
Abstract
Background
Anxiety disorders are highly prevalent in primary care and cause a substantial burden of disease. Screening on risk status, followed by preventive interventions in those at risk may prevent the onset of anxiety disorders, and thereby reduce the disease burden. The willingness to participate in screening and interventions is crucial for the scope of preventive strategies, but unknown. This feasibility study, therefore, investigated participation rates of screening and preventive services for anxiety disorders in primary care, and explored reasons to refrain from screening.
Methods
In three general practices, screening was offered to individuals visiting their general practitioner (total n = 2454). To assess risk status, a 10-item questionnaire was followed by a telephone interview (including the CIDI) when scoring above a predefined threshold. Preventive services were offered to those at risk. Participation rates for screening and preventive services for anxiety disorders were assessed. Those not willing to be screened were asked for their main reason to refrain from screening.
Results
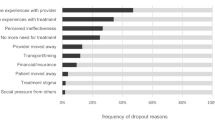
Of all individuals, 17.3% participated in initial screening, and of those with a possible risk status, 56.0% continued screening. In 30.1% of those assessed, a risk status to develop an anxiety disorder was verified. Of these, 22.6% already received some form of mental health treatment and 38.7% of them agreed to participate in a preventive intervention and were referred. The most frequently mentioned reasons to refrain from screening were the emotional burden associated with elevated risk status, the assumption not to be at risk, and a lack of motivation to act upon an elevated risk status by using preventive services.
Conclusions
Screening in general practice, followed by offering services to prevent anxiety disorders in those at risk did not appear to be a feasible strategy due to low participation rates. To enable the development of feasible and cost-effective preventive strategies, exploring the reasons of low participation rates, considering involving general practitioners in preventive strategies, and looking at preventive strategies in somatic health care with proven feasibility may be helpful.
Similar content being viewed by others

Background
Anxiety disorders are prevalent, often have a chronic course, and are associated with functional limitations. Given these features, preventing the development of anxiety disorders seems a good strategy. Hence, screening of individuals on risk factors and early stages of the disorder offers the opportunity to provide preventive interventions, and thereby limit the disease burden for both the individual and the society.
Some decades ago, Wilson and Jungner identified criteria defining situations in which screening on risk factors and early stages of the disorder is appropriate [1](Table 1). Based on these criteria, screening on risk factors and subclinical anxiety is indeed warranted. First, anxiety disorders are one of the most common psychiatric disorders with a lifetime prevalence of approximately 20% [2–4] and an annual incidence rate of 3% among adults [5]. They are regarded an important health problem [4, 6] given their often chronic course [7] and functional limitations [6, 8, 9]. Related to their chronic course, comorbid disorders often occur [10], thereby negatively impacting on the outcome. Second, effective preventive interventions based on cognitive behavioural treatments are available [11–16]. It is plausible that these interventions are acceptable for those at risk because interventions are not associated with any hazard and can be provided according to the individuals’ preference, i.e. in an individual format, a group intervention or a format using the internet. Third, screening implies that risk factors for anxiety disorders are known and can be assessed accurately. Previously, we defined target groups for the prevention of anxiety disorders, in which the largest public health benefit for the lowest effort can be achieved [17]. These target groups consist of individuals 1) with a (subthreshold) panic attack in the past year, 2) with an affective disorder in the past year, or 3) with a history of anxiety disorders combined with low mastery. These target group characteristics can be assessed relatively simple and without any risks involved, i.e. by a self report questionnaire and a telephone interview. Given the substantial costs associated with anxiety disorders [18], case-finding and subsequent treatment may well be cost-effective.
Given the assessment criteria, screening on high risk groups for the development of anxiety disorders is thus both appropriate and possible. However, the level of willingness of primary care patients to participate in screening and in interventions to prevent anxiety disorders is unknown. It is imaginable that some individuals refrain from screening because the knowledge of being at risk may be emotionally stressful. Likewise, using preventive services implicates not only time investment, but also a continuous confrontation with being at risk. In addition, in individuals visiting primary care, prevention of anxiety disorders may not be on their (somatic) agenda. Participation in screening and preventive interventions is crucial with regard to the population health benefit that can be achieved by preventive strategies, and with regard to the cost-effectivity of such strategies. Given the importance of participation rates for large scale implementation of preventive strategies, we conducted a study assessing the willingness of individuals for screening and preventive interventions in primary care.
