
Abstract
Background
The risk of allergic diseases among Kawasaki disease (KD) patients relative to the general population is not known. The aim of this study was to perform a population-based cohort study to investigate the risk of allergic diseases among children after KD in Taiwan- a country with the third highest incidence of KD in the world.
Methods
Data were obtained from the Taiwan National Health Insurance Research Database. In total, 253 patients who were 5 years of age or younger and had a first-time hospitalization with a diagnosis of KD between 1997 and 2005 were included as the study cohort and 1,012 non-KD patients matched for age and sex were included as comparison cohort. Multivariate Cox proportional hazard regression model was used to adjust for confounding and to compare the 6-year allergic-free survival rate between these two cohorts.
Results
The incidence rate of allergic diseases (184.66 per 1000 person-year) was significantly higher in the KD cohort than in the control cohort (124.99 per 1000 person-years). After adjusting for potential confounders, the adjusted hazard ratios of asthma and allergic rhinitis were 1.51 (95% confidence interval = 1.17-1.95) and 1.30 (95% confidence interval = 1.04-1.62), respectively.
Conclusion
We conclude that KD patients were at an increased risk for allergic diseases compared with the comparison cohort.
Similar content being viewed by others


Background
Kawasaki disease (KD) is an acute febrile systemic vasculitis that was first described by Kawasaki et al. in 1974 [1]. In developed countries, it is the leading cause of acquired heart disease in children but its etiology remains unknown [2–4]. This acute illness presents with systemic inflammation and occurs with fever lasting at least 5 days, with conjunctival and oral mucosa changes, fissured lips, cervical lymphadenopathy, skin rash, and palm/sole erythema/induration [5, 6]. The most serious complication of KD is the presence of coronary artery lesions (CAL), including myocardial infarction, coronary artery fistula formation [7], coronary artery dilatation, and coronary artery aneurysm (CAA) [8, 9]. Children aged less than 5 years of age are the most susceptible population. According to recent epidemiologic studies, Asian populations have a much higher incidence of KD. Japan has the highest annual incidence in the world [10], followed by Korea and Taiwan (218, 113 and 69 per 100,000 children aged < 5 years of age, respectively) [11, 12]. The incidence of KD has increased globally in recent years [9, 10, 13–15].
It has been reported that the prevalence of atopic dermatitis among children with KD was 9 times greater than that of controls [16]. A Japanese cross-sectional survey reported that atopic dermatitis and/or allergic rhinitis were more common in KD-affected children when compared to the non-KD controls [17]. A cross-sectional sibling study conducted in Singapore reported that KD-affected children had more allergy and asthma than their non-KD affected siblings [18]. These cross-sectional data suggest that KD tended to be associated with allergic diseases [17, 18]. Recently, a case–control study found that KD patients were more likely to have been admitted to hospital for asthma/allergy than non-KD controls (OR = 2.6, 95% CI = 1.7-4.2) [19]. These data suggest that these allergic diseases are unlikely to reflect immune dysfunction resulting from KD itself [19].
To our knowledge, despite several reports of conditions associated with alergic diseases in KD patients (cross-sectional or case–control designs), large sample data regarding the exact incidence of allergic diseases occurring in KD patients are still lacking. We undertook the present study to determine the incidence of allergic diseases in KD patients in Taiwan.
Methods
Data source
The National Health Insurance (NHI) program, which provides compulsory universal health insurance, was implemented in Taiwan on March 1, 1995. Under the NHI, 98% of the island’s population receives all forms of health care services including outpatient services, inpatient care, Chinese medicine, dental care, childbirth, physical therapy, preventive health care, home care, and rehabilitation for chronic mental illness. In cooperation with the Bureau of NHI, the National Health Research Institute (NHRI) of Taiwan randomly sampled a representative database of 1,000,000 subjects from the entire NHI enrollees by means of a systematic sampling method for research purposes. There were no statistically significant differences in age, gender, and healthcare costs between the sample group and all enrollees, as reported by the NHRI. This dataset (from January 1996 to December 2010) includes all claim data for these 1,000,000 subjects, offers a good opportunity to examine the incidence of allergic diseases occurring among patients with KD. These databases have previously been used for epidemiological research, and information on prescription use, diagnoses, and hospitalizations has been shown to be of high quality [20].
Because the identification numbers of all individuals in the NHRI databases were encrypted to protect the privacy of the individuals, this study was exempt from full review by the Institution Review Board.
