
Abstract
Background
To explore the intraocular pressure-lowering effect and complications of diode laser transscleral cyclophotocoagulation (DLTSC) followed by phacotrabeculectomy on medically unresponsive acute primary angle closure eyes.
Methods
Nine eyes of nine medically unresponsive acute primary angle closure patients were enrolled. All the patients underwent cyclophotocoagulation followed by phacotrabeculectomy to control the prolonged acute attack. Data were recorded prospectively and then analyzed retrospectively. The reduction in intraocular pressure, improvement of vision and the complications were evaluated.
Results
After DLTSC, the IOP of all the patients were reduced, but all were above 21 mmHg under topical anti-glaucoma medications. After phacotrabeculectomy, the IOP of all the patients was decreased. At the final visit, the vision of all the patients was improved and the IOP of all the patients was below 21 mmHg without anti-glaucoma medications. There were no complications during the DLTSC and phacotrabeculectomy. Uveitis was the common complications after the both procedures, which were resolved by medication treatment.
Conclusion
Diode laser transscleral cyclophotocoagulation followed by phacotrabeculectomy is an alternative procedure to control the intraocular pressure of medically unresponsive acute primary angle closure eyes with few complications.
Similar content being viewed by others


Background
Acute primary angle closure (APAC) is a common ophthalmic emergency that requires early treatment. The longer the duration of increased intraocular pressure (IOP), the more irreversible damage there is to the optic nerve head, iris, lens, endothelium, and drainage pathways [1, 2]. Early aggressive management of an acute episode is crucial to prevent development of primary angle closure glaucoma (PACG) after APAC and to relieve the excruciating symptoms of the patients [3].
The conventional treatment for APAC is to reduce IOP medically, after which laser peripheral iridoplasty or iridotomy (LPI) is performed. However, in some eyes, the acute attack is severe and often refractory to medical treatment [4–7], and the prolonged poor cornea clarity of APAC patients limits the application of LPI. In such cases, trabeculectomy is occasionally performed as an urgent intervention [6]. However, for medically unresponsive APAC cases, trabeculectomy on inflamed ‘hot’ eyes with high IOP poses a high risk of surgical failure and complications, such as suprachoroidal hemorrhage [4, 8–10].
Is there any other method to control the high IOP of medically unresponsive APAC eyes? Diode laser transscleral cyclophotocoagulation (DLTSC), initially reserved for eyes with refractory glaucoma and limited visual prognosis, is now being used more widely, even as primary surgical treatment in glaucoma therapy, including primary open-angle and pseudoexfoliative glaucoma [7, 11], chronic angle closure glaucoma [12, 13], and even eyes with good vision [14]. In this study, we aimed to explore the safety and efficacy of DLTSC followed by phacotrabeculectomy on Chinese medically unresponsive APAC eyes.
Methods
Patients
Consecutive medically unresponsive APAC patients accepted DLTSC followed by phacotrabeculectomy from November 2008 to October 2010 were included in this study. Data were recorded prospectively and then analyzed retrospectively. This study adheres to the Declaration of Helsinki and was approved by the ethics committee of Tianjin Medical University Eye Hospital. Informed consent was obtained from each patient.
All the patients underwent a thorough ocular examination, including visual acuity, slit-lamp biomicroscopy, IOP, B-scan, ultrasound biomicroscopy etc at presentation. Post-operative evaluation was conducted on days 1, 7 and months 1, 3, 6 and 12. The patients, who needed closer follow-up, according to the clinical outcome, were evaluated monthly or even weekly. On each occasion, the patients were fully examined under the slit-lamp biomicroscopy. The visual acuity and IOP were determined. Any complications of surgery were noted. All the IOP was measured by non-contact tonometer (Full Auto Tonometer TX-F, Canon, Japan) for three times and the average was recorded.
