
Abstract
Background
The present study evaluates the outcome of 19 children with rhabdomyosarcoma of the head-and-neck region treated with Intensity Modulated Radiotherapy (IMRT) or Fractionated Stereotactic Radiotherapy (FSRT) between August 1995 and November 2005.
Methods
We treated 19 children with head-and-neck rhabdomyosarcoma with FSRT (n = 14) or IMRT (n = 5) as a part of multimodal therapy. Median age at the time of radiation therapy was 5 years (range 2–15 years). All children received systemic chemotherapy according to the German Soft Tissue Sarcoma Study protocols.
Median size of treatment volume for RT was 93,4 ml. We applied a median total dose of 45 Gy (range 32 Gy – 54 Gy) using a median fractionation of 5 × 1,8 Gy/week (range 1,6 Gy – 1,8 Gy).
The median time interval between primary diagnosis and radiation therapy was 5 months (range 3–9 months).
Results
After RT, the 3- and 5-year survival rate was 94%. The 3- and 5-year actuarial local control rate after RT was 89%.
The actuarial freedom of distant metastases rate at 3- and 5-years was 89% for all patients.
Radiotherapy was well tolerated in all children and could be completed without interruptions > 4 days. No toxicities >CTC grade 2 were observed. The median follow-up time after RT was 17 months.
Conclusion
IMRT and FSRT lead to excellent outcome in children with head-and-neck RMS with a low incidence of treatment-related side effects.
Similar content being viewed by others


Background
Rhabdomyosarcoma (RMS) is the most common soft tissue sarcoma entity in children [1]. The most common sites of RMS in children are the head and neck region (35%), the genitourinary tract (35%) and the extremities (17%) [2]. The orbit is the primary site in about 10% of these tumors, the most common localization in the head and neck area is parameningeal, including the nasopharynx, the paranasal sinuses, the middle ear and mastoid and the infratemporal fossa/pterygopalatine space [2–8]. Most children are younger than 10 years of age (72%) [9].
Modern therapy protocols comprise of surgical resection, chemotherapy and radiotherapy (RT). However, RT in children is commonly applied cautiously with respect to early and late side effects [10–14].
With modern RT techniques such as Intensity Modulated Radiotherapy (IMRT) and Fractionated Stereotactic Radiotherapy (FSRT), the treatment of complex shaped target volumes in close vicinity to sensitive risk structures is possible [15–17]. The present study evaluates the efficacy and toxicity FSRT and IMRT in children with head and neck RMS.
Methods
From August 1995 to November 2005, we treated 19 children with RMS of the head-and-neck region with FSRT (n = 14) and IMRT (n = 5) at our institution.
The data presented in this analysis were acquired retrospectively and anonymously; therefore, no official approval by the local ethics committee was necessary.
Patients' characteristics
The distribution of the tumor sites is shown in table 1. The median age of the children was 5 years at the time of RT (range 2–15 years). The male to female ratio was 1,4 : 1.
Before radiation therapy, all patients had undergone at least one surgical procedure. At primary diagnosis, 3 patients had a subtotal tumor resection, and in 16 patients only a biopsy was performed.
Patients were classified according to the surgical-pathologic grouping system used in the Intergroup Rhabdomyosarcoma Study Group (IRSG) trials [18, 19]. The patients' characteristics can be found in table 1.
All patients included into this study received systemic chemotherapy according to the German Soft Tissue Sarcoma Study protocols CWS 91, CWS 96 and CWS 2002 [20, 21]. The aggressive interdisciplinary treatment concepts are performed in close collaboration between the radiation oncologist and the pediatric oncologist. All patients were registered at the CWS study center.
The median time interval between primary diagnosis and radiation therapy was 5 months (range 3–9 months).
Treatment planning for FSRT and IMRT
Patients were immobilized using an individual mask fixation system made of Scotch-Cast™; for treatment planning contrast-enhanced MRI- and CT-scans were acquired with the mask attached to a non-invasive stereotactic localization frame with an overall geometrical uncertainty of 1–2 mm [22].