Study cohorts
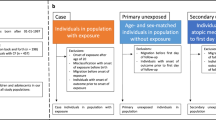
From this database, we selected all children who were 5 years of age or younger and had a first-time hospitalization with a diagnosis of KD (ICD-9-CM code 446.1) between 1997 and 2005 (n = 378). We excluded subjects who had been hospitalized with a KD before the year of 1997 (i.e., in 1996; because the NHI program started in 1995, we were able to trace the use of medical services only to 1996) to limit the study subjects to new cases (n = 31). We excluded subjects who had been given a diagnosis of allergic diseases including asthma (ICD-9 CM code 493.X) or allergic rhinitis (ICD-9 CM code 477.X) prior to their index ambulatory care visit (the date of a patient’s hospitalization for KD) (n = 93). In total, 254 patients with KD were included in the study group.
The comparison cohort was selected from the remaining patients in the database. We first excluded patients who had been diagnosed with KD during the period 1996–2010 and those older 5 years of age. Controls were also chosen from 1997 to 2005. For each study cohort patient, 4 reference individuals were identified randomly and matched for gender, age, and year of index ambulatory care visit. For comparison cohort, the index ambulatory care visit was their first ambulatory care visit occurring in the index year. Of the 254 incident KD cases ascertained, no controls could be found for one case. A total of 1,012 individuals served as a comparison cohort group.
Potential confounders
For all individuals in the two cohorts, we obtained data on potential confounders including age, gender, number of physician visits 1 year before index date, the levels of insurance as an economic index and urbanization level of the community in which the patients resided. In Taiwan, the urbanization levels are divided into 7 categories, ranging from category 1 (the most urbanized) to category 7 (least urbanized), based on 5 indices: population density, percentages of residents with college or higher education, percentages of residents over 65 years old, percentage of residents who were agricultural workers, and the number of physicians per 100,000 people [21]. For the analyses, the urban–rural classification was aggregated into 3 levels: I. urban (categories 1 and 2), II. suburban (categories 3 and 4), and III. rural (categories 5, 6, and 7). All children were financially dependents of the insured (the ones who paid the insurance fee; i.e., usually the child’s parents, grandparents, or social welfare institutions). We used the monthly income of children’s enrollees as a proxy to measure of children’s socioeconomic status.
Statistics
For comparisons of proportions between the study and comparison cohorts, chi-square statistics were used. We compared continuous data using the student t test. Each patient was individually tracked for a 5-year period starting from their cohort entry to identify whether the patient had experienced allergic rhinitis or asthma during the follow-up period. The person-years of follow-up were calculated for each patient from the date of the cohort entry to the date of being diagnosed with allergic diseases or the end of the study (a 5-year follow-up period), whichever occurred first. Incidence rates were calculated by dividing the number of allergic diseases by the total person-years of follow-up. Cox proportional hazards regression models were used to estimate the hazard ratios (HR) and 95% confidence intervals (CI) in a multivariate model adjusting for the above-mentioned potential confounders. The assumption of proportional hazards was assessed by including an interaction term between time and exposure (KD patients vs patients in the comparison cohort) in the model, and the proportional assumption was satisfied. Analyses were performed using the SAS statistical package (version 9.2, SAS Institute Inc., Cary, NC, USA). All statistical tests were two-sided. Values of p < 0.05 were considered statistically significant.
Results
There were 253 patients in our KD cohort that were compared with 1,012 selected matched controls. Table 1 presents the distribution of demographic characteristics of the study subjects and controls. After matching for sex and age, patients with KD had comparable characteristics for monthly income of the insured and urbanicity of residence of the health insurance enrolled. However, patients with KD had more physician visit on average than patients in the comparison cohort (22.42 times vs 15.31 times).
Table 2 shows the distribution of allergic diseases during the 5-year follow-up periods for these two cohorts. Of the total 1,265 sampled patients, 620 patients (49.01%) developed allergic diseases throughout the study periods, 148 (58.50% of the KD patients) from the study cohort (with an incidence rate of 184.66 per 1,000 person-years) and 472 (46.64%) from the comparison cohort (with an incidence rate of 124.99 per 1,000 person-years). The log-rank test showed that KD patients had significantly lower 5-year allergic disease-free survival rates than patients in the comparison cohort (p < 0.001).
Table 2 also shows the crude and adjusted hazard ratios (HR) for allergic diseases for the two groups. After adjusting for potential confounders, the HR for asthma for KD patients was 1.51 (95% CI = 1.17-1.95) compared to patients in the comparison cohort. KD patients were at a 1.30-fold risk for allergic rhinitis compared with patients in comparison cohort (HR = 1.30, 95% CI = 1.04-1.62).
