birth weight 3.11 kilograms (kg), standard deviation (SD) 0.39) than the female infants (mean birth weight 3.03 kg, SD 0.37) [23].

Outcome measures
We examined eight biological outcome measures, typically associated with cardiovascular disease: systolic blood pressure, diastolic blood pressure, fasting plasma glucose, HDL-cholesterol, total cholesterol, triglycerides, waist-hip ratio (WHR), and body mass index (BMI). We also examined the metabolic syndrome and its components using the International Diabetes Federation definition [34], with raised blood pressure as systolic blood pressure ≥ 130 mmHg or diastolic blood pressure ≥ 85 mmHg or treatment for hypertension, reduced HDL-C as HDL cholesterol <1.03 mmol/L in men or <1.29 mmol/L in women or treatment for this specific abnormality, raised fasting plasma glucose as fasting plasma glucose ≥ 5.6 mmol/L or previously diagnosed type 2 diabetes, raised triglycerides as triglycerides >1.7 mmol/L and central obesity as waist circumference ≥ 80 cm in women or ≥ 90 cm in men. The metabolic syndrome is the presence of central obesity and any two other components [34].
Statistical analysis
We used a separate-sample instrumental variable (SSIV) estimator [35, 36]. SSIV is similar to the more common two-stage least squares method, except that each stage is calculated using separate data. The first stage used birth rank to predict birth weight by sex from published data on birth weight in Chinese infants. The second stage used the regression predictions of birth weight from the first stage as independent variables predicting cardiovascular disease risk factors. From these models we reported adjusted mean differences (Δ) or odds ratios with 95% confidence intervals (CIs) per sex-specific standard deviation higher birth weight, so as to have a comparable measure in men and women. We also examined whether the associations with birth weight varied by age and sex from the p values of the relevant interaction terms. However, it is possible that birth rank is a better instrument among men than women, because the factors potentially associated with birth rank, such as childhood socioeconomic position, are not associated with CVD risk among men in this study [37], so we also presented sex-specific results.
Potential confounders considered were study phase, age (in 5-year age-groups), life course socio-economic position (parental possessions, education and job type), lifestyle habits (ever-smoking, use of alcohol and physical activity both leisure and other), number of offspring and measures of early life experience (leg length and seated height), categorized as in Table 1.We included potential confounders on a change in estimate criteria for blood pressure, on this basis we excluded job type and lifestyle habits. We should have excluded measures of early life experiences as well on this basis, however to ensure we had adjusted for environmental differences during growth we also included leg length and seated height in one of the models. Thus, we presented four models. Model 1 adjusted for use of appropriate medication (not included when analyzing metabolic syndrome or its components), study phase, age and sex. Model 2 additionally adjusted for parental possessions and education. Model 3 additionally adjusted for number of offspring, leg length and seated height. The role of adiposity is unclear, so Model 4 additionally adjusted for BMI and WHR, where appropriate.
Results
Of the 20,086 participants, 18,958 (94.4%) had complete data on all items of interest, so we did not perform imputations. There were more women (13,907) than men (5,051), and the women were younger (mean age 59.4 (SD 7.1)) than the men (mean age 63.1 (SD 7.0)). Age ranged from 50 to 96 years, but only 457 participants were older than 75 years.
Table 1 shows potential confounders and cardiovascular risk factors by birth rank, with birth ranks 4 to 10+ combined for compactness. Among men the instrumental variable, birth rank, had little association with potential confounders such as education, job type, smoking status, alcohol use and physical activity, although higher birth rank was associated with fewer parental possessions and fewer offspring. Birth rank was also associated with height, leg length and seated height. Among women birth rank was not associated with seated height, job type, alcohol use or number of offspring, although higher birth rank was associated with fewer parental possessions, lower education, manual job, never smoking and more physical activity.
