
Abstract
Background
We investigated our translation of The Mood Disorder Questionnaire (MDQ) as a screening instrument for bipolar disorder in a psychiatric setting in Finland.
Methods
In a pilot study for the Jorvi Bipolar Study (JoBS), 109 consecutive non-schizophrenic psychiatric out- and inpatients in Espoo, Finland, were screened for bipolar disorder using the Finnish translation of the MDQ, and 38 of them diagnostically interviewed with the SCID.
Results
Forty subjects (37%) were positive in the MDQ screen. In the SCID interview, twenty patients were found to suffer from bipolar disorder, of whom seven (70%) of ten patients with bipolar I but only two (20%) of ten with bipolar II disorder had been previously clinically correctly diagnosed. The translated MDQ was found internally consistent (alpha 0.79) and a feasible screening tool.
Conclusions
Bipolar disorder, particularly type II, remains commonly unrecognized in psychiatric settings. The Mood Disorder Questionnaire is a feasible screen for bipolar disorder, which could well be integrated into psychiatric routine practice.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Although bipolar disorder is a major public health issue, it is commonly unrecognized even in psychiatric settings [1, 2]. Feasible screening instruments are needed to improve recognition and diagnosis of the various forms of the illness. The Mood Disorder Questionnaire [3] is a recently developed and simple screening method already validated in a US multicenter study. The instrument was found to have relatively good sensitivity (0.73) and very good specificity (0.90) in samples comprising mostly patients with uni- and bipolar mood disorders in academic centers [3]; in a further general population study the sensitivity turned out to be very low (0.28), but specificity (0.97) remarkably high [4]. The instrument has so far been little investigated by others than its developers.
In the present pilot study, using our Finnish translation of the Mood Disorder Questionnaire among unselected psychiatric patients, we investigated its psychometric and screening properties, and its feasibility in improving recognition of type I and II bipolar disorder.
Methods
The present investigation was a pilot study for the ongoing Jorvi Bipolar Study (JoBS). The screening for bipolar disorder was conducted at the Department of Psychiatry at Jorvi Hospital, part of the Helsinki University Central Hospital, from 1st–31st October, 2001. The Department has a catchment area of approximately 250 000 inhabitants, but this pilot study was conducted only in two selected community mental health centres (Leppävaara and Kirkkonummi), and in the psychiatric outpatient clinic of Jorvi Hospital and three of its psychiatric wards. The whole JoBS project has been evaluated and accepted in the Ethics Committee of the Helsinki and Uusimaa Hospital District, and it complies with the principles of the Helsinki Declaration.
Three patient groups were screened: (a) all new patients who were referred to treatment in the Department of Psychiatry; (b) all patients who had earlier received treatment in the Department, but now had a new referral, and (c) those already in contact with the facilities, without a clinical diagnosis of ICD-10 schizophrenia, and now showing signs of deteriorating clinical state after at least two months of limited or no symptoms. The aim was to include all incident episodes of bipolar disorder among patients receiving treatment.
The Mood Disorder Questionnaire [3] is a short self-report screening instrument, and was translated into Finnish by the authors. The first question includes 13 items, symptoms or behaviors related to a manic or hypomanic syndrome. The second question asks whether several of the symptoms have been experienced during the same time period, and the third asks about resulting problems, classified as minor, moderate or serious. The screen is regarded positive when seven or more positive symptoms have occurred, several within the same episode, causing moderate to severe problems. If the MDQ was negative, the attending professional was also asked whether bipolar disorder might be present despite a negative screen (clinical suspicion).
All patients with a positive screen or clinically suspected of having bipolar disorder were invited to be interviewed with the Structured Clinical Interview for DSM-IV Axis I Disorders, Clinician Version, SCID-CV [5]. In addition, a systematic sample of every third patient with 4–6 positive items in question 1 of the MDQ was drawn from each setting. All interviewers were either psychiatrists or residents with several years experience in psychiatry and relevant training. The first two authors supervised the diagnostic process.
Results
Screening phase
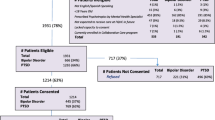
The group of eligible patients comprised 113 subjects, of whom two (2%) refused and two (2%) were excluded because of not speaking Finnish. Altogether 109 (96%) patients were screened. Their mean age was 37.9 ± 11.4 years, and 56 (51%) were female. Forty subjects (37%) were positive in the MDQ. Twenty-nine (27%) subjects had negative MDQ but 4–6 positive items in question 1. This latter group included four of the five subjects (5% of the total) with negative MDQ who were clinically suspected of possibly suffering from bipolar disorder.
The frequency of positive responses to the various symptom items of question 1 ranged from 27% (more social) to 74% (racing thoughts). In the vast majority of those reporting seven or more items, several symptoms had occurred within the same time period (in 87%), and moderate to serious problems were present (in 91%). The internal consistency of the translated instrument was found to be good (Cronbach's alpha 0.79).