For FSRT, we used the three-dimensional treatment planning system Voxelplan [23]. Three to five isocentric non-coplanar irregularly shaped fields formed by a midsize multileaf collimator were applied.
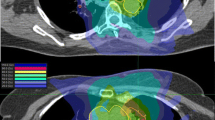
For IMRT, the inverse treatment-planning program Konrad (MRC Systems GmbH, Heidelberg, Germany) was used [24, 25]. An integrated multi-leaf collimator allowed for IMRT using the "step-and-shoot" technique described previously [26]. Fig. 1 shows an IMRT treatment plan for a child with head and neck RMS.

Typical 3D treatment plan of Intensity modulated Radiotherapy (IMRT) for a child with head-and-neck RMS. Thick red line = target volume; orange area 90–100% of the total dose; yellow area 70–90% of the total dose; green area 50–70% of the total dose; blue areas 10–50% of the total dose.
Median size of the planning target volume (PTV) for radiation was 93,4 ml (range 20,8 – 354,8 ml), consisting of the area of contrast uptake in T1-weighted sequences and the enhancing lesion and edema visible in T2-weighted MRI scans prior to chemotherapy including a 20 mm safety margin. It was our policy to define the PTV according to the common guidelines outlined in the treatment protocols of the GPOH. Gross tumor volume (GTV) and clinical target volume (CTV) were not defined separately for planning purposes.
We applied a median total dose of 45 Gy (range 32 Gy – 54 Gy) using a median fractionation of 5 × 1,8 Gy/week (range 1,6 Gy – 1,8 Gy).
In 4 patients, the total dose was applied in a hyperfractionated regimen using single fraction doses of 1,6 Gy.
Deep sedation or general anaesthesia was required in 5 out of 19 children.
Follow-up
Patients were seen for follow-up 6 weeks after radiation, thereafter in 3 to 12 months intervals, including contrast-enhanced MRI-scans, anamnesis and clinical examination. The clinical oncological follow-up was performed by the attending pediatric oncologist. Median follow-up time was 17 months (range 3 months 12 years).
Statistics
Overall survival was calculated from primary diagnosis, survival after RT was calculated from initiation of RT. Progression-free survival after RT was calculated from the first day of RT until tumor progression (local or distant) or death (by any cause), whichever happened first, using the Kaplan Meier method [27]. All statistical analyses were performed using the Statistica 6.1 Software (StatSoft, Tulsa, OK, USA).
Results
Survival
Overall survival rate after primary diagnosis of the RMS was 94% at 3 and 5 years, respectively (Fig. 2). One patient died of tumor progression.

Overall survival in 19 children with head-and-neck RMS treated with FSRT or IMRT.
Local control
The 3- and 5 year actuarial local control rate after RT was 89% (Fig. 3A). We observed 2 local recurrences.

Local Control rates were 89% after 3- and 5-years (A). For RMS of the orbit only, local control was 100% after 5 years, and 81% for parameningeal RMS and other RMS of the head and neck (B). The rate of distant metastases-free survival was 89% at 5 years (C). Distant-metastases free survival rates were 100% for orbital RMS, and 81% for parameningeal and other head-and-neck RMS (D).
With respect to tumor localization, the 3- and 5-year local control rates were 100% for patients with RMS of the orbit and 91% for patients with parameningeal tumors. One patient with parameningeal RMS developed local progression within the prior RT field of the tumor after 4 months. The patient had received a total RT dose of 54 Gy, RT was initiated 5 months after primary diagnosis after inclusion into the CWS-91 protocol. The tumor had shown no response to the CWS chemotherapy (ifosfamide, vincristine, actinomycin-D), and the chemotherapy regimen was switched to carboplatin/etoposide, which showed also no response. Thereafter, RT was initated.
One patient with RMS (ISG Group 4) of the mylohyoid muscle developed local failure 2 months after completion of RT simultaneously with distant bone metastases and progression of the lung metastases present at primary diagnosis. This patient was 1 year old at primary diagnosis, was included into the CWS 2002 protocol and showed no response to chemotherapy prior to RT, which was initiated 4 months after diagnosis; a total RT dose of 54 Gy was applied. At primary diagnosis, lung metastases were already present.
