
Abstract
Background
Poor health literacy is often a key cause of lack of or delayed uptake of health care services. The aim of this study was to assess the health literacy of common ocular diseases, namely cataract, glaucoma, night blindness, trachoma and diabetic retinopathy in Nepal.
Methods
A cross sectional study of 1741 participants randomly selected from non-triaged attendants in the outpatient queue at Tilganga Institute of Ophthalmology, a semi urban general population of Bhaktapur district of Kathmandu Valley and patients attending rural outreach clinics. Participants responded to trained enumerators using verbally administered, semi structured questionnaires on their awareness and knowledge of cataract, glaucoma, diabetic retinopathy, night blindness, and trachoma.
Results
The awareness of cataract across the entire sample was 49.6%, night blindness was 48.3%, diabetic retinopathy was 29%, glaucoma was 21.3% and trachoma was 6.1%. Patients presenting to rural outreach clinics had poorer awareness of cataract, glaucoma, diabetic retinopathy, night blindness and trachoma compared to those from a semi-urban community and an urban eye hospital (p<0.05), Old age was directly associated with poorer awareness of cataract, glaucoma, night blindness, trachoma and diabetic retinopathy (p<0.05). Female gender was associated with lower awareness of cataract, glaucoma, night blindness and trachoma (p<0.05). Literacy was associated with greater awareness of cataract, glaucoma, diabetic retinopathy, night blindness and trachoma (p<0.05). Higher education was significantly associated with greater awareness of cataract, night blindness and trachoma (p<0.05). Multivariate analysis found that the awareness of common ocular diseases was significantly associated with level of education (p<0.05). Similarly, awareness of cataract, glaucoma, trachoma and night blindness was associated with female gender (p<0.05) whereas awareness of cataract, night blindness, trachoma and diabetic retinopathy was associated with age (p<0.05) but the awareness glaucoma and diabetic retinopathy was associated with camps.
Conclusions
Low awareness of common ocular conditions is associated with factors such as female gender, old age, lower levels of education and rural habitation. A would be successful health promotion programs should specifically target health determinants to promote health literacy and to ensure timely utilization of eye care services.
Similar content being viewed by others


Background
In 1981, the Nepal Blindness Survey provided the first epidemiological information on the prevalence of blindness in Nepal. The prevalence of blindness in Nepal was estimated to be 0.84% and was among the poorer in the world [1]. The Rapid Assessment of Avoidable Blindness Survey in 2012 of Nepal found that the prevalence of blindness was 0.35% [2]. Despite the expansion of eye health services, preventable and correctable ocular conditions such as cataract remain leading causes of blindness in Nepal [3–7].
It has long been recognized that in both developing and developed countries, poor health literacy is a key cause of lack of or delayed uptake of health care services, lack of compliance to treatment and poor follow-up [8–12]. Health literacy is defined as the ability of an individual to access, understand and use information to promote and maintain good health [13]. It has been suggested that poor ocular health literacy is a key contributor to the dichotomy that exists between disease prevalence and service uptake [5, 14–16]. In an Indian study, it was found that awareness and knowledge of common ocular conditions, such as cataract, glaucoma, night blindness, trachoma and diabetic retinopathy was very poor [9]. Having heard of the disease was defined as “awareness” and having some understanding of the basic etiology and symptoms of the disease was defined as “knowledge”. At present, no comprehensive study on the awareness and knowledge of common ocular conditions exists for the Nepalese population.
Health education and promotion is the one of the most powerful tools to increase the health literacy, as a public health goal, in different settings or localities [17–19]. As Nepal is a developing country, eye health system here is more focused on the curative services rather than promotive and preventive services. It is the best time to assess and explore the situation of the awareness and knowledge of common eye diseases among different groups of people to help the eye health authorities to make and implement a good plan which is both cost effective and efficient in different social and geographic settings in Nepal.
The aim of this study was to investigate the awareness and knowledge of common causes of blindness, namely: cataract, glaucoma, diabetic retinopathy, night blindness and trachoma in a semi-urban community of Kathmandu Valley; patients presenting to an urban eye hospital and; patients presenting to rural outreach clinics (camps). Since health literacy itself is a multi- factorial entity, the study also investigated the relationship between lack of awareness and other risk factors of poor ocular health such as gender, location of habitation, level of education, literacy and age.