Discussion
To our knowledge, this is the first population-based cohort study to examine the relationship between KD and the subsequent risk of allergic diseases (asthma and allergic rhinitis). Previous studies used either cross-sectional [16–18] or case–control designs [19] to investigate the prevalence of asthma/allergic diseases in KD patients and non-KD controls.
Previous studies reported that the majority of the increased asthma and allergy admissions occurred prior to the KD illness, suggesting that these allergy/asthma are unlikely to reflect immune dysfunction resulting from KD itself. It may also suggest that a distinct immune phenotype may be associated with an increased risk of both KD and asthma/allergy [19]. In the acute stage of KD, there is sustained neutrophil activation [22], with increased release of human neutrophil elastase and matrix metalloproteinases [23], and similar patterns may be important in childhood asthma [24]. Polymorphisms in the mannose-binding lectin (MBL) gene have been reported to be associated with susceptibility to KD [25]. A role for MBL polymorphisms in susceptibility to asthma and allergic disease has also been reported [26]. This suggests that immunogenetic variations in the innate immune response may contribute to the shared risk of KD and asthma/allergy [19].
In this population-based cohort study, we found that KD patients were 1.52 times more likely than the comparison cohort to develope allergic diseases. These data may reflect the immunological consequences of KD, and/or an underlying susceptibility to both KD and asthma/allergy. The investigation of children following the KD illness does not differentiate between the two possibilities.
The mechanisms by which KD may increase the risk of future development of allergic diseases remain unclear. The immune system is highly activated during KD with a myriad of immunoregulatory changes including Th1 immune related response (such as IFN-gamma, TNF-alpha, IL-1, and IL-10) [27–29] and Th2 immune related response (such as eosinophil, IL-4, IL-5 [30, 31]. There is evidence that the scar from prior BCG vaccination and the tuberculin skin test becomes inflated in patients during acute KD and is a marker of Th1-mediated delayed hypersensitivity reaction [32]. Thus, if KD is indeed a strong Th1 trigger and Th1 is associated with a reduced risk of allergic diseases, we would expect that children with KD will have a lower risk of developing allergic diseases. Our data did not provide support for this hygiene hypothesis, where an inverse relationship between increased Th1 cell-mediated inflammation (KD) and decreased Th2-cell mediated allergy is observed [33, 34]. By contrast, we observed a positive association between KD and the risk of allergic diseases. The reasons for the differences in the findings are unknown. KD results in an acute inflammation. It has been shown that infections (inflammations) are able to alter the function of regulatory T cells [35]. Our finding of an increased risk of developing allergic diseases following KD may therefore plausibly be related to the effect of regulatory T cells. Clearly, more work will be needed before the influence of immune activation of Th1/Th2 on the risk of developing allergic diseases is understood.
The major strength of our study is the use of a computerized database, which is population based and is highly representative and allows a clear observation of the temporal relationship between KD and allergic diseases. Because we included a national sample of KD patients between 1997 and 2005, and because the control subjects in this study were selected from a simple random sampling of insured general population, we can rule out the possibility of selection bias.
Several limitations of the present study should be noted. First, KD cases were identified using medical diagnoses recorded in the claim database. Data on the accuracy of KD discharge diagnoses is not available in Taiwan. Potential inaccurate data in claims record could also lead to possible misclassification of KD. Given the comprehensiveness of the NHI database and its previous use for incidence study for KD [12], we are confident that the effect of misclassification of case status on our results is most likely of minor importance. Second, diagnoses of allergic diseases rely on administrative claims data may be less accurate than those obtained according to standardized criteria and misclassification is possible. However, this misclassification is likely to be nondifferential and therefore would tend to underestimate rather than overestimate the true relative risk of alleric diseases among KD patients. Third, any study investigating an increased incidence of one disease (allergic disease) conditional on the diagnosis of another disease (KD) in clinical settings may suffer from detection bias. In this study, the fact that KD patients had more physician visit on average than patients in the comparison cohort could make KD patients more likely to have allergies diagnosed. In addition, physicians might be more inclined to find allergic diseases in patients who had KD due to the fact that previous studies have shown the correlation between KD and allergic disease [16–19]. Therefore, the possibility that our findings have arisen from detection bias could not be excluded. Fourth, although we adjusted for several potential confounders in the statistical analysis, a number of possible confounding variables, including body mass index and family history of allergic diseases, which are associated with allergic diseases were not included in our database. Lastly, as with any observational study, residual confounding by unmeasured factors which are different between case cohort and comparison cohort is also possible.