The rate of local control in children with parameningeal and head- and-neck tumors was 81% at 3- and 5-years as compared to 100% in RMS involving the orbit only (Fig. 3B).
Distant metastases-free survival
The actuarial freedom of distant metastases rate at 3- and 5-years was 89% for all patients at 3 and 5 years (Fig. 3C). For patients with RMS of the orbit only, the actuarial distant progression-free rate was 100% at 5 year. One patient with parameningeal RMS developed distant metastases in both lungs 6 months after completion of RT and 1 month after local tumor progression. The actuarial 3- and 5-year distant disease-free survival rate was 91%, respectively in children with parameningeal RMS. As noted above, one girl diagnosed with ISRG 4 RMS of the mylohyoid muscle developed local and distant progression simultaneously 2 months after completion of RT. The rate of distant-metastases-free survival in children with parameningeal and head-and -neck RMS was 81% at 5-years as compared to 100% in children with involvement of the orbit only (Fig. 3D).
Toxicity
Radiotherapy was well tolerated in all children and could be completed without interruptions > 4 days.
Acute radiation induced toxicity
Minor acute radiation-induced side effects occurring within 3 months from RT included skin erythema in 8 patients (42%), alopecia in 4 patients (21%), conjunctivitis in 3 patients (16%), mucositis in 8 patients (42%) and nausea/vomiting in 2 patients (11%); no toxicities >CTC grade 2 developed.
Long-term radiation induced toxicity
To date, the long-term toxicity, developing per definition <6 months after RT, developed in 9 out of 19 patients (47%). We observed three patients with reduced lacrimation and one patient with chronic swelling of the left eye lid with slight erythema CTC grade 1. One patient developed trismus. However, the poor cooperation of the patient in training mouth opening after RT could have contributed to this outcome. In one patient growth hormone deficiency developed with subsequent microsomia requiring growth hormone replacement. This patient had been treated with the initial CWS-96 protocol followed by treatment according to the CWS-protocol for tumor recurrence. Radiotherapy had been applied during the initial protocol with 32 Gy, followed by 8 Gy brachytherapy and 50,4 Gy FSRT for tumor recurrence. In one patient with orbital RMS visual deficiency present prior to RT declined leading to amaurosis. Optic pathway structures received a dose of 34 Gy in 1,8 Gy fractions. Discrete erythema and swelling of the eye lid was observed in the same patient with reduced lacrimation. One patient presented with reduced mouth-opening, and facial asymmetry developed in one patient only (5%). One patient with RMS of the pterygoid fossa developed asymmetric growth of the face with growth reduction on the left side. Until now, no secondary malignancies developed.
Discussion
Treatment guidelines of RMS include surgical resection, systemic chemotherapy using combinations of actinomycin-D, vincristine and cyclophosphamide as well as RT. Commonly, children with RMS are treated within interdisciplinary study protocols: the IRSG (North America), SIOP (Europe), CWS (Germany) and ICS protocols (Italy) [28]. Radiation therapy is an essential part in all treatment protocols for all but completely resected low risk tumors [29, 30]; as a result of these multimodality approaches, the prognosis for children with RMS has improved, with long-term survival rates of 70–80%.
While improvement of outcome with respect to local and distant failures, radiation-induced side effects remained a major problem [31].
IMRT and FSRT enable the delivery of high doses to a defined target volume while sparing surrounding organs at risk; especially for complex shaped tumors of the head-and-neck, RT doses required can be applied while adhering to the tolerance doses of critical normal tissue structures. FSRT has been used safely and effectively for other childhood tumors [32, 33]. IMRT helps spare normal tissues from high-dose areas, but delivers low doses to larger volumes of normal tissue discussed critically with respect to the risk of secondary malignancies. We reserved IMRT for cases in which FSRT did not yield acceptable dose distributions taking into account commonly accepted physical parameters like 90% target coverage and maximum/minimum doses to the adjacent organs at risk.