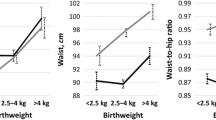
Table 2 shows that birth weight was negatively associated with blood pressure, (diastolic and systolic) but had no association with glucose, triglycerides, total cholesterol, HDL-cholesterol, waist-hip ratio, body mass index in model 2. Adjustment for number of offspring, leg length and seated height, in model 3, attenuated the association between birth weight and systolic blood pressure. Adjustment for BMI and WHR, in model 4, did not change the estimates. There was little evidence that the association of birth weight and the outcomes concerned varied with sex, except for HDL-cholesterol, where there was a positive association among women, otherwise the pattern in men and women was similar. There was no evidence that the associations varied with age (data not shown).
Table 3 shows that birth weight was negatively associated with the presence of raised blood pressure in all models but had no association with other components of the metabolic syndrome or the syndrome itself in any model. There was little evidence that the association of birth weight and metabolic syndrome or its components varied with sex, except for central obesity, where there were opposite associations by sex, although the confidence intervals included 1 for both men and women, otherwise the pattern in men and women was similar. There was no evidence that the associations varied with age (data not shown).
Repeating the analysis using the association of birth rank with birth weight from five mid 20th century studies produced similar results (Additional Files 2, 3).
Discussion
In a large study of older people from an under-studied population using a novel approach we found that higher estimated birth weight was possibly associated with lower blood pressure and in women estimated birth weight was positively associated with HDL-cholesterol, but there was no association between birth weight and other lipids, fasting glucose or the metabolic syndrome. These findings are consistent with meta-analysis indicating that birth weight may have a small effect on blood pressure [3], although most publications focus only on systolic blood pressure [3]. These findings are also fairly consistent with studies suggesting that birth weight has little clear association with lipids [6, 7], with mixed findings concerning sex-specific effects [38]. Our findings are less consistent with the association usually found between lower birth weight and diabetes [5]. However, this association is less clear outside of long-term developed western populations [18–20, 39]. As such, our study extends observations concerning the long-term effects of birth weight in largely western populations to a developing population, with the advantage of using a potentially less confounded measure of pre-natal experience. Birth weight is usually socially patterned and positively associated with adult height [40], however birth rank had relatively little social patterning. There were significant differences in birth rank by parental possessions, because of our large sample size, but the absolute differences were small.
Limitations
Despite using the instrumental variable approach to minimise confounding in a large sample in an under-studied population, there are several limitations. First, the infrastructure to facilitate fully representative cohort studies in developing countries such as China is not readily available, which could preclude evidence from a large proportion of the global developing population during a period of transition. Our findings would be biased if people with specific birth rank and cardiovascular risk factors were systematically excluded, such as first-borns with low blood pressure or later-borns with high blood pressure; we have little reason to believe this is likely. Second, survival bias is possible. If survivorship were an issue we would have expected differences in association between the older and younger age-groups, of which we found little evidence. Third, the assumptions for a valid instrument are that it should be associated with the exposure and only associated with the outcome via the exposure. It is possible that birth rank does not satisfy these assumptions in this population, despite the consistently observed association between birth rank and birth weight [23–29]. We could not verify the association between birth rank and birth weight in our cohort, because participants were largely unable to answer questions on their birth weight, probably because it had never been measured. In the current southern Chinese populations, birth rank is positively associated with birth weight [30]. The effect of birth rank on birth weight may be reduced by older brothers [41]. We did not ask about the siblings' sex; lack of this information would weaken our instrumental variable at random for which our large sample should compensate. It is also possible that birth rank may be an instrumental variable for infant growth, as well as or instead of birth weight, because infants with lower birth order often grow rapidly in the immediate post-natal period. Rapid post-natal growth is associated with cardiovascular disease risk factors [42]. We do not have infant growth rates for this cohort. However rapid infant growth is usually associated with several aspects of cardiovascular risk [42], not just blood pressure. As regards, the assumption concerning a lack of association between birth rank and potential confounders, this was more apparent among men than women. Moreover, childhood socio-economic position has little association with CVD risk among men in this population [37]. As such, birth rank may be a more suitable instrumental variable for men than women. However, the associations were similar in both sexes. We also had to use a separate sample instrumental variable approach, so we could not adjust for covariates in the prediction equation for birth weight nor could we test the strength of our instrument. We did carry out sensitivity analyses using prediction equations based on other studies and results were similar (Additional Files 2, 3).