Diode laser transscleral cyclophotocoagulation
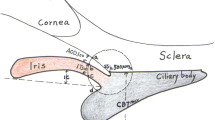
Diode laser transscleral cyclophotocoagulation was performed with the OcuLight SLx 810 nm diode laser photocoagulator and the handheld fiberoptic G-probe, both from Iris Medical Instruments (Mountain View, CA) [13, 15]. All the treatments were performed under local anesthesia (2 ml of 2% lidocaine as a retrobulbar injection). The laser was set at an initial power of 1700 mW and a duration of 1 second. The laser power was titrated upwards and downwards during the procedure. The target was to achieve a ‘burst’ sound in roughly half of the laser applications. Laser applications were spaced evenly over the inferior 180 degrees, while sparing the 3- and 9-o’clock regions.
Post-operatively, all preoperative IOP-lowering medications, except systemic medications (such as high-osmotic agents) and topical pilocarpine, were continued. The patients were also given tobramycin and dexamethasone eye drops (TobraDex, S.A. Alcon-Couvreur N.V., Rijksweg, Puurs, Belgium) 6 times per day, 1% atropine gel (Dishan, Xingqi Co., Ltd, Shenyang, China) twice per day, and pranoprofen eye drops (Pranopulin, Senju Pharmaceutical Co., Ltd, Osaka, Japan) 4 times per day.
Phacotrabeculectomy
All the surgeries were performed by the same experienced surgeon (JJ). During the surgery, after the fornix-based conjunctival flap and rectangular scleral flap were performed, mitomycin-C (MMC) was applied under the conjunctival and scleral flaps. Then, the phacoemulsification and intraocular lens (IOL) implantation was performed, followed by trabeculectomy and peripheral iridectomy. The scleral flap and the conjunctival wound were closed with 10/0 nylon sutures at the end of the surgery.
After surgery, all IOP-lowering medications were discontinued. Postoperative medications employed routinely are tobramycin and dexamethasone eye drops (TobraDex, S.A. Alcon-Couvreur N.V., Rijksweg, Puurs, Belgium) 6 times per day, and pranoprofen eye drops (Pranopulin, Senju Pharmaceutical Co., Ltd, Osaka, Japan) 4 times per day. All the drops were discontinued after 6 weeks of treatment.
Results
Patients’ characteristics
Nine consecutive medically unresponsive APAC patients (9 eyes) were enrolled in this study. All of the patients presented with symptoms of eye pain, blurred vision, headache and nausea. The duration of the acute attack ranged from 6 days to 23 days. The vision of the patients was threatened mostly by significant cornea edema. The IOP of the patients ranged from 43.2 mmHg to 58.7 mmHg, despite maximum medication. None of the patients were performed laser peripheral iridotomy for corneal edema. The detailed patient characteristics are indicated in Table 1.
Clinical outcome after DLTSC
There were no complications during the DLTSC procedure. After DLTSC, the IOP of all the patients was lower, but all were above 21 mmHg (from 23.3 to 32 mmHg) under topical anti-glaucoma medications. After DLTSC, corneal edema of all the patients was relieved in part. All the patients experienced uveitis (aqueous flare: from ++ to +++), 5 patients experienced subconjunctival hemorrhage, and only 1 patient experienced exudation in the anterior chamber, indicating a relatively severe inflammatory reaction.
Clinical outcome after phacotrabeculectomy
After phacotrabeculectomy, the IOP of all the patients was lower. The follow-up period ranged from 14 months to 35 months. At the final visit, the vision of all the patients was improved and the IOP of all the patients was below 21 mmHg (from 12.8 to 18 mmHg) without anti-glaucoma medications or other surgical interventions. The detailed IOP results are indicated in Table 2.
There were no complications during the surgery. At 1 day after surgery, all the patients presented with cornea edema and uveitis and 3 patients presented with exudation in the anterior chamber, which were resolved within a week by medication treatment alone (2 patients) or combined with YAG laser (1 patient). No other complications were encountered during the follow-up after the surgery.