Diagnostic findings
Of those eligible for diagnostic interview, 38 of 51 (75%) agreed to participate. Of those interviewed, 20 (53%) were diagnosed with bipolar disorder: ten (26%, 5 males) with type I and ten (26%, 3 males) with type II (Table 1). The mean ages of the two groups were 38.2 ± 8.0 years and 39.1 ± 12.5 years, respectively. Using the SCID-interview as the gold standard, the MDQ screening produced 9 false positives (5 patients with unipolar MDD; one schizoaffective, brief psychotic, and personality disorders; plus an amphetamine-induced psychosis) and three false negative patients (one type I with < 7 acknowledged items, one type II patient with only minor problems due to hypomania, and one type II with both). Less than half of those diagnosed with bipolar disorder in the SCID interview had had a ICD-10 diagnosis of bipolar disorder, mania or hypomania, or bipolar schizoaffective disorders before the interview. Of the bipolar I patients seven (70%) had a relevant diagnosis before the interview, compared to only two of the bipolar II patients (20%). Despite the small sample size, the difference approached statistical significance (Fisher's exact test, p = 0.07).
The properties of the MDQ as a screen within the diagnostically interviewed sample
In the ROC-analysis (Table 2, Additional file: 1) with the standard cut-offs, sensitivity emerged as high (0.85), but specificity only moderate (0.47). However, the optimal cut-off within this sample was found to be eight symptoms but accepting also minor problems due to episodes (sensitivity 0.90, specificity 0.59). Ignoring severity of problems caused (question three) altogether resulted in very low specificity.
Discussion
We found the Mood Disorder Questionnaire to be a feasible method for improving recognition of bipolar disorder, which has clearly been a problem. However, by definition, hypomania involves no marked impairment. Whether necessitating moderate to severe problems to be caused by it is useful in screening should be further investigated. Having minor problems might be enough.
This was a pilot study for the current Jorvi Bipolar Study (JoBS). Several methodological limitations should be noted, some suggesting caution in interpreting the findings. The sample of patients screened with the Mood Disorder Questionnaire was not large (N = 109), albeit probably representative of psychiatric in- and outpatients in the area. The number of patients interviewed with SCID was relatively small. Those interviewed with SCID were not a random sample of all patients screened, but a sample of cases suspected of having bipolar disorder on the basis of the finding in the MDQ, or other clinical factors. The screen thus influenced whether a diagnostic interview was conducted. It is therefore clear that the ROC-analysis overestimated sensitivity and underestimated specificity, and cannot be compared with respective estimates from unselected samples [3]. It only shows that within this sample, the optimal cut-offs would have been different. Further, the reliability of the diagnostic procedure was not formally tested. Finally, the generalizability of our findings within Finland, or to other countries, is not known. Given the relatively good resources and interest in bipolar disorder in the Jorvi psychiatric facilities, we expect recognition to be at least not worse than elsewhere in Finland. Our finding of underrecognition is comparable with those from other countries [6–10].
The Mood Disorder Questionnaire appears to be a feasible method for improving the recognition of bipolar disorder. The internal consistency of the translated instrument was almost as good (Cronbach's alpha 0.79 vs. 0.90) as in the original validation study [3]. Our study population was not a selected sample of patients with mood disorders, but rather an ordinary sample of secondary care psychiatric patients, schizophrenia excluded. Nevertheless, our prevalences of positive items (27–74% vs. 34–77%) and bipolar disorder (53% vs. 55%) were similar to the original validation study figures, although the proportion of type II disorder was higher (50% vs. 24%) in ours. In the third published study of the MDQ [11] that focused on its factor structure, rates of positive items were convergent, although slightly lower (12–65%) among private practice mood disorder patients.
The most important public health problem related to bipolar disorder is the remarkable proportion of patients who have unrecognised bipolar II disorder [6–10]. The majority of unrecognised patients in our sample, too, had bipolar II disorder. It is therefore vital that the MDQ is also sensitive to bipolar II. Hypomania, as defined in the DSM-IV, must not be related to marked impairment [12]. Thus the last question in the MDQ, necessitating moderate to severe problems due to episodes, appears to have a higher threshold for impairment. In our diagnosed sample, accepting minor impairment too, but necessitating eight symptoms, was found to be the optimal cut-off. Nevertheless, even using the standard cut-offs several patients with previously unrecognised bipolar II disorders were identified, and in fact, ignoring the last question completely resulted in lower specificity. It is to be noted that our findings are based only on ten bipolar II patients and an enriched subsample of patients with bipolar disorder. We suggest that the optimal cut-offs for bipolar II disorders should be further investigated in larger and representative patient samples.