In three general practices, screening was offered to patients visiting their general practitioner (irrespective of the reason for their visit). When risk status appeared present, a preventive intervention of their choice was offered. We investigated the proportion of individuals willing to be screened, and the proportion willing to accept a preventive intervention in those at risk.
Methods
In 2010 and 2011, we consecutively offered screening in three general practices located in Amsterdam, Leiden and Almere, thereby covering different regional parts of the Netherlands. Screening was offered free of charge to any individual between 18 and 65 years old who spoke sufficiently Dutch when visiting their general practitioner, irrespective of the reason of their visit. Trained research assistants offered a package to all visitors, including an information letter, the question whether they were willing to be screened for their risk status to develop an anxiety disorder in the oncoming year, a few questions regarding socio-demographics, and the initial screening questions. Individuals could either fill in the questions directly while waiting, or could fill them in at home and return the package in a postage-paid envelope.
The information letter included information about the frequent occurrence of anxiety disorders, the availability of effective preventive interventions, the possibility to assess their risk status, and the procedure.
The research proposal has been approved by the Ethical Review Board of VU-University Medical Center. The Ethical Review Board concluded that, given that the research used fully disidentified data only, informed consent was not required. The information letter provided to all potential participants described that disidentified data would be used to assess the willingness for screening and interventions to prevent anxiety disorders.
If patients refrained from screening, they were asked to provide several socio-demographic characteristics (gender, age, education), and were asked to report the reason of their refusal. If patients agreed to be screened, questions regarding social-demographics were followed by 10 screening questions. These aimed to identify those high-risk groups for the development of anxiety disorders we mentioned in the introduction: individuals 1) with a (subthreshold) panic attack in the past year, 2) with an affective disorder in the past year, or 3) with a history of anxiety disorders combined with low mastery [17]. To screen for panic attacks and affective disorder, we used screening questions regarding panic and depressive mood from the Web-based Screening Questionnaire (WSQ;[19]). The WSQ is a questionnaire screening for the presence of common mental disorders. Symptoms during the past year were included. Validated cut-off scores of the WSQ were used. To screen for anxiety disorders in the past, two questions were formulated. The first asked for anxiety problems in the past, the second whether these anxiety problems had resulted in limited functioning or suffering or had resulted in seeking treatment. Finally, mastery was assessed using an adapted version of the Mastery Scale [20], including 5 items. The total score provides information about the degree of control one assumes to have over his life. In correspondence with previous research [17, 21], low mastery was defined as a score lower than or equal to 18. A possible high risk status was regarded present if individuals reported positively on 1) the screening question of panic attacks, or 2) the screening question on depressive mood, or 3) on the questions regarding anxiety problems in the past that had resulted in limited functioning or suffering or for which treatment was indicated, combined with low mastery.
If a high risk status was absent, individuals were informed per email or per post (depending on their preference). It was thereby mentioned that the future onset of an anxiety disorder could not be ruled out based on a screening. Individuals scoring positively on the initial screening questions were regarded as having a possible high risk status because the screening questions provide insufficient assurance of a proper selection of people at high risk for two reasons. First, based on a screening question the presence of a fully developed anxiety disorder cannot be ruled out. Second, there is a risk of false positives because the WSQ is over inclusive [19].
In individuals with a possible high risk status, initial screening questions were therefore followed by a telephone interview. These individuals were, therefore contacted within two weeks. If necessary, individuals were contacted at different times a day up till at least five times by telephone, and once by post. A psychologist conducted the telephone interview, consisting of the section on anxiety disorders (past year and lifetime), and on depressive disorders (past year only) of the Composite International Diagnostic Interview (CIDI), version 2.1 [22]. The CIDI is a valid and reliable instrument to diagnose psychiatric disorders and can be conducted by trained lay interviewers [23]. If the interview verified the high-risk status (and verified the absence of a fully developed anxiety disorder), a suitable preventive intervention was offered. This could either be assisted self help, internet interventions, a group intervention, or regular treatment for a depressive disorder.