Nevertheless, we cannot be sure of the strength of birth rank as an instrument, although we did find an association in the expected direction with blood pressure. It would be valuable, if birth rank were used an instrumental variable for birth weight in a single sample including birth rank, birth weight and cardiovascular risk factors, however we are not aware of any such analysis. Fourth, higher birth rank may be associated with poorer childhood conditions, due to a parental strategy of lower investment in each offspring, and thereby offset any benefits of higher birth weight. Parents could also pay greater attention to children of lower birth rank, however to what extent that might be relevant in a culture where children are traditionally cared for by their grandparents is difficult to assess. Moreover, there is little difference in height by birth rank (Table 1), height is not clearly associated with cardiovascular risk in this population [17], and we adjusted for several measures of early life environment (parental possessions, education, leg length and seated height). Finally, we are basing our conclusions on a set of largely null results, which could well be due to insufficiently sensitive methods, encompassing all stages of the study from fieldwork to analysis. However, we did find some of the expected associations between birth weight and cardiovascular risk, just not all of them.
Despite these limitations in our study, our findings suggest little association between birth weight and cardiovascular risk factors in a population with a recent history of economic development. Perhaps the relevant exposure(s) did not vary or foetal exposures impact blood pressure but other mechanisms, of which birth weight is a non-causal marker, underlie the commonly observed inverse association between birth weight and diabetes, such as genetic influences as in the 'foetal insulin hypothesis' [43]. Alternatively, more recent socio-biological conceptualisations of the changes in disease patterns with economic development [44] suggest that the commonly observed associations for diabetes could simply be an historical coincidence, generated by two unrelated secular trends that occur with economic development. Height increases over many generations of economic development [45], perhaps as epigenetic constraints on fetal, infant and childhood linear growth "wear off" [46, 47]. Although trends in birth weight are less well documented, height determines birth weight [48]. Birth weight has certainly increased in southern Chinese over the last 60 years [25, 30]. It is also becoming increasingly evident that sex-steroids also increase over generations of economic development [49–51], which predisposes women to breast cancer [52] and perhaps men to ischemic heart disease [37, 53, 54]. However, increasingly levels of sex-steroids over generations would also reduce vulnerability to diabetes because of the anabolic effects of sex-steroids on muscle mass [55], providing greater capacity for glucose disposal. The historical coincidence of these two separate secular trends would generate an apparent negative association between birth weight and diabetes, particularly in populations with a long history of economic development and hence heterogeneity in intra-population experience over generations. Conversely, in populations with a much more recent history of economic development and hence homogeneity of experience over generations there would be less association, as seen here and the cohorts from more recently developed populations [18–20].
Conclusion
Although, our study is only preliminary and hypothesis generating, nevertheless it has some potential implications. It suggests that the developmental origins of health paradigm needs to be extended beyond birth weight and infancy to investigate how exposures across and within generations affect cardiovascular disease risk factors, and specifically to consider that the observed associations may be a historical co-incidence. It also suggests that there may not be a common foetal development pathway determining blood pressure, diabetes and lipids, consistent with the disparate trends in sub-types of cardiovascular disease with economic development. Moreover, if confirmed it suggests that in developing countries birth weight may not be a useful intervention target.
Rather than being determined by birth weight, some of the commonly observed associations between birth weight and cardiovascular diseases may be a marker of exposures across generations or even a historical co-incidence. Future studies of birth weight and cardiovascular risk should include measures of parental and/or grandparental exposures, so that the relative contribution of inter-generational exposures and birth weight can be examined. Moreover, comparisons of maternal exposures during pregnancy across ethnicities and epidemiological stages might help identify the underlying exposures driving associations between birth weight and cardiovascular disease risk. Meanwhile caution should be exercised in extrapolating observational studies from long-term developed populations to other settings.
References
Barker DJ, Winter PD, Osmond C, Margetts B, Simmonds SJ: Weight in infancy and death from ischaemic heart disease. Lancet. 1989, 2: 577-580. 10.1016/S0140-6736(89)90710-1.