Conclusion
In conclusion, this study is the first cohort study to investigate epidemiologic data for allergic diseases among children after KD. Our study results provide evidence that KD patients are at an increased risk for the development of allergic diseases compared with the general population.
References
Kawasaki T, Kosaki F, Okawa S: A new infantile acute febrile mucocutaneous lymph node syndrome (MLNS) prevailing in Japan. Pediatrics. 1974, 54: 271-6.
Wang CL, Wu YT, Liu CA: Kawasaki disease: infection, immunity and genetics. Pediatr Infect Dis J. 2005, 24: 998-1004. 10.1097/01.inf.0000183786.70519.fa.
Burns JC, Glode MP: Kawasaki syndrome. Lancet. 2004, 364: 533-44. 10.1016/S0140-6736(04)16814-1.
Kuo HC, Liang CD, Wang CL: Serum albumin level predicts initial intravenous immunoglobulin treatment failure in Kawasaki disease. Acta Paediatr. 2010, 99: 1578-83. 10.1111/j.1651-2227.2010.01875.x.
Liang CD, Kuo HC, Yang KD: Coronary artery fistula associated with Kawasaki disease. Am Heart J. 2009, 157: 584-8. 10.1016/j.ahj.2008.11.020.
Kuo HC, Wang CL, Wang L: Patient characteristics and intravenous immunoglobulin product may affect eosinophils in Kawasaki disease. Pediatr Allergy Immunol. 2008, 19: 184-5. 10.1111/j.1399-3038.2007.00657.x.
Townley RG, Barlan IB, Patino C: The effect of BCG vaccine at birth on the development of atopy or allergic disease in young children. Ann Allergy Asthma Immunol. 2004, 92: 350-5. 10.1016/S1081-1206(10)61574-8.
Newburger JW, Takahashi M, Gerber MA: Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the Committee on Rheumatic Fever, Endocarditis and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Circulation. 2004, 110: 2747-71. 10.1161/01.CIR.0000145143.19711.78.
Kuo HC, Yang KD, Juo SH: ITPKC Single Nucleotide Polymorphism Associated with the Kawasaki Disease in a Taiwanese Population. PLoS One. 2011, 6: e17370-10.1371/journal.pone.0017370.
Nakamura Y, Yashiro M, Uehara R: Epidemiologic features of Kawasaki disease in Japan: results of the 2007–2008 nationwide survey. J Epidemiol. 2010, 20: 302-7. 10.2188/jea.JE20090180.
Park YW, Han JW, Hong YM: Epidemiological features of Kawasaki disease in Korea, 2006–2008. Pediatr Int. 2011, 53: 36-9. 10.1111/j.1442-200X.2010.03178.x.
Huang WC, Huang LM, Chang IS: Epidemiologic features of Kawasaki disease in Taiwan, 2003–2006. Pediatrics. 2009, 123: e401-5. 10.1542/peds.2008-2187.
Du ZD, Zhao D, Du J: Epidemiologic study on Kawasaki disease in Beijing from 2000 through 2004. Pediatr Infect Dis J. 2007, 26: 449-51. 10.1097/01.inf.0000261196.79223.18.
Bar-Meir M, Haklai Z, Dor M: Kawasaki disease in Israel. Pediatr Infect Dis J. 2011, 30: 589-92. 10.1097/INF.0b013e31820e3849.
Singh S, Aulakh R, Bhalla AK: Is Kawasaki disease incidence rising in Chandigarh, North India?. Arch Dis Child. 2011, 96: 137-40. 10.1136/adc.2010.194001.
Brosius CL, Newburger JW, Burns JC: Increased prevalence of atopic dermatitis in Kawasaki disease. Pediatr Infect Dis J. 1988, 7: 863-6.
Matsuoka S, Tatara K, Nakagawa R: Tendency toward atopy in Kawasaki disease. Eur J Pediatr. 1997, 156: 30-2. 10.1007/s004310050546.
Liew WK, Lim CW, Tan TH: The effect of Kawasaki disease on childhood allergies- a sibling control study. Pediatr Allergy Immunol. 2011, 22: 488-93. 10.1111/j.1399-3038.2011.01149.x.
Webster RJ, Carter KW, Warrington NM: Hospitalization with infection, asthma and allergy in Kawasaki disease patients and their families: genealogical analysis using linked population data. PLoS One. 2011, 6: e28004-10.1371/journal.pone.0028004.
Kuo HW, Tsai SS, Tiao MM: Epidemiologic features of CKD in Taiwan. Am J Kidney Dis. 2007, 49: 46-55. 10.1053/j.ajkd.2006.10.007.