Results
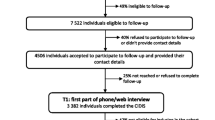
In 2010 and 2011, screening was offered to 2536 individuals visiting their general practitioner, (see Figure 1), 1500 in Amsterdam, 403 in Leiden and 633 in Almere. When screening had been offered to the majority of individuals visiting their general practitioner, screening was ended. Forty-three individuals reported to have been diagnosed with an anxiety disorder. In addition, 39 individuals mistakenly received the package but were excluded later based on age limits or language problems. The target population for screening thus consisted of 2454 individuals.

Flowchart screening.
Of these 2454, 424 individuals (17.3%) completed the questionnaire. This proportion differed significantly between the three general practitioners offices: 14.6% in Amsterdam, 21.5% in Leiden en 21.1% in Almere (X 2 (df = 2) = 18.42; p < 0.001). Of those screened, 63.9% was female, 34.4% male (1.7% missing data), the mean age was 40.5 years (SD 14.0 years)(0.5% missing data); 4.5% only had basic education, 55.9% secondary general education or intermediate vocational education, and 37.8% had higher vocational or scientific education (1.9% missing data).
The other 2030 individuals either explicitly refused to be screened (‘explicit refusers’; n = 861) or did not return the questionnaire (‘implicit refusers’; n = 1169).
Socio-demographic characteristics were provided by 23.4% (n = 468) of all refusers.
Age, gender and educational level did not differ significantly between these refusers and those who completed the screening questionnaire (gender p = 0.31; age p = 0.25; education p = 0.45). In addition, 25.7% (n = 522) provided information about the reason to refuse screening, see Table 2. The most important reasons to refrain from screening were a lack of motivation for preventive interventions (34.9%), emotional burden associated with the presence of a risk status (19.7%), and not considering themselves at risk (17.8%).
Of the 424 individuals who completed the questionnaire, 43.4% (n = 184) scored positively on the initial screening, and were therefore eligible for further screening by a telephone interview, administered to 56.0% (n = 103). The remaining individuals either refused further screening (40.2%; n = 74) or could not be reached (3.8%; n = 7).
Of the 103 individuals who completed the telephone interview with the CIDI-sections anxiety and depression, 29.1% (n = 30) already fulfilled criteria of an anxiety disorder, and were advised to seek regular treatment. In 40.8% (n = 42) a heightened risk status could not be verified, and in the remaining 30.1% (n = 31) a risk status for the onset of anxiety disorders was present. The most commonly diagnosed target group for prevention consisted of depressive disorders. Of those with a verified risk status, 22.6% already received mental health treatment, 38.7% refused psychiatric treatment despite the verified risk status and a similar proportion expressed willingness for an intervention and was referred (Figure 1).
Discussion
In theory, the prevention of anxiety disorders appears a good strategy to diminish the burden of disease because anxiety disorders are prevalent and severe, screening on risk status can be conducted safely and effective preventive interventions are available. Moreover, screening for mental disorders has been successfully provided by trained lay interviewers [24]. Such a procedure may limit costs for screening. The importance that individuals attach to prevention, and their willingness to participate in screening and preventive interventions, is unknown. Yet, participation rates in both screening and preventive interventions impact on the disease burden that can be prevented, and on the cost-effectivity of preventive strategies. In the current study the participation rates of screening and preventive interventions with regard to anxiety disorders were assessed by offering screening to 2454 individuals of three general practices, and by offering preventive interventions to those at risk.
We may conclude that the feasibility of the prevention of anxiety disorders in primary care was poor: only a minority of the target population was willing to be screened: 17.3% for initial screening, and of those with a possible risk status 56.0% was motivated for further screening. Of those with a verified risk status, some already received mental health treatment, and some were not motivated to undergo treatment despite the knowledge of being at risk. Thus, offering screening to a large number of individuals resulted in providing preventive interventions in only a few individuals.