Gluckman PD, Hanson MA, Cooper C, Thornburg KL: Effect of in utero and early-life conditions on adult health and disease. N Engl J Med. 2008, 359: 61-73. 10.1056/NEJMra0708473.
Huxley R, Neil A, Collins R: Unravelling the fetal origins hypothesis: is there really an inverse association between birthweight and subsequent blood pressure?. Lancet. 2002, 360: 659-665. 10.1016/S0140-6736(02)09834-3.
Harder T, Rodekamp E, Schellong K, Dudenhausen JW, Plagemann A: Birth weight and subsequent risk of type 2 diabetes: a meta-analysis. Am J Epidemiol. 2007, 165: 849-857. 10.1093/aje/kwk071.
Whincup PH, Kaye SJ, Owen CG, Huxley R, Cook DG, Anazawa S, Barrett-Connor E, Bhargava SK, Birgisdottir BE, Carlsson S, de Rooij Sr, Dyck RF, Eriksson JG, Falkner B, Fall C, Forsen T, Grill V, Gudnason V, Hulman S, Hypponen E, Jeffreys M, Lawlor DA, Leon DA, Minami J, Mishra G, Osmond C, Power C, Rich-Edwards JW, Roseboom TJ, et al: Birth weight and risk of type 2 diabetes: a systematic review. JAMA. 2008, 300: 2886-2897. 10.1001/jama.2008.886.
Lauren L, Jarvelin MR, Elliott P, Sovio U, Spellman A, McCarthy M, Emmett P, Rogers I, Hartikainen AL, Pouta A, Hardy R, Wadsworth M, Helmsdal G, Olsen S, Bakoula C, Lekea V, Millwood I: Relationship between birthweight and blood lipid concentrations in later life: evidence from the existing literature. Int J Epidemiol. 2003, 32: 862-876. 10.1093/ije/dyg201.
Huxley R, Owen CG, Whincup PH, Cook DG, Colman S, Collins R: Birth weight and subsequent cholesterol levels: exploration of the "fetal origins" hypothesis. JAMA. 2004, 292: 2755-2764. 10.1001/jama.292.22.2755.
Simeoni U, Barker DJ: Offspring of diabetic pregnancy: long-term outcomes. Semin Fetal Neonatal Med. 2009, 14: 119-124. 10.1016/j.siny.2009.01.002.
Catalano PM, Thomas A, Huston-Presley L, Amini SB: Increased fetal adiposity: a very sensitive marker of abnormal in utero development. Am J Obstet Gynecol. 2003, 189: 1698-1704. 10.1016/S0002-9378(03)00828-7.
Voigt M, Heineck G, Hesse V: The relationship between maternal characteristics, birth weight and pre-term delivery: evidence from Germany at the end of the 20th century. Econ Hum Biol. 2004, 2: 265-280. 10.1016/j.ehb.2004.04.005.
Joseph KS, Kramer MS: Should we intervene to improve fetal and infant growth?. A life course approach to chronic disease epidemiology. Edited by: Kuh D, Ben-Shlomo Y. 2004, Oxford: OUP, 399-414.
Hawkesworth S: Conference on "Multidisciplinary approaches to nutritional problems". Postgraduate Symposium. Exploiting dietary supplementation trials to assess the impact of the prenatal environment on CVD risk. Proc Nutr Soc. 2009, 68: 78-88. 10.1017/S0029665108008781.
McMullen S, Mostyn A: Animal models for the study of the developmental origins of health and disease. Proc Nutr Soc. 2009, 68: 306-320. 10.1017/S0029665109001396.
Schwartz R, Susa J: Fetal macrosomia--animal models. Diabetes Care. 1980, 3: 430-432. 10.2337/diacare.3.3.430.
Aerts L, Van Assche FA: Animal evidence for the transgenerational development of diabetes mellitus. Int J Biochem Cell Biol. 2006, 38: 894-903. 10.1016/j.biocel.2005.07.006.
Ezeamama AE, Viali S, Tuitele J, McGarvey ST: The influence of socioeconomic factors on cardiovascular disease risk factors in the context of economic development in the Samoan archipelago. Soc Sci Med. 2006, 63: 2533-2545. 10.1016/j.socscimed.2006.06.023.