Discussion
To date, many methods have been studied to control the IOP of APAC. The conventional initial treatment may involve one or more of the IOP-lowering drugs. However, for a significant proportion of APAC patients, these treatments may fail to reduce IOP. [1] Laser peripheral iridotomy appears to be effective and safe in controlling rising IOP [16–19]. However, for Asian eyes, the results after LPI are not satisfactory [20, 21]. Moreover, the application of LPI is compromised by the edematous cornea of APAC patients. In cases when LPI is not possible, immediate paracentesis has been proposed as an alternative procedure to rapidly lower the IOP [22]. However, the performance of paracentesis in an eye with APAC has many unique technical difficulties [1], and the paracentesis itself runs the risk of ocular decompression retinopathy [23] and intraocular inflammation. Therefore, in selected cases, surgical intervention may need to be considered as a primary procedure to lower the IOP [6]. However, for medically unresponsive cases of APAC, trabeculectomy on eyes with high IOP has a high risk of surgical failure and complications, especially suprachoroidal hemorrhage [4]. As a severely debilitating complication of glaucoma surgery, suprachoroidal hemorrhage has been reported to be strongly associated with the level of the preoperative IOP in several studies [8–10].
Diode laser transscleral cyclophotocoagulation, traditionally used only in eyes with advanced end stage glaucoma and with little or no visual potential, has now become a popular minimally invasive treatment for glaucoma [7, 11–14]. The 810 nm diode wavelength is twice as efficient for DLTSC than the Nd:YAG wavelength of 1064 nm, and the near infrared light generated by the diode laser is absorbed better by melanin than the longer wavelengths [14, 24]. This advantage allows the diode laser to use less energy to produce comparable lesions.
In this study, for medically unresponsive APAC eyes, firstly, we tried DLTSC to control the high IOP. Although the IOP was decreased after DLTSC, the desired degree of reduction was not achieved. The authors think this is mostly because of the conservative protocol for DLTSC in our study, or APAC is not sensitive to DLTSC, which needs further study to confirm. In order to avoid severe complication, we adopted the narrow laser scope (only the inferior 180 degrees), a short laser duration time (1000 ms) and low laser energy (1700 mW) during the DLTSC. The only article covering the use of DLTSC on APAC eyes in the literature included 5 APAC cases from two ophthalmic units in the United Kingdom [25]. All of their 5 cases achieved successful control of IOP and resolution of the acute attack after DLTSC, which is different from the results in our case series. The mechanism of their better control of IOP was not clear; we think it may be partly due to the iridotomy or iridoplasty performed before DLTSC in most of their cases.
Although the IOP was not controlled under 21 mmHg after DLTSC, the cornea edema was relieved and the IOP was decreased in part, which enabled us to perform phacotrabeculectomy with a lower risk of severe complications. After the surgery, the IOP of all the eyes was controlled to an ideal level and visual acuity was significantly improved. Moreover, except for uveitis and cornea edema, no other severe complications (such as vision loss, phthisis and suprachoroidal hemorrhage, etc.) were encountered after DLTSC and filtration surgery. One reason might be the comparatively low laser energies we applied in comparison with other investigators, who treated with 1.75–3 W for 2 s [26–29]. Another might be the relieved corneal edema and the decreased IOP by DLTSC before phacotrabeculectomy, which simplified the surgical manipulations.
The authors acknowledge the limitations of the study. This was a non-comparative case series and the sample size was relatively small. The laser energy employed and the MMC protocol used were not uniform and the IOP-lowering effect of cataract surgery alone was not evaluated. A prospective comparative study (filtration surgery after DLTSC versus filtration surgery under high IOP) with larger samples would be ideal. Further study to compare the IOP-lowering effect of different DLTSC protocols on APAC eyes is needed. However, in this study, the authors did, indeed, propose an alternative procedure to control the IOP of medically unresponsive APAC eyes without severe complications.
Conclusions
Diode laser transscleral cyclophotocoagulation followed by phacotrabeculectomy is an alternative procedure to control the intraocular pressure of medically unresponsive acute primary angle closure eyes with few complications.
References
Lam DS, Tham CC, Lai JS, Leung DY: Current approaches to the management of acute primary angle closure. Curr Opin Ophthalmol. 2007, 18: 146-151. 10.1097/ICU.0b013e32808374c9.