Conclusions
The Mood Disorder Questionnaire seems to be a feasible method for improving the recognition of bipolar disorder. Whether screening is actually beneficial is related to the quality of current routine diagnostic procedures. It is useful in psychiatric settings only if recognition without it is a problem, which according to our findings is certainly true. The proportion of previously unrecognised cases was particularly high in bipolar II disorders, only a few of whom had previously received the correct diagnosis. Our findings support the value and feasibility of screening for bipolar disorder with the MDQ in psychiatric settings.
References
Hirschfeld RMA, Lewis LL, Vornik LA: Perceptions and impact of bipolar disorder: How far have we really come? The National Depressive and Manic-Depressive Association 2000 survey of individuals with bipolar disorder. J Clin Psychiatry. 2003, 64: 161-174.
Suppes T, Leverich GS, Keck PE, Nolen WA, Denicoff KD, Altshuler LL, McElroy SL, Rush AJ, Kupka R, Frye MA, Bickel M, Post RM: The Stanley Foundation Treatment Outcome Network II. Demographics and illness characteristics of the first 261 patients. J Affect Disord. 2001, 67: 45-69. 10.1016/S0165-0327(01)00432-3.
Hirschfeld RMA, Williams JBW, Spitzer RL, Calabrese JR, Flynn L, Keck PE, Flynn L, Keck PE, Lewis L, McElroy SL, Post RM, Rapport DJ, Russell JM, Sachs GM, Zajecka J: Development and validation of a screening instrument for bipolar spectrum disorder: The Mood Disorder Questionnaire. Am J Psychiatry. 2000, 157: 1873-1875. 10.1176/appi.ajp.157.11.1873.
Hirschfeld RMA, Holzer C, Calabrese JR, Weissman M, Reed M, Davies M, Frye MA, Keck P, McElroy S, Lewis L, Tierce J, Wagner KD, Hazard E: Validity of the Mood Disordr Questionnaire: A general population study. Am J Psychiatry. 2003, 160: 178-180. 10.1176/appi.ajp.160.1.178.
First MB, Spitzer RL, Gibbon M, Williams JBW: Structured Clinical Interview for DSM-IV Axis I Disorders – Clinician Version (SCID-CV). 1997, Washington, DC, American Psychiatric Press
Angst J, Felder W, Frey R, Stassen HH: The course of affective disorders: I. Change of diagnosis of monopolar, unipolar and bipolar illness. Archiv Psychiatr Nervenkr. 1978, 226: 57-64.
Cassano GB, Akiskal HS, Savino M, Musetti L, Perugi G: Proposed subtypes of bipolar II and related disorders: with hypomanic episodes (or cyclothymia) and with hyperthymic temperament. J Affect Disord. 1992, 26: 127-140. 10.1016/0165-0327(92)90044-7.
Benazzi F: Antidepressant-associated hypomania in outpatient depression: A 203-case study in private practice. J Affect Disord. 1997, 46: 73-77. 10.1016/S0165-0327(97)00082-7.
Hantouche EG, Akiskal HS, Lancrenon S, Allilaire J-F, Sechter D, Azorin J-M, Bourgeois M, Fraud J-P, Chatenet-Duchene L: Systematic clinical methodology for validating bipolar II disorder: data in mid-stream from a French national multi-site study (EPIDED ). J Affect Disord. 1998, 50: 163-173. 10.1016/S0165-0327(98)00112-8.
Ghaemi SN, Boiman EE, Goodwin FK: Diagnosing bipolar disorder and the effect of antidepressants: a naturalistic study. J Clin Psychiatry. 2000, 61: 804-08.
Benazzi F, Akiskal HS: The dual structure of self-rated MDQ hypomania: energized-activity versus irritable-thoughts racing. J Affect Disord. 2003, 73: 59-64. 10.1016/S0165-0327(02)00333-6.
American Psychiatric Association (APA): Diagnostic and Statistical Manual of Mental Disorders. Fourth Edition, Text Revision. Washington, DC, American Psychiatric Association. 2000
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-244X/3/8/prepub
Acknowledgements
The present study was supported by a research grant from the Jorvi Hospital.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
No competing interests.
Authors' contributions
EI supervised the study, analyzed the data and wrote the paper. KS supervised the fieldwork, interviewed patients, and participated in writing the paper. OM, HV, SL, MP and PA interviewed patients and commented on the manuscript. All authors participated in the translation of the Mood Disorder Questionnaire, plus read and approved the final manuscript.
Electronic supplementary material
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Isometsä, E., Suominen, K., Mantere, O. et al. The Mood Disorder Questionnaire improves recognition of bipolar disorder in psychiatric care. BMC Psychiatry 3, 8 (2003). https://doi.org/10.1186/1471-244X-3-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-244X-3-8