Methods
The cross sectional study was conducted to determine the awareness and knowledge of cataract, glaucoma, night blindness, trachoma and diabetic retinopathy in 1741 respondents over a three month period (March through May in 2009). The sample size was determined by the assumed status of awareness and knowledge of the diseases. Since the status of awareness and knowledge of these conditions are unknown in Nepal, the status of awareness and knowledge figures were derived from studies in India [9]. Night blindness and trachoma were of the lowest awareness and knowledge thus the assumed lowest status of awareness was 20% in all diseases with allowable error of 20%. Then the minimum sample size was 400 in each group. The study ultimately recruited 1741 participants.
Within each location, respondents were randomly selected including 893 respondents from the general semi-urban population of the Bhaktapur district of Kathmandu Valley, 413 respondents from the outpatient queue of an urban eye hospital (Tilganga Institute of Ophthalmology) and 431 respondents presenting to rural outreach clinics. The three groups were selected because they provided respondents from both rural and urban communities. They also represent the groups to which new health promotion measures could be immediately implemented. As free and accessible services are infrequent in rural communities, it is common for many patients who are free of disease symptoms to present themselves at rural outreach clinics. Thus, the sample of patients from four rural outreach clinics in Kathmandu Valley provides a representative sample of the rural community in general. Respondents aged 18 and above years were selected by two processes: (1) the process of simple random sampling using their registration number if they were at the hospital outpatient clinic and rural outreach clinic, or (2) the use of the latest community member list provided by the local government for the semi urban community from the Bhaktapur district of Kathmandu Valley. Questionnaires on awareness and knowledge of cataract, glaucoma, night blindness, trachoma and diabetic retinopathy were designed in English by the Research Department at Tilganga Institute of Ophthalmology, and translated into Nepali using a pragmatic approach to adapt to the target population. All questionnaires were verbally administered by field enumerators who spoke local language and had an understanding of the eye diseases of interest. They were trained and supervised on site by investigators from the research department of Tilganga Institute of Ophthalmology. The same enumerators and investigators were involved at all sites. The pretesting of questionnaires was conducted by enumerators on a similar semi-urban community from a different district of Kathmandu Valley, as well patients from both urban and rural backgrounds at the institute. Respondents demonstrated awareness if they had heard of the eye disease in question. All questions about knowledge were semi- structured. Respondents were asked to “tell” what threat the eye disease posed. The questionnaire contained a list of the possible responses, and the field enumerators marked against the response that most closely corresponded to the respondent’s answer.
Collected data was reviewed immediately on site by the enumerators, then centrally at the Tilganga Institute of Ophthalmology. The data was collated and entered into Microsoft Excel 2007 at the Research Department of Tilganga Institute of Ophthalmology. The data were analyzed using Statistical Package for Social Science (SPSS Inc., Chicago, IL, USA) version 11.5. The bivariate (Spearman’s Rho test, chi square test and odds ratio) and multivariate analysis was used to determine the relationship between age, gender, rural habitation, literacy and level of education with awareness. P values less than 0.05 were considered statistically significant.
The Institutional Review Committee of Tilganga Institute of Ophthalmology reviewed and gave approval to conduct research in the line with the Helsinki Declaration of Medical Ethics.
Results
Demographic information
One thousand seven hundred and forty one participants were included in this study. Eight hundred and ninety three (51.29%) were from the semi-urban communities in Bhaktapur district in Kathmandu Valley, 431 (24.76%) were from the outpatient queue at the Tilganga Institute of Ophthalmology, an urban eye hospital, and 417 (23.95%) were selected from rural outreach clinics. Their age ranged from 16 to 89 years and the mean age was 41.5 (SD 17.7) years. The male to female ratio was 1.2 (54.6% male and 45.4% female). Thirty three point four percent of respondents were illiterate, defined as no formal schooling (Table 1).
Awareness of common ocular conditions
Overall awareness was 49.6% (863) for cataract, 21.3% (370) for glaucoma, 48.3% (841) for night blindness, 6.1% (106) for trachoma and 29% (504) for diabetic retinopathy (Table 2 Part A).
Age
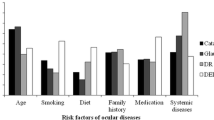
Old age was significantly associated with poorer awareness of cataract (Spearman’s Rho correlation coefficient (r) =0.94, p = 0.005), glaucoma (r = 1.00, p<0.001), night blindness (r = 1.00, p<0.001), trachoma (r = 0.89, p = 0.019) and diabetic retinopathy (r = 1.00, p<0.001) (Table 2, part C).