David R, Tessler Z, Yassur Y: Long-term outcome of primary acute angle-closure glaucoma. Br J Ophthalmol. 1985, 69: 261-262. 10.1136/bjo.69.4.261.
Tan AM, Loon SC, Chew PT: Outcomes following acute primary angle closure in an Asian population. Clin Experiment Ophthalmol. 2009, 37: 467-472. 10.1111/j.1442-9071.2009.02060.x.
Aung T, Tow SL, Yap EY, Chan SP, Seah SK: Trabeculectomy for acute primary angle closure. Ophthalmology. 2000, 107: 1298-1302. 10.1016/S0161-6420(00)00137-8.
Seah SK, Foster PJ, Chew PT, Jap A, Oen F, Fam HB, Lim AS: Incidence of acute primary angle-closure glaucoma in Singapore. An island-wide survey. Arch Ophthalmol. 1997, 115: 1436-1440. 10.1001/archopht.1997.01100160606014.
Buckley SA, Reeves B, Burdon M, Moorman C, Wheatcroft S, Edelsten C, Benjamin L: Acute angle closure glaucoma: relative failure of YAG iridotomy in affected eyes and factors influencing outcome. Br J Ophthalmol. 1994, 78: 529-533. 10.1136/bjo.78.7.529.
Kramp K, Vick HP, Guthoff R: Transscleral diode laser contact cyclophotocoagulation in the treatment of different glaucomas, also as primary surgery. Graefes Arch Clin Exp Ophthalmol. 2002, 240: 698-703. 10.1007/s00417-002-0508-5.
Speaker MG, Guerriero PN, Met JA, Coad CT, Berger A, Marmor M: A case-control study of risk factors for intraoperative suprachoroidal expulsive hemorrhage. Ophthalmology. 1991, 98: 202-209. 10.1016/S0161-6420(91)32316-9. discussion 210
Jiraskova N, Rozsival P, Pozlerova J, Ludvikova M, Burova M: Expulsive hemorrhage after glaucoma filtering surgery. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2009, 153: 221-224. 10.5507/bp.2009.038.
The Fluorouracil Filtering Surgery Study Group: Risk factors for suprachoroidal hemorrhage after filtering surgery. Am J Ophthalmol. 1992, 113: 501-507.
Grueb M, Rohrbach JM, Bartz-Schmidt KU, Schlote T: Transscleral diode laser cyclophotocoagulation as primary and secondary surgical treatment in primary open-angle and pseudoexfoliatve glaucoma. Long-term clinical outcomes. Graefes Arch Clin Exp Ophthalmol. 2006, 244: 1293-1299. 10.1007/s00417-006-0280-z.
Lai JS, Tham CC, Chan JC, Lam DS: Diode laser transscleral cyclophotocoagulation in the treatment of chronic angle-closure glaucoma: a preliminary study. J Glaucoma. 2003, 12: 360-364. 10.1097/00061198-200308000-00011.
Lai JS, Tham CC, Chan JC, Lam DS: Diode laser transscleral cyclophotocoagulation as primary surgical treatment for medically uncontrolled chronic angle closure glaucoma: long-term clinical outcomes. J Glaucoma. 2005, 14: 114-119. 10.1097/01.ijg.0000151890.41239.c5.
Ansari E, Gandhewar J: Long-term efficacy and visual acuity following transscleral diode laser photocoagulation in cases of refractory and non-refractory glaucoma. Eye (Lond). 2007, 21: 936-940. 10.1038/sj.eye.6702345.
Pokroy R, Greenwald Y, Pollack A, Bukelman A, Zalish M: Visual loss after transscleral diode laser cyclophotocoagulation for primary open-angle and neovascular glaucoma. Ophthalmic Surg Lasers Imaging. 2008, 39: 22-29. 10.3928/15428877-20080101-09.
Lai JS, Tham CC, Chua JK, Lam DS: Immediate diode laser peripheral iridoplasty as treatment of acute attack of primary angle closure glaucoma: a preliminary study. J Glaucoma. 2001, 10: 89-94. 10.1097/00061198-200104000-00004.