FSRT and IMRT were chosen in order to reduce dose to normal tissue structures as a general philosophy, but target volumes were not altered with different treatment techniques. Great effort was made to choose beam angles in order to reduce irradiation of bony structures not included into the target volumes in growing children. In patients where bony structures had to be included, e.g. cervical spine, symmetrical irradiation was ensured in order to avoid asymmetric bone growth whenever possible without compromises in target coverage and without exceeding the tolerance dose of normal tissue structures.
During follow-up, only one patient with RMS of the pterygoid fossa developed asymmetric growth of the face with growth reduction on the left side. It must be noted that observation time after RT is relatively short to fully determine long-term side effects such as cosmetic deformity. Therefore, longer follow-up time is needed to make final statements.
With the steep dose-fall off generated by modern high-precision RT, some concern has been raised as to whether the risk of tumor recurrences at the field border might be increased. The results obtained in the present analysis compare favourably to the results published by the large pediatric hematology study groups and reports on single-institution studies [1, 34–38]. Using FSRT and IMRT, the rate of field-border recurrences seems not to be increased outside the PTV as long as the PTV itself is not reduced.
A study published by Wolden et al. reported on 28 patients with head-and-neck RMS [39]. Patients with alveolar histologic features showed significantly worse outcomes as compared to embryonal or undifferentiated tumors. However, in our study, histology as well as other established prognostic factors showed no statistically significant influence on the outcome, most probably due to the small patient number and the small number of events. Furthermore, these factors have already been addressed by the CWS trials which follow a risk-adapted combination of CHT and RT.
Proton RT is another treatment modality enabling the application of high doses while sparing surrounding normal tissue. Preliminary results of proton RT in children with orbital RMS were published by Yock et al. [40]. At the MGH in Boston, 7 children with orbital RMS were treated with proton irradiation in combination with standard chemotherapy. Treatment plan intercomparisons of proton plans and conventional 3-D plans showed that with proton RT excellent tumor coverage can be obtained while reducing the radiation dose to the adjacent normal tissues.
Conclusion
FSRT and IMRT offer excellent results for the treatment of pediatric patients with RMS of the head-and-neck region. The incidence of acute and long-term side-effects is very low. Since only few centers can offer the treatment of pediatric patients with protons to date, FSRT and IMRT can be considered the best photon therapy modalities for a number of pediatric patients with head-and-neck RMS [40].
References
Pappo AS, Shapiro DN, Crist WM, Maurer HM: Biology and therapy of pediatric rhabdomyosarcoma. J Clin Oncol. 1995, 13: 2123-2139.
Wiener ES: Head and neck rhabdomyosarcoma. Semin Pediatr Surg. 1994, 3: 203-206.
Karcioglu ZA, Hadjistilianou D, Rozans M, DeFrancesco S: Orbital rhabdomyosarcoma. Cancer Control. 2004, 11: 328-333.
Sessions DG, Ragab AH, Vietti TJ, Biller HF, Ogura JH: Embryonal rhabdomyosarcoma of the head and neck in children. Laryngoscope. 1973, 83: 890-897. 10.1288/00005537-197306000-00006.
Liebner EJ: Embryonal rhabdomyosarcoma of head and neck in children. Correlation of stage, radiation dose, local control, and survival. Cancer. 1976, 37: 2777-2786. 10.1002/1097-0142(197606)37:6<2777::AID-CNCR2820370632>3.0.CO;2-S.
Mehta S, Verma A, Mann SB, Mehra YN, Sharma SC, Radotra BD: Rhabdomyosarcoma of head and neck--an analysis of 24 cases. Indian J Cancer. 1996, 33: 37-42.
Pratt CB, Smith JW, Woerner S, Mauer AM, Hustu HO, Johnson WW, Shanks EC: Factors leading to delay in the diagnosis and affecting survival of children with head and neck rhabdomyosarcoma. Pediatrics. 1978, 61: 30-34.
Gilles R, Couanet D, Sigal R, De Baere T, Tardivon A, Masselot J, Vanel D: Head and neck rhabdomyosarcomas in children: value of clinical and CT findings in the detection of loco-regional relapses. Clin Radiol. 1994, 49: 412-415. 10.1016/S0009-9260(05)81828-8.