Schooling CM, Jiang C, Lam TH, Thomas GN, Heys M, Lao X, Zhang W, Adab P, Cheng KK, Leung GM: Height, its components and cardiovascular risk in older Chinese: a cross-sectional analysis of The Guangzhou Biobank Cohort Study. Am J Public Health. 2007, 18: 1834-1841. 10.2105/AJPH.2006.088096.
Victora CG, Adair L, Fall C, Hallal PC, Martorell R, Richter L, Sachdev HS: Maternal and child undernutrition: consequences for adult health and human capital. Lancet. 2008, 371: 340-357. 10.1016/S0140-6736(07)61692-4.
Fall CH, Stein CE, Kumaran K, Cox V, Osmond C, Barker DJ, Hales CN: Size at birth, maternal weight, and type 2 diabetes in South India. Diabet Med. 1998, 15: 220-227. 10.1002/(SICI)1096-9136(199803)15:3<220::AID-DIA544>3.0.CO;2-O.
Fall CH, Sachdev HS, Osmond C, Lakshmy R, Biswas SD, Prabhakaran D, Tandon N, Ramji S, Reddy KS, Barker DJ, Bhargava SK: Adult metabolic syndrome and impaired glucose tolerance are associated with different patterns of BMI gain during infancy: Data from the New Delhi Birth Cohort. Diabetes Care. 2008, 31: 2349-2356. 10.2337/dc08-0911.
Xiao X, Zhang ZX, Cohen HJ, Wang H, Li W, Wang T, Xu T, Liu A, Gai MY, Ying S, Schmitz O, Yi Z: Evidence of a relationship between infant birth weight and later diabetes and impaired glucose regulation in a Chinese population. Diabetes Care. 2008, 31: 483-487. 10.2337/dc07-1130.
Cheung YB, Low L, Osmond C, Barker D, Karlberg J: Fetal growth and early postnatal growth are related to blood pressure in adults. Hypertension. 2000, 36: 795-800.
Millis J, Seng YP: The effect of age and parity of the mother on birth weight of the offspring. Ann Hum Genet. 1954, 19: 58-73. 10.1111/j.1469-1809.1954.tb01263.x.
Roberts DF, Tanner RE: Effects of parity on birth weight and other variables in a Tanganyika Bantu sample. Br J Prev Soc Med. 1963, 17: 209-15.
Uttley KH: The birth weight of full term Cantonese babies. Chinese Medical Journal. 1940, 58: 585-591.
Fraccaro M: A contribution to the study of birth weight based on an Italian sample. Ann Hum Genet. 1956, 20: 297-
Namboodiri NK, Balakrishnan V: On the effect of maternal age and parity on the birth weight of the offspring (Indian infants). Ann Hum Genet. 1959, 23: 189-203. 10.1111/j.1469-1809.1959.tb01463.x.
Magnus P, Berg K, Bjerkedal T: The association of parity and birth weight: testing the sensitization hypothesis. Early Hum Dev. 1985, 12: 49-54. 10.1016/0378-3782(85)90136-7.
Juntunen KS, Laara EM, Kauppila AJ: Grand grand multiparity and birth weight. Obstet Gynecol. 1997, 90: 495-499. 10.1016/S0029-7844(97)00269-X.
Cheung YB, Yip PS: Social patterns of birth weight in Hong Kong, 1984-1997. Soc Sci Med. 2001, 52: 1135-1141. 10.1016/S0277-9536(00)00228-8.
Paffenbarger RS, Thorne MC, Wing AL: Chronic disease in former college students. VIII. Characteristics in youth predisposing to hypertension in later years. Am J Epidemiol. 1968, 88: 25-32.
Higgins M, Keller J, Moore F, Ostrander L, Metzner H, Stock L: Studies of blood pressure in Tecumseh, Michigan. I. Blood pressure in young people and its relationship to personal and familial characteristics and complications of pregnancy in mothers. Am J Epidemiol. 1980, 111: 142-155.