To our knowledge, participation rates in screening and interventions aiming to prevent anxiety disorders have not been assessed before. With regard to the present study, several limitations should be taken into account. First, offering screening in only three general practices may have reduced generalizability of the findings; participation rates of screening differed significantly between these practices. However, in none of the practices participation rates were near sufficient to make screening a feasible option. Second, findings cannot be generalized to other preventive programs, because recruitment methods may impact on participation rates. Third, limited data is available about individuals who refrained from screening, because most of them did not return the screening list. As a result, other reasons to refrain from screening than those mentioned above cannot be ruled out.
Despite these limitations, findings of the present study do not stand alone, but correspond with findings regarding the prevention of depressive disorders in which only about 1% of those eligible participated in preventive interventions [25]. Cuijpers and colleagues presented an overview of possible causes of low participation rates [25] (Table 3). Some of the potential causes they describe can be ruled out in the present study: we explicitly reported on risk status thereby excluding unawareness as potential cause, we explained that preventive interventions are effective, mentioned the availability of several preventive interventions, including internet interventions which allow people to follow the intervention at their own pace, and we provided contact addresses to start an intervention of the individuals’ preference. The timing of recruiting participants may have been unsuitable in the present study as potential participants were waiting for their general practitioner to discuss another problem. However, the procedure allowed taking the questionnaire home and returning it later. Given low participation rates when recruiting in the general practitioners office, one could consider other modes of recruitment, such as recruiting participants through systematic screening in the population or via the internet. Because the general practitioner himself was not involved in recruiting participants in the present study, one could also hypothesize that endorsement by general practitioners may improve participation rates, for example, by discussing a potential stigma or by mentioning potential negative consequences of anxiety disorders, including those on cardiovascular function [26]. The two-step procedure might also have discouraged potential candidates. However, this does not seem very likely given that most individuals refrained from screening before taking notice of the procedure. In the present study, emotional burden associated with a potential risk status appeared to be the main reason to refrain from screening. This may well be related to perceived stigma. Alonso and colleagues showed that those with an anxiety disorder frequently feel embarrassed or discriminated related to their mental health [27], and Cuijpers and colleagues [25] suggested stigma as a cause of low participation rates. Other frequently reported reasons to refrain from screening were the assumption not to be at risk of developing an anxiety disorder, and a lack of motivation to use preventive services. It can be hypothesized, that lack of knowledge regarding risk factors and regarding the severity of anxiety disorders may impact upon participation rates. If so, increasing knowledge on anxiety disorders might encourage individuals to participate in screening and prevention.
Conclusions
Whereas theoretically, screening and prevention of anxiety disorders may substantially reduce the disease burden associated with anxiety disorders, the reduction of the disease burden cannot be capitalized if participation rates in screening and preventive services are low, as was found in the present study. Given the potential benefits, and given the high participation rates in some somatic screening programs such as screening for breast cancer [28], we should not refrain from further attempts to prevent the onset of anxiety disorders. To enable the development of feasible and cost-effective preventive strategies, exploring the reasons of low participation rates, considering involving general practitioners in preventive strategies, and looking at preventive strategies in somatic health care with proven feasibility may be helpful.
References
Wilson JMG, Jungner G: Principles and practice of screening for disease. 1968, Geneva: World Health Organization
Alonso J, Angermeyer MC, Bernert S, Bruffaerts R, Brugha TS, Bryson H, de Girolamo G, de Graaf R, Demyttenaere K, Gasquet I, Haro JM, Katz SJ, Kessler RC, Kovess V, Lepine JP, Ormel J, Polidori G, Russo LJ, Vilagut G, Almansa J, Rbabzadeh-Bouchez S, Autonell J, Bernal M, Buist-Bouwman MA, Codony M, Domingo-Salvany A, Ferrer M, Joo SS, Martinez-Alonso M, Matschinger H, et al: Prevalence of mental disorders in Europe: results from the European Study of the Epidemiology of Mental Disorders (ESEMeD) project. Acta Psychiatr Scand. 2004, 420 (Suppl): 21-27.
de Graaf R, ten Have M, van Gool C, van Dorsselaer S: Prevalence of mental disorders and trends from 1996 to 2009. Results from the Netherlands Mental Health Survey and Incidence Study-2. Soc Psychiatry Psychiatr Epidemiol. 2012, 47: 203-213. 10.1007/s00127-010-0334-8.