Gender
Females had significantly lower awareness of cataract (odds ratio = 1.77 (95% confidence interval (CI) = 1.46-2.14, p < 0.001), glaucoma (odds ratio = 1.38 (95% CI = 1.09-1.75), p = 0.007), night blindness (odds ratio = 1.67 (95% CI = 1.38-2.02), p<0.001), trachoma (odds ratio = 1.67 (95% CI = 1.10-2.52), p = 0.014). The difference in awareness for diabetic retinopathy between males and females was not significant (odds ratio = 1.19 (95% CI = 0.96-1.46), p = 0.11) (Table 2, Part D).
Location of participants
Patients presenting at rural outreach clinics had significantly poorer awareness of cataract (odds ratio = 2.32 (95% CI = 1.84-2.91), p < 0.001), glaucoma (odds ratio = 3.57 (95% CI = 2.48-5.14), p< 0.001), night blindness (odds ratio = 3.14 (95% CI = 2.47-3.99), p< 0.001), trachoma (odds ratio = 6.80 (95% CI = 2.75-16.82), p< 0.001) and diabetic retinopathy (odds ratio = 2.63 (95% CI = 1.97-3.50), p<0.001) compared to patients presenting to urban outpatient clinic at Tilganga Institute of Ophthalmology and the general semi-urban population of Kathmandu valley (Table 2, part B).
Awareness and level of education
Illiterate participants (33.43%) had significantly poorer awareness of all ocular conditions investigated including cataract (odds ratio = 3.83 (95 CI = 3.09-4.75), p< 0.001), glaucoma (odds ratio = 2.84 (95% CI = 2.13-3.79), p<0.001), night blindness (odds ratio = 4.78 (95% CI = 3.82-5.96), p < 0.001), trachoma (odds ratio = 4.64 (95% CI = 2.46-8.72), p<0.001) and diabetic retinopathy (odds ratio = 3.14 (95% CI = 2.43-4.06), p< 0.001).
The level of education of participants and their awareness of the conditions was also investigated. The levels of education were divided into three categories: illiterate, those who have basic literacy but less than primary school education, those whose highest level of education was primary, lower secondary or higher secondary or tertiary.
Higher level of education was significantly associated with greater awareness of cataract (r = 0.90, p = 0.037), night blindness (r = 0.90, p = 0.037) and trachoma (r = 0.98, p = 0.005). However, the relationship between higher education and awareness of diabetic retinopathy (r = 0.70, p = 0.188) and glaucoma (r = 0.70, p = 0.188) were not significant (Table 2, Part E).
Multiple correlations showed that the awareness on female gender is significantly associated with cataract (r = −0.128, p = 0.000), glaucoma (r = −0.065, p = 0.008), trachoma (r = −0.060, p = 0.012) and night blindness (r = −0.115, p = 0.000) except diabetic retinopathy (r = −0.023, p = 0.198). The awareness is significantly associated with cataract (r = −0.142, p = 0.000), trachoma (r = −0.053, p = 0.025), night blindness (r = −0.23, p = 0.000) and diabetic retinopathy (r = −0.109, p = 0.000) expect glaucoma (r = −0.042, p = 0.060) by ageing of population. The awareness is significantly associated with cataract (r = 0.352, p = 0.000), glaucoma (r = 0.216, p = 0.000), trachoma (r = 0.155, p = 0.000), night blindness (r = 0.420, p = 0.000) and diabetic retinopathy (r = 0.265, p = 0.000) by higher education level. Whereas the awareness of common ocular diseases is significantly associated with glaucoma (r = −0.151, p = 0.000) and diabetic retinopathy (r = −0.142, p = 0.000) with rural outreach clinics (camps) but there is no association with cataract (r = −0.028, p = 0.147), trachoma (r = −0.014, p = 0.304) and night blindness (r = 0.008, p = 0.379) (Table 3).
Source of information
The survey also investigated the common sources of information for awareness and knowledge of common ocular conditions. The Television and print media such as magazines, posters and newspapers, were the source of information in 52% of cases. Twenty four point nine percent of respondents derived their awareness and knowledge of common ocular conditions from family, relatives and friends who suffer from the condition, while 9.4% respondents derived their information from family, relatives and friends who do not suffer from the conditions (9.4%). Health care workers were the source of awareness in 3.3% and outreach eye clinics were the source of information in 3.1% of cases (Table 4).