Jiang C, Thomas GN, Lam TH, Schooling CM, Zhang W, Lao X, Adab P, Liu B, Leung GM, Cheng KK: Cohort profile: The Guangzhou Biobank Cohort Study, a Guangzhou-Hong Kong-Birmingham collaboration. Int J Epidemiol. 2006, 35: 844-852. 10.1093/ije/dyl131.
Alberti KG, Zimmet P, Shaw J: The metabolic syndrome--a new worldwide definition. Lancet. 2005, 366: 1059-1062. 10.1016/S0140-6736(05)67402-8.
Dee TS, Evans WN: Teen drinking and educational attainment: evidence from two-sample instrumental variables estimates. J Labor Econ. 2003, 21: 178-209. 10.1086/344127.
Angrist JD, Krueger AB: The effect of age at school entry on educational-attainment - an application of instrumental variables with moments from 2 samples. J Am Statist Assoc. 1992, 87: 336-10.2307/2290263.
Schooling CM, Jiang CQ, Lam T.H, Zhang W, Cheng KK, Leung GM: Life-Course Origins of Social Inequalities in Metabolic risk in the Population of a Developing Country. AJE. 2008, 167: 419-428. 10.1093/aje/kwm329.
Cooper R, Power C: Sex differences in the associations between birthweight and lipid levels in middle-age: findings from the 1958 British birth cohort. Atherosclerosis. 2008, 200: 141-149. 10.1016/j.atherosclerosis.2007.11.011.
Tian JY, Cheng Q, Song XM, Li G, Jiang GX, Gu YY, Luo M: Birth weight and risk of type 2 diabetes, abdominal obesity and hypertension among Chinese adults. Eur J Endocrinol. 2006, 155: 601-607. 10.1530/eje.1.02265.
Li L, Dangour AD, Power C: Early life influences on adult leg and trunk length in the 1958 British birth cohort. Am J Hum Biol. 2007, 19: 836-843. 10.1002/ajhb.20649.
Nielsen HS, Mortensen L, Nygaard U, Schnor O, Christiansen OB, Andersen AM: Brothers and reduction of the birth weight of later-born siblings. Am J Epidemiol. 2008, 167: 480-484. 10.1093/aje/kwm330.
Singhal A, Lucas A: Early origins of cardiovascular disease: is there a unifying hypothesis?. Lancet. 2004, 363: 1642-1645. 10.1016/S0140-6736(04)16210-7.
Hattersley AT, Tooke JE: The fetal insulin hypothesis: an alternative explanation of the association of low birthweight with diabetes and vascular disease. Lancet. 1999, 353: 1789-1792. 10.1016/S0140-6736(98)07546-1.
Schooling CM, Leung GM: A socio-biological explanation for social disparities in non-communicable chronic diseases - the product of history?. JECH. 2010, DOI 1011 36/jech.2008.086553
Cole TJ: The secular trend in human physical growth: a biological view. Econ Hum Biol. 2003, 1: 161-168. 10.1016/S1570-677X(02)00033-3.
Schooling CM, Jiang C, Heys M, Zhang W, Lao X, Adab P, Cowling B.J, Thomas GN, Cheng KK, Leung GM: Is leg length a biomarker of childhood conditions in older Chinese women? The Guangzhou Biobank Cohort Study. JECH. 2008, 62: 160-167.
Schooling CM, Jiang CQ, Heys M, Zhang W, Adab P, Cheng KK, Lam T.H, Leung GM: Are height and leg length universal markers of childhood conditions? The Guangzhou Biobank Cohort Study. JECH. 2008, 62: 607-614.
Barron SL: The epidemiology of human pregnancy. Proc R Soc Med. 1968, 61: 1200-1206.
Ellison PT, Bribiescas RG, Bentley GR, Campbell BC, Lipson SF, Panter-Brick C, Hill K: Population variation in age-related decline in male salivary testosterone. Hum Reprod. 2002, 17: 3251-3253. 10.1093/humrep/17.12.3251.
Ellison PT: Salivary steroids and natural variation in human ovarian function. Ann N Y Acad Sci. 1994, 709: 287-98. 10.1111/j.1749-6632.1994.tb30417.x.