Kessler RC, Chiu WT, Demler O, Merikangas KR, Walters EE: Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005, 62: 617-627. 10.1001/archpsyc.62.6.617.
Bijl RV, de Graaf R, Ravelli A, Smit F, Vollebergh WA: Gender and age-specific first incidence of DSM-III-R psychiatric disorders in the general population. Results from the Netherlands Mental Health Survey and Incidence Study (NEMESIS). Soc Psychiatry Psychiatr Epidemiol. 2002, 37: 372-379. 10.1007/s00127-002-0566-3.
Hoeymans N, Poos MJJC, Gommer AM: Welke ziekten veroorzaken de grootste ziektelast (in DALY's)?. Volksgezondheid Toekomst Verkenning. Nationaal Kompas Volksgezondheid. 2006, Bilthoven: RIVM
Bruce SE, Yonkers KA, Otto MW, Eisen JL, Weisberg RB, Pagano M, Shea MT, Keller MB: Influence of psychiatric comorbidity on recovery and recurrence in generalized anxiety disorder, social phobia, and panic disorder: a 12-year prospective study. Am J Psychiatry. 2005, 162: 1179-1187. 10.1176/appi.ajp.162.6.1179.
Alonso J, Angermeyer MC, Bernert S, Bruffaerts R, Brugha TS, Bryson H, de Girolamo G, de Graaf R, Demyttenaere K, Gasquet I, Haro JM, Katz SJ, Kessler RC, Kovess V, Lepine JP, Ormel J, Polidori G, Russo LJ, Vilagut G, Almansa J, Rbabzadeh-Bouchez S, Autonell J, Bernal M, Buist-Bouwman MA, Codony M, Domingo-Salvany A, Ferrer M, Joo SS, Martinez-Alonso M, Matschinger H, et al: Disability and quality of life impact of mental disorders in Europe: results from the European Study of the Epidemiology of Mental Disorders (ESEMeD) project. Acta Psychiatr Scand. 2004, 420 (Suppl): 38-46.
Mendlowicz MV, Stein MB: Quality of life in individuals with anxiety disorders. Am J Psychiatry. 2000, 157: 669-682. 10.1176/appi.ajp.157.5.669.
de Graaf R, Bijl RV, ten Have M, Beekman AT, Vollebergh WA: Pathways to comorbidity: the transition of pure mood, anxiety and substance use disorders into comorbid conditions in a longitudinal population-based study. J Affect Disord. 2004, 82: 461-467. 10.1016/j.jad.2004.03.001.
Gardenswartz CA, Craske MG: Prevention of panic disorder. Behav Ther. 2001, 32: 725-737. 10.1016/S0005-7894(01)80017-4.
Kenardy J, McCafferty K, Rosa V: Internet-delivered indicated prevention for anxiety disorders: A randomized controlled trial. Behav Cogn Psychother. 2003, 31: 279-289. 10.1017/S1352465803003047.
Livermore N, Sharpe L, McKenzie D: Prevention of panic attacks and panic disorder in COPD. Eur Respir J. 2010, 35: 557-563. 10.1183/09031936.00060309.
Meulenbeek P, Willemse G, Smit F, van Balkom A, Spinhoven P, Cuijpers P: Early intervention in panic: randomized controlled trial and cost-effectiveness analysis. Trials. 2008, 9: 67-10.1186/1745-6215-9-67.
Swinson RP, Soulios C, Cox BJ, Kuch K: Brief treatment of emergency room patients with panic attacks. Am J Psychiatry. 1992, 149: 944-946.
van't Veer-Tazelaar PJ, van Marwijk HW, van Oppen P, van der Horst HE, Smit F, Cuijpers P, Beekman AT: Prevention of late-life anxiety and depression has sustained effects over 24 months: a pragmatic randomized trial. Am J Geriatr Psychiatry. 2011, 19: 230-239. 10.1097/JGP.0b013e3181faee4d.