Discussion
This study identified a number of factors associated with lower awareness of common ocular conditions in Nepal, where blindness due to treatable conditions remains high despite increasing efforts to improve eye health. The factors examined were age, gender, literacy, level of education and location of habitation.
Cataract is the principal cause of blindness in Nepal, followed by glaucoma and diabetic retinopathy and trachoma [20–22]. The awareness of ocular conditions correlated with the prevalence of these conditions with the exception of night blindness. The high level of awareness and low prevalence of night blindness is directly related to the Nepal National Vitamin A Program which is a six month yearly campaign that delivers high dose vitamin A to 6 to 60 months old children in 42 of the 75 districts in Nepal [23].
In Nepal, 69% of blind people are females [1]. However, there is not a majority of females to males in the Nepalese population. Also, this disparity is not accounted for by longer female life expectancy (0.88 males to 1 female in those over the age of 65 years) [24]. Females account for 63.8% of cataract blindness because they do not receive treatment at the same rate as men [1]. It is estimated that cataract blindness would be reduced by 12.5% in developing countries if women received cataract surgery at the same rate as men [25]. Given the significant difference in level of awareness of common ocular conditions between males and females, it is likely that low level of awareness plays an important role. Potential causes for this include the fact that only 24% of females in Nepal are literate as opposed to 52% of males. Females are also more likely to live in a rural location and have lower income [24, 26, 27]. All these factors reduce access to health education, and ultimately, affect health seeking behaviour. Any programs aimed at improving health literacy must specifically address gender specific barriers. Programs aimed at improving other determinants such as poor literacy should also be gender-sensitive.
The highest rate of blindness in Nepal is for those who are over 70 years of age where prevalence is over 10.6% [28]. Even in developed countries, the risk of blindness is ten times higher in those over 65 than for younger individuals [29, 30]. There are many causes for the under-utilization of services in the elderly. For example, the elderly are more likely to associate decline in vision with natural aging, less likely to present for surveillance and monitoring, more conservative in the uptake of procedures, less compliant with medications and follow-up [31–33]. This may be related to the fact that literacy rates decline with age in both males and females, and urban and rural communities. For example, literacy amongst 10–14 year olds is 86% for males and 83% for females compared to the literacy rate of 34% for older males and 3% for older females [34]. The Elderly are also more likely to live in rural areas [35]. Hence, there is a need for culturally secure educational programs targeted at the elderly.
Eighty percent of the Nepalese population and ninety percent of country’s blind population live in rural areas. Numerous studies from developed and developing countries have demonstrated under-utilization of services in rural areas [36–40]. With the increase in free rural outreach services, it is proposed that a lack of education about common eye diseases and their management is a major contributor to the current roadblock in service utilization. Despite the fact that rural outreach clinics rely on self-presentation, this study showed that awareness of common ocular diseases is significantly lower in this group when compared to the general population in semi urban communities, as well as those who present to urban tertiary eye care centre. This may be attributed to the fact that tools such as print and electronic media, which are the source of information in 52% of cases, are less readily available. Also, the significant disparity in literacy rate between urban (literacy rate of 64%) and rural (literacy rate of 34%) communities may preclude the use of such sources [34]. Further, many patients present despite little awareness of eye diseases because outreach clinics are one of the few free health services available to rural communities and the frequency of service provision is low. However, without adequate awareness and knowledge, the initiative to present to outreach clinics may not translate to acceptance of treatments, such as cataract surgery, or timely presentation to services when they are not free and easily accessible [41]. In fact, one study showed that even when offered free transport and free surgery, the utilization of cataract surgery in parts of rural Nepal was as low as 60% [16]. Therefore, education about the early warning signs of common ocular conditions, the benefits of timely management, and its possible outcomes would be an important addition to current rural outreach services.
Illiteracy is generally associated with lack of disease awareness [13, 42, 43]. Forty three percent of the Nepalese population is illiterate. Fourteen percent of males and 18% of females have not attended primary school. Fifty four percent of males and 59% females have not attended high school. Female, old age, rural habitation and lower socio-economic class are all risk factors for illiteracy [34]. This is the same groups who carries the highest burden of disease and have the least capacity to access care. Higher level of education beyond simple literacy is associated with better awareness and knowledge of common ocular conditions when compared to those with basic literacy. This may be confounded by other factors such as higher socio-economic background and urban habitation. In summary, it is vital that future health promotion campaigns need to expand beyond traditional means of printed media to make them accessible to illiterate populations who carry high disease burdens.