Wharam MD: Rhabdomyosarcoma of Parameningeal Sites. Semin Radiat Oncol. 1997, 7: 212-216. 10.1016/S1053-4296(97)80005-7.
Oeffinger KC, Hudson MM: Long-term complications following childhood and adolescent cancer: foundations for providing risk-based health care for survivors. CA Cancer J Clin. 2004, 54: 208-236.
Mulhern RK, Merchant TE, Gajjar A, Reddick WE, Kun LE: Late neurocognitive sequelae in survivors of brain tumours in childhood. Lancet Oncol. 2004, 5: 399-408. 10.1016/S1470-2045(04)01507-4.
Paulino AC: Late effects of radiotherapy for pediatric extremity sarcomas. Int J Radiat Oncol Biol Phys. 2004, 60: 265-274. 10.1016/j.ijrobp.2004.02.001.
Simon T, Hero B, Bongartz R, Schmidt M, Muller RP, Berthold F: Intensified external-beam radiation therapy improves the outcome of stage 4 neuroblastoma in children > 1 year with residual local disease. Strahlenther Onkol. 2006, 182: 389-394. 10.1007/s00066-006-1498-8.
Eich HT, Muller RP, Micke O, Kocher M, Berthold F, Hero B: Esthesioneuroblastoma in childhood and adolescence. Better prognosis with multimodal treatment?. Strahlenther Onkol. 2005, 181: 378-384. 10.1007/s00066-005-1362-2.
Schafer M, Munter M, Sterzing F, Haring P, Rhein B, Debus J: Measurements of characteristics of time pattern in dose delivery in step-and-shoot IMRT. Strahlenther Onkol. 2005, 181: 587-594. 10.1007/s00066-005-1289-7.
Sterzing F, Munter MW, Schafer M, Haering P, Rhein B, Thilmann C, Debus J: Radiobiological investigation of dose-rate effects in intensity-modulated radiation therapy. Strahlenther Onkol. 2005, 181: 42-48. 10.1007/s00066-005-1290-1.
Combs SE, Thilmann C, Debus J, Schulz-Ertner D: Precision radiotherapy for hemangiopericytomas of the central nervous system. Cancer. 2005, 104: 2457-2465. 10.1002/cncr.21448.
Lawrence W, Anderson JR, Gehan EA, Maurer H: Pretreatment TNM staging of childhood rhabdomyosarcoma: a report of the Intergroup Rhabdomyosarcoma Study Group. Children's Cancer Study Group. Pediatric Oncology Group. Cancer. 1997, 80: 1165-1170. 10.1002/(SICI)1097-0142(19970915)80:6<1165::AID-CNCR21>3.0.CO;2-5.
Lawrence W, Gehan EA, Hays DM, Beltangady M, Maurer HM: Prognostic significance of staging factors of the UICC staging system in childhood rhabdomyosarcoma: a report from the Intergroup Rhabdomyosarcoma Study (IRS-II). J Clin Oncol. 1987, 5: 46-54.
Schuck A, Mattke AC, Schmidt B, Kunz DS, Harms D, Knietig R, Treuner J, Koscielniak E: Group II rhabdomyosarcoma and rhabdomyosarcomalike tumors: is radiotherapy necessary?. J Clin Oncol. 2004, 22: 143-149. 10.1200/JCO.2004.04.180.
Koscielniak E, Harms D, Henze G, Jurgens H, Gadner H, Herbst M, Klingebiel T, Schmidt BF, Morgan M, Knietig R, Treuner J: Results of treatment for soft tissue sarcoma in childhood and adolescence: a final report of the German Cooperative Soft Tissue Sarcoma Study CWS-86. J Clin Oncol. 1999, 17: 3706-3719.
Menke M, Hirschfeld F, Mack T, Pastyr O, Sturm V, Schlegel W: Photogrammetric accuracy measurements of head holder systems used for fractionated radiotherapy. Int J Radiat Oncol Biol Phys. 1994, 29: 1147-1155.