Lai JS, Tham CC, Chua JK, Poon AS, Chan JC, Lam SW, Lam DS: To compare argon laser peripheral iridoplasty (ALPI) against systemic medications in treatment of acute primary angle-closure: mid-term results. Eye (Lond). 2006, 20: 309-314. 10.1038/sj.eye.6701867.
Lam DS, Lai JS, Tham CC, Chua JK, Poon AS: Argon laser peripheral iridoplasty versus conventional systemic medical therapy in treatment of acute primary angle-closure glaucoma: a prospective, randomized, controlled trial. Ophthalmology. 2002, 109: 1591-1596. 10.1016/S0161-6420(02)01158-2.
Saunders DC: Acute closed-angle glaucoma and Nd-YAG laser iridotomy. Br J Ophthalmol. 1990, 74: 523-525. 10.1136/bjo.74.9.523.
Aung T, Ang LP, Chan SP, Chew PT: Acute primary angle-closure: long-term intraocular pressure outcome in Asian eyes. Am J Ophthalmol. 2001, 131: 7-12. 10.1016/S0002-9394(00)00621-8.
Lai JS, Tham CC, Chua JK, Poon AS, Lam DS: Laser peripheral iridoplasty as initial treatment of acute attack of primary angle-closure: a long-term follow-up study. J Glaucoma. 2002, 11: 484-487. 10.1097/00061198-200212000-00005.
Lam DS, Chua JK, Tham CC, Lai JS: Efficacy and safety of immediate anterior chamber paracentesis in the treatment of acute primary angle-closure glaucoma: a pilot study. Ophthalmology. 2002, 109: 64-70. 10.1016/S0161-6420(01)00857-0.
Rao SK, Greenberg PB, Macintyre RB, Ducharme JF: Ocular decompression retinopathy after anterior chamber paracentesis for uveitic glaucoma. Retina. 2009, 29: 280-281. 10.1097/IAE.0b013e318185ea54.
Lin P, Wollstein G, Glavas IP, Schuman JS: Contact transscleral neodymium:yttrium-aluminum-garnet laser cyclophotocoagulation Long-term outcome. Ophthalmology. 2004, 111: 2137-2143. 10.1016/j.ophtha.2004.05.027.
Manna A, Foster P, Papadopoulos M, Nolan W: Cyclodiode laser in the treatment of acute angle closure. Eye (Lond). 2012, 26: 742-745. 10.1038/eye.2011.361.
Brancato R, Carassa RG, Bettin P, Fiori M, Trabucchi G: Contact transscleral cyclophotocoagulation with diode laser in refractory glaucoma. Eur J Ophthalmol. 1995, 5: 32-39.
Rebolleda G, Munoz FJ, Murube J: Audible pops during cyclodiode procedures. J Glaucoma. 1999, 8: 177-183.
Schlote T, Derse M, Rassmann K, Nicaeus T, Dietz K, Thiel HJ: Efficacy and safety of contact transscleral diode laser cyclophotocoagulation for advanced glaucoma. J Glaucoma. 2001, 10: 294-301. 10.1097/00061198-200108000-00009.
Threlkeld AB, Johnson MH: Contact transscleral diode cyclophotocoagulation for refractory glaucoma. J Glaucoma. 1999, 8: 3-7.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2415/14/26/prepub
Acknowledgements
We thank Dr Jun Qiao who helped to collect the data and Dr Tian Tian who helped to proofread the manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
JJ and XX designed and supervised the study; LW drafted the manuscript; CY and WL collected the data; LY and LA analyzed the data and helped to draft the manuscript. All authors read and approved the final manuscript.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Liu, W., Chen, Y., Lv, Y. et al. Diode laser transscleral cyclophotocoagulation followed by phacotrabeculectomy on medically unresponsive acute primary angle closure eyes: the long-term result. BMC Ophthalmol 14, 26 (2014). https://doi.org/10.1186/1471-2415-14-26
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2415-14-26