Batelaan NM, Smit F, de Graaf R, van Balkom AJ, Vollebergh WA, Beekman AT: Identifying target groups for the prevention of anxiety disorders in the general population. Acta Psychiatr Scand. 2010, 122: 56-65.
Smit F, Cuijpers P, Oostenbrink J, Batelaan N, de Graaf R, Beekman A: Costs of nine common mental disorders: implications for curative and preventive psychiatry. J Ment Health Policy Econ. 2006, 9: 193-200.
Donker T, van Straten A, Marks I, Cuijpers P: A brief Web-based screening questionnaire for common mental disorders: development and validation. J Med Internet Res. 2009, 11: e19-10.2196/jmir.1134.
Pearlin LI, Schooler C: The structure of coping. J Health Soc Behav. 1978, 19: 2-21. 10.2307/2136319.
Batelaan NM, de Graaf R, Penninx BW, van Balkom AJ, Vollebergh WA, Beekman AT: The 2-year prognosis of panic episodes in the general population. Psychol Med. 2010, 40: 147-157. 10.1017/S0033291709005625.
World Health Organization: Composite International Diagnostic Interview (CIDI), version 2.1. 1998, Geneva: World Health Organization
Robins LN, Wing J, Wittchen HU, Helzer JE, Babor TF, Burke J, Farmer A, Jablenski A, Pickens R, Regier DA: The Composite International Diagnostic Interview An epidemiologic Instrument suitable for use in conjunction with different diagnostic systems and in different cultures. Arch Gen Psychiatry. 1988, 45: 1069-1077. 10.1001/archpsyc.1988.01800360017003.
Patel V, Weiss HA, Chowdhary N, Naik S, Pednekar S, Chatterjee S, De Silva MJ, Bhat B, Araya R, King M, Simon G, Verdeli H, Kirkwood BR: Effectiveness of an intervention led by lay health counsellors for depressive and anxiety disorders in primary care in Goa, India (MANAS): a cluster randomised controlled trial. Lancet. 2010, 376 (9758): 2086-2095. 10.1016/S0140-6736(10)61508-5.
Cuijpers P, van Straten A, Warmerdam L, van Rooy MJ: Recruiting participants for interventions to prevent the onset of depressive disorders: possible ways to increase participation rates. BMC Health Serv Res. 2010, 10: 181-10.1186/1472-6963-10-181.
Roest AM, Martens EJ, de Jonge P, Denollet J: Anxiety and risk of incident coronary heart disease: a meta-analysis. J Am Coll Cardiol. 2010, 56: 38-46. 10.1016/j.jacc.2010.03.034.
Alonso J, Buron A, Bruffaerts R, He Y, Posada-Villa J, Lepine JP, Angermeyer MC, Levinson D, de Girolamo G, Tachimori H, Mneimneh ZN, Medina-Mora ME, Ormel J, Scott KM, Gureje O, Haro JM, Gluzman S, Lee S, Vilagut G, Kessler RC, Von Korff M: Association of perceived stigma and mood and anxiety disorders: results from the World Mental Health Surveys. Acta Psychiatr Scand. 2008, 118: 305-314. 10.1111/j.1600-0447.2008.01241.x.
European commission Eurostat: Breast cancer screening statistics. Downloaded from: http://epp.eurostat.ec.europa.eu/statistics_explained/index.php/Breast_cancer_screening_statistics. Accessed 04-10-2012
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-244X/12/206/prepub
Acknowledgements
This research was funded by ZONMw, the Netherlands Organization for Health Research and Development, projectnumber 100002111.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
All authors declare that they have no competing interests.
Authors’ contributions
All authors designed the current study. NB, HM, and BT were involved in data collection. NB performed the statistical analyses. All authors contributed to the interpretation of the results. NB drafted the manuscript. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Batelaan, N.M., Smit, J.H., Cuijpers, P. et al. Prevention of anxiety disorders in primary care: A feasibility study. BMC Psychiatry 12, 206 (2012). https://doi.org/10.1186/1471-244X-12-206
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-244X-12-206