Liu CY, Hung YT, Chuang YL: Incorporating developments stratification of Taiwan townships into sampling design of large scale health interview survey. J Health Manag. 2006, 14: 1-22.
Kuo HC, Yang KD, Liang CD: The relationship of eosinophilia to intravenous immunoglobulin treatment failure in Kawasaki disease. Pediatr Allergy Immunol. 2007, 18: 354-9. 10.1111/j.1399-3038.2007.00516.x.
Biezeveld MH, van Mierlo G, Lutter R: Sustained activation of neutrophils in the course of Kawasaki disease: an association with matrix metalloproteinases. Clin Exp Immunol. 2005, 141: 183-8. 10.1111/j.1365-2249.2005.02829.x.
Gualano RC, Vlahos R, Anderson GP: What is the contribution of respiratory viruses and lung proteases to airway remodelling in asthma and chronic obstructive pulmonary disease?. Pulm Pharmacol Ther. 2006, 19: 18-23. 10.1016/j.pupt.2005.02.009.
Sato S, Kawashima H, Kashiwagi Y: Association of mannose-binding lectin gene polymorphisms with Kawasaki disease in the Japanese. Int J Rheum Dis. 2009, 12: 307-10. 10.1111/j.1756-185X.2009.01428.x.
Worthley DL, Bardy PG, Mullighan CG: Mannose-binding lectin: biology and clinical implications. Intern Med J. 2005, 35: 548-55. 10.1111/j.1445-5994.2005.00908.x.
Jason J, Gregg L, Han: Immunoregulatory changes in Kawasaki disease. Clin Immunol Immunopatho. 1997, 84: 296-306. 10.1006/clin.1997.4376.
Hsieh KS, Lai TJ, Hwang YT: IL-10 promoter genetic polymorphisms and risk of Kawasaki disease in Taiwan. Dis Markers. 2011, 30: 51-9.
Kuo HC, Chang WC: Genetic polymorphisms in Kawasaki disease. Acta Pharmacol Sin. 2011, 32: 1193-8. 10.1038/aps.2011.93.
Burns JC, Shimizu C, Shike H: Family-based association analysis implicates IL-4 in susceptibility to Kawasaki disease. Genes Immun. 2005, 6: 438-44. 10.1038/sj.gene.6364225.
Kuo HC, Wang CL, Liang CD: Association of lower eosinophil-related T helper 2 (Th2) cytokines with coronary artery lesions in Kawasaki disease. Pediatr Allergy Immunol. 2009, 20: 266-72. 10.1111/j.1399-3038.2008.00779.x.
Bertotto A, Spinozzi F, Vagliasindi C: Tuberculin skin test reactivity in Kawasaki disease. Pediatr Res. 1997, 1: 560-2.
Strachan DP: Hay fever, hygiene, and household size. Br Med J. 1989, 299: 1259-60. 10.1136/bmj.299.6710.1259.
Maitra A, Sherriff A, Griffiths M: Pertussis vaccination in infancy and asthma or allergy in later childhood: birth cohort study. Br Med J. 2004, 328: 925-6. 10.1136/bmj.38045.858889.EB.
Preston JA, Thorburn AN, Starkey MR: Streptococcus pneumonia infection suppress allergic airways disease by inducing regulatory T-cells. Eur Respir J. 2011, 37: 53-64. 10.1183/09031936.00049510.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2431/13/38/prepub
Acknowledgments
This study is based in part on data from the National Health Insurance Research Database provided by the Bureau of National Health Insurance, Department of Health and managed by National Health Research Institutes. The interpretation and conclusions contained herein do not represent those of Bureau of National Health Insurance, Department of Health or National Health Research Institutes.
This study was supported in part from the National Science Council, Taiwan (NSC 100-2314-B-182-061-MY3); and grant from Chang Gung Memorial Hospital, Taiwan. (CMRPG8A0481).
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
KHC wrote the manuscript. CWC, YKD, YHR and WCL provided essential insight into the interpretation of the results. HSC did the statistical analysis. YCY contributed to study design and interpretation of the data. He had full access to all of the data in the study and took responsibility for the integrity of the data and the accuracy of the data analysis. All authors read and approved the final manuscript.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Kuo, HC., Chang, WC., Yang, K.D. et al. Kawasaki disease and subsequent risk of allergic diseases: a population-based matched cohort study. BMC Pediatr 13, 38 (2013). https://doi.org/10.1186/1471-2431-13-38
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2431-13-38