Nunez-de la MA, Chatterton RT, Choudhury OA, Napolitano DA, Bentley GR: Childhood conditions influence adult progesterone levels. PLoS Med. 2007, 4: e167-10.1371/journal.pmed.0040167.
Trichopoulos D: Hypothesis: does breast cancer originate in utero?. Lancet. 1990, 335: 939-940. 10.1016/0140-6736(90)91000-Z.
Schooling CM, Lam TH, Ho SY, Mak KH, Leung GM: Does economic development contribute to sex differences in ischaemic heart disease mortality? Hong Kong as a natural experiment using a case-control study. BMC Public Health. 2008, 8: 10.1186/1471-2458-8-32.
Chung RY, Schooling CM, Cowling B.J, Leung GM: How does socioeconomic development affect risk of mortality? An age-period-cohort analysis from a recently transitioned population in China. AJE. 2010, 171: 345-356. 10.1093/aje/kwp378.
Schooling CM, Jiang CQ, Zhang WS, Lam TH, Cheng KK, Leung GM: Visceral adiposity would be expected to predict incident diabetes better in women than men. Diabetologia. 2010, 53: 393-395. 10.1007/s00125-009-1613-3.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2458/10/270/prepub
Acknowledgements
The Guangzhou Cohort Study investigators include: Guangzhou No. 12 Hospital: XQ Lao, WS Zhang, M Cao, T Zhu, B Liu, CQ Jiang (Co-PI); The University of Hong Kong: CM Schooling, SM McGhee, R Fielding, GM Leung, TH Lam (Co-PI); The University of Birmingham: P Adab, GN Thomas, Y Peng, KK Cheng (Co-PI). We would also like to thank Prof. Sir R Peto and Dr ZM Chen of the Clinical Trial Service Unit, The University of Oxford for their support.
The work was supported by The University of Hong Kong Foundation for Development and Research, and the University of Hong Kong University Research Committee Strategic Research Theme Public Health, Hong Kong; Guangzhou Public Health Bureau, and Guangzhou Science and Technology Bureau, Guangzhou, China; and The University of Birmingham, UK. The funding sources had no role in any of the following: study design; the collection, analysis, and interpretation of data; the writing of the report; and the decision to submit the paper for publication.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
CMS originated the idea, designed this analysis, interpreted the results and wrote the first draft, with the help of GML, SLAY and BJC. SLAY revised the analysis and edited the manuscript. THL, KKC, CQJ designed the original study and acquired the data with the help of WSZ. All authors revised the manuscript critically for important intellectual content; and gave final approval of the version to be submitted.
Electronic supplementary material
12889_2010_2181_MOESM1_ESM.DOC
Additional file 1: Supplemental tables. Published data concerning birth rank and birth weight extracted for easy reference from a report from Singapore in 1951/2[23] Table S1.1: Infant birth weight by birth rank and sex Table S1.2: Equation and coefficients to predict birth weight from birth rank. (DOC 38 KB)
12889_2010_2181_MOESM2_ESM.DOC
Additional file 2: Instrumental variable estimates for the effect per birth weight standard deviation on cardiovascular disease risk factors in 18,958 older Chinese men and women in phases 2 and 3 of the Guangzhou Biobank Cohort Study (2005-8), based on 5 mid 20th century studies[23–27] of birth rank and birth weight. (DOC 54 KB)
12889_2010_2181_MOESM3_ESM.DOC
Additional file 3: Instrumental variable estimates (odds ratio) for the effect per birth weight standard deviation on cardiovascular disease risk factors in 18,958 older Chinese men and women in phases 2 and 3 of the Guangzhou Biobank Cohort Study (2005-8), based on 5 mid 20th century studies[23–27] of birth rank and birth weight. (DOC 47 KB)
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Schooling, C., Jiang, C., Lam, T. et al. Estimated birth weight and adult cardiovascular risk factors in a developing southern Chinese population: a cross sectional study. BMC Public Health 10, 270 (2010). https://doi.org/10.1186/1471-2458-10-270
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2458-10-270