Multivariate analysis revealed that the awareness of common ocular diseases namely cataract glaucoma, trachoma, night blindness and diabetic retinopathy was significantly associated with level of education (p = <0.05). Similarly, association was found in female gender, age and location of the participants where some diseases had association with common ocular diseases and some were not. Except diabetic retinopathy (p = 0.198), the awareness of common ocular diseases had significant association with female gender (p = <0.05). The awareness of cataract, trachoma, night blindness and diabetic retinopathy had significant association with age (p <0.05). Glaucoma and diabetic retinopathy were significant association with location (p <0.05) but other three ocular conditions like cataract, trachoma and night blindness were not associated with rural outreach camps.
There are some limitations to this study. Firstly, two of the three cohorts (approximate 48.71% of respondents) are already presenting for care either to an urban eye hospital clinic or to a rural outreach clinic, thus, many already demonstrate some awareness of ocular conditions. However, presentation does not necessarily equate to knowledge and awareness, which are essential for identification of early warning signs of disease, compliance to treatment and follow-up. Further, it is common for the majority of the population from a community to present for check-up by the outreach clinics even in the absence of disease or symptom because the service is free and accessible. Therefore, this group offers a relatively representative sample of a rural community. Evidently, there exists much scope for more comprehensive studies on awareness and knowledge of ocular diseases in those from rural communities who have not presented to care, but the recruitment of respondents may be difficult. It is also important to note that while this study examined the relationship between individual determinants of health literacy, it has been alluded to in the discussion that many of these factors co-exist. Therefore, future work is needed to determine the complex interplay between these factors and their collective impact on health literacy and outcome.
Conclusions
Whilst some progress has been made in the reduction of blindness in Nepal, further improvements necessitate an increase in health literacy of the community. This study shows that even at the sentinel stages of awareness and knowledge, factors such as female gender, old age, illiteracy, lower level of education and rural habitation act as major impediments. Additionally, these factors impacting on health literacy tend to occur simultaneously in the same individuals and producing compounding effects. Strategic actions targeted at these factors are essential in the development of programs that can holistically address all the barriers to the improvement of ocular health.
References
Brilliant LB, Pokhrel RP, Grasset NC, Lepkowski JM, Kolstad A, Hawks W, Pararajasegaram R, Brilliant GE, Gilbert S, Shrestha SR, et al: Epidemiology of blindness in Nepal. Bull World Health Organ. 1985, 63 (2): 375-386.
Nepal Netra Jyoti Sangh: The epidemiology of blindness in Nepal. 2012, Kathmandu Nepal: Netra Jyoti Sangh
Rahmani B, Tielsch JM, Katz J, Gottsch J, Quigley H, Javitt J, Sommer A: The cause-specific prevalence of visual impairment in an urban population. The Baltimore Eye Survey. Ophthalmol. 1996, 103 (11): 1721-1726. 10.1016/S0161-6420(96)30435-1.
Rizyal A, Karmacharya PC, Koirala S: Profile of blindness in Nepal: a hospital based study. Nepal Med College J. 2005, 7 (1): 54-57.
Thapa SS, Berg RV, Khanal S, Paudyal I, Pandey P, Maharjan N, Twayna SN, Paudyal G, Gurung R, Ruit S, et al: Prevalence of visual impairment, cataract surgery and awareness of cataract and glaucoma in Bhaktapur district of Nepal: The Bhaktapur Glaucoma Study. BMC Ophthalmol. 2011, 11 (1): 2-10.1186/1471-2415-11-2.
Khatry SK, West KP, Katz J, LeClerq SC, Pradhan EK, Wu LS, Thapa MD, Pokhrel RP: Epidemiology of xerophthalmia in Nepal. A pattern of household poverty, childhood illness, and mortality. The Sarlahi Study Group. Arch Ophthalmol. 1995, 113 (4): 425-429. 10.1001/archopht.1995.01100040039024.
Sapkota YD, Sunuwar M, Naito T, Akura J, Adhikari HK: The prevalence of blindness and cataract surgery in rautahat district, Nepal. Ophthalmic Epidemiol. 2010, 17 (2): 82-89. 10.3109/09286581003624947.