Schlegel W, Pastyr O, Bortfeld T, Becker G, Schad L, Gademann G, Lorenz WJ: Computer systems and mechanical tools for stereotactically guided conformation therapy with linear accelerators. Int J Radiat Oncol Biol Phys. 1992, 24: 781-787.
Preiser K, Bortfeld T, Hartwig K, Schlegel W, Stein J: [Inverse radiotherapy planning for intensity modulated photon fields]. Radiologe. 1998, 38: 228-234. 10.1007/s001170050347.
Bortfeld T: Optimized planning using physical objectives and constraints. Semin Radiat Oncol. 1999, 9: 20-34. 10.1016/S1053-4296(99)80052-6.
Munter MW, Thilmann C, Hof H, Didinger B, Rhein B, Nill S, Schlegel W, Wannenmacher M, Debus J: Stereotactic intensity modulated radiation therapy and inverse treatment planning for tumors of the head and neck region: clinical implementation of the step and shoot approach and first clinical results. Radiother Oncol. 2003, 66: 313-321. 10.1016/S0167-8140(03)00021-5.
Clark TG, Bradburn MJ, Love SB, Altman DG: Survival analysis part I: basic concepts and first analyses. Br J Cancer. 2003, 89: 232-238. 10.1038/sj.bjc.6601118.
Benk V, Rodary C, Donaldson SS, Flamant F, Maurer H, Treuner I, Carli M, Gehan E: Parameningeal rhabdomyosarcoma: results of an international workshop. Int J Radiat Oncol Biol Phys. 1996, 36: 533-540. 10.1016/S0360-3016(96)00362-8.
Crist WM, Anderson JR, Meza JL, Fryer C, Raney RB, Ruymann FB, Breneman J, Qualman SJ, Wiener E, Wharam M, Lobe T, Webber B, Maurer HM, Donaldson SS: Intergroup rhabdomyosarcoma study-IV: results for patients with nonmetastatic disease. J Clin Oncol. 2001, 19: 3091-3102.
Crist W, Gehan EA, Ragab AH, Dickman PS, Donaldson SS, Fryer C, Hammond D, Hays DM, Herrmann J, Heyn R, .: The Third Intergroup Rhabdomyosarcoma Study. J Clin Oncol. 1995, 13: 610-630.
Paulino AC, Simon JH, Zhen W, Wen BC: Long-term effects in children treated with radiotherapy for head and neck rhabdomyosarcoma. Int J Radiat Oncol Biol Phys. 2000, 48: 1489-1495. 10.1016/S0360-3016(00)00799-9.
Combs SE, Thilmann C, Huber PE, Hoess A, Debus J, Schulz-Ertner D: Achievement of long-term local control in patients with craniopharyngiomas using high precision stereotactic radiotherapy. Cancer. 2007, 109: 2308-2314. 10.1002/cncr.22703.
Schulz-Ertner D, Debus J, Lohr F, Frank C, Hoss A, Wannenmacher M: Fractionated stereotactic conformal radiation therapy of brain stem gliomas: outcome and prognostic factors. Radiother Oncol. 2000, 57: 215-223. 10.1016/S0167-8140(00)00230-9.
Donaldson SS, Meza J, Breneman JC, Crist WM, Laurie F, Qualman SJ, Wharam M: Results from the IRS-IV randomized trial of hyperfractionated radiotherapy in children with rhabdomyosarcoma--a report from the IRSG. Int J Radiat Oncol Biol Phys. 2001, 51: 718-728. 10.1016/S0360-3016(01)01709-6.
Paulino AC, Bauman N, Simon JH, Nguyen TX, Ritchie JM, Tannous R: Local control of parameningeal rhabdomyosarcoma: outcomes in non-complete responders to chemoradiation. Med Pediatr Oncol. 2003, 41: 118-122. 10.1002/mpo.10312.
Buwalda J, Schouwenburg PF, Blank LE, Merks JH, Copper MP, Strackee SD, Voute PA, Caron HN: A novel local