Attebo K, Mitchell P, Cumming R, Smith W: Knowledge and beliefs about common eye diseases. Aust N Z J Ophthalmol. 1997, 25 (4): 283-287.
Dandona R, Dandona L, John RK, McCarty CA, Rao GN: Awareness of eye diseases in an urban population in southern India. Bull World Health Organ. 2001, 79 (2): 96-102.
Livingston PM, Lee SE, De Paola C, Carson CA, Guest CS, Taylor HR: Knowledge of glaucoma, and its relationship to self-care practices, in a population sample. Aust N Z J Ophthalmol. 1995, 23 (1): 37-41. 10.1111/j.1442-9071.1995.tb01643.x.
Livingston PM, McCarty CA, Taylor HR: Knowledge, attitudes, and self care practices associated with age related eye disease in Australia. Brit J Ophthalmol. 1998, 82 (7): 780-785. 10.1136/bjo.82.7.780.
Javitt JC: Preventing blindness in Americans: The need for eye health education. Surv Ophthalmol. 1995, 40 (1): 41-44. 10.1016/S0039-6257(95)80045-X.
7th Global Conference on Health Promotion: track themes 2: Health literacy and health behaviour. http://www.who.int/healthpromotion/conferences/7gchp/track2/en/index.html,
Sapkota YD, Pokharel GP, Dulal S, Byanju RN, Maharjan IM: Barriers to up take cataract surgery in Gandaki Zone, Nepal. Kathmandu Univ Med J (KUMJ). 2004, 2 (2): 103-112.
Sapkota YD, Pokharel GP, Nirmalan PK, Dulal S, Maharjan IM, Prakash K: Prevalence of blindness and cataract surgery in Gandaki Zone, Nepal. Brit J Ophthalmol. 2006, 90 (4): 411-416. 10.1136/bjo.2005.082503.
Snellingen T, Shrestha BR, Gharti MP, Shrestha JK, Upadhyay MP, Pokhrel RP: Socioeconomic barriers to cataract surgery in Nepal: the south Asian cataract management study. Brit J Ophthalmol. 1998, 82 (12): 1424-1428. 10.1136/bjo.82.12.1424.
Nutbeam D: Health literacy as a public health goal: a challenge for comptemporary health education and strategies into the 21st century. Health Prom Int. 2000, 15 (3): 259-267. 10.1093/heapro/15.3.259. 15
Shores NJ, Maida I, Soriano V, Nunez M: Sexual transmission is associated with spontaneous HCV clearance in HIV-infected patients. J Hepatol. 2008, 49 (3): 323-328. 10.1016/j.jhep.2008.04.010.
Noertjojo K, Maberley D, Bassett K, Courtright P: Awareness of eye diseases and risk factors: identifying needs for health education and promotion in Canada. Canad J Ophthalmol. 2006, 41 (5): 617-623. 10.1016/S0008-4182(06)80035-9.
Editorial: Cataract - a leading cause of blindness. J Nepal Med Assoc. 2007, 46 (167): I-II.
Thapa SS, Berg RVD, Khanal S, Paudyal I, Pandey P, Maharjan N, Twyana SN, Paudyal G, Gurung R, Ruit S, et al: Prevalence of visual impairment, cataract surgery and awareness of cataract and glaucoma in Bhaktapur district of Nepal: The Bhaktapur Glaucoma Study. BMC Ophthalmol. 2011, 11: 1-10.1186/1471-2415-11-1.
Nepal facts and figures. http://www.hollows.org/nepal/Facts/,
Gorstein J, Shreshtra RK, Pandey S, Adhikari RK, Pradhan A: Current status of vitamin a deficiency and the National vitamin a control program in Nepal: results of the 1998 National micronutrient status survey. Asia Pacif J Clin Nutrit. 2003, 12 (1): 96-103.
Abou-Gareeb I, Lewallen S, Bassett K, Courtright P: Gender and blindness: a meta-analysis of population-based prevalence surveys. Ophthal Epidemiol. 2001, 8 (1): 39-56. 10.1076/opep.8.1.39.1540.
Lewallen S, Courtright P: Gender and use of cataract surgical services in developing countries. Bull World Health Organ. 2002, 80 (4): 300-303.
Balarajan Y, Selvaraj S, Subramanian SV: Health care and equity in India. Lancet. 2011, 377 (9764): 505-515. 10.1016/S0140-6736(10)61894-6.
Bornemisza O, Ranson MK, Poletti TM, Sondorp E: Promoting health equity in conflict-affected fragile states. Soc Sci Med. 2010, 70 (1): 80-88. 10.1016/j.socscimed.2009.09.032.
Asian Journal of Ophthalmology: Blindness in Asia - The Facts. 2002, Singapore, 11-13. vol.4
Pizzarello LD: The dimensions of the problem of eye disease among the elderly. Ophthalmology. 1987, 94 (9): 1191-1195. 10.1016/S0161-6420(87)33308-1.
Singh MM, Murthy GVS, Venkatraman R, Rao SP, Nayar S: A study of ocular morbidity among elderly population in a rural area of central India. Ind J Ophthalmol. 1997, 45 (1): 61-65.
Brundtland GH: Endorsement of the global initiative vision 2020: the right to sight. J Comm Eye Health. 1999, 12: 16-
Wormald R: Delivery of eye care to the elderly: practical considerations. Comm Eye Health. 1999, 12: 6-7.
Pradhan S, Mughal N, Mahomed I: Self-reported eye disease in elderly South Asian subjects from an inner city cluster in Bradford: a small-scale study to investigate knowledge and awareness of ocular disease. Eye. 2000, 14 (4): 620-624. 10.1038/eye.2000.153.
LIteracy and education literacy rates. http://cbs.gov.np/wp-content/uploads/2012/02/Statistical_Report_Vol1.pdf,
Demographic characteristics. http://cbs.gov.np/wp-content/uploads/2012/02/Statistical_Report_Vol1.pdf,
Chandrashekhar TS, Bhat HV, Pai RP, Nair SK: Coverage, utilization and barriers to cataract surgical services in rural South India: results from a population-based study. Public health. 2007, 121 (2): 130-136. 10.1016/j.puhe.2006.07.027.
Ng JQ, Morlet N, Semmens JB: Socioeconomic and rural differences for cataract surgery in Western Australia. Clin Exper Ophthalmol. 2006, 34 (4): 317-323. 10.1111/j.1442-9071.2006.01214.x.
Zhou JB, Guan HJ, Qu J, Yang XJ, Peng D, Gu HY: A study on the awareness of cataract disease and treatment options in patients who need surgery in a rural area of Eastern China. Eur J Ophthalmol. 2008, 18 (4): 544-550.
Du Toit R, Ramke J, Naduvilath T, Brian G: Awareness and use of eye care services in Fiji. Ophthal Epidemiol. 2006, 13 (5): 309-320. 10.1080/09286580600826629.
Krishnaiah S, Kovai V, Srinivas M, Shamanna BR, Rao GN, Thomas R: Awareness of glaucoma in the rural population of Southern India. Ind J Ophthalmol. 2005, 53 (3): 205-208. 10.4103/0301-4738.16685.
Brilliant GE, Lepkowski JM, Zurita B, Thulasiraj RD: Social determinants of cataract surgery utilization in South India. Archives of Ophthalmology. 1991, 109 (4): 584-589. 10.1001/archopht.1991.01080040152048.
Kickbusch IS: Health literacy: addressing the health and education divide. Health Promotion International. 2001, 16 (3): 289-297. 10.1093/heapro/16.3.289.
Brilliant GE, Brilliant LB: Using social epidemiology to understand who stays blind and who gets operated for cataract in a rural setting. Soc Sci Med. 1985, 21 (5): 553-558. 10.1016/0277-9536(85)90040-1.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2415/14/2/prepub
Acknowledgements and funding
We would like to acknowledge the Fred Hollows Foundation (FHF) for the financial support. We also like to thank Dr. Andreas Muller, Research Coordinator of FHF, Mr. Todd Ritter, Program Coordinator of FHF, Dr. Anil Subedi, Partnership Manger of FHF, all participants and staffs of Tilganga Institute of Ophthalmology for their contributions to the success of this research work.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
MKS contributed to the design of the study, its implementation and preparation of the manuscript. CWG contributed to the analysis of data, preparation and revision of the manuscript. NM contributed to the collection and analysis of data. RG and SR contributed to the design of the study and preparation of the manuscript. All authors read and approved the final manuscript.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an open access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Shrestha, M.K., Guo, C.W., Maharjan, N. et al. Health literacy of common ocular diseases in Nepal. BMC Ophthalmol 14, 2 (2014). https://doi.org/10.1186/1471-2415-14-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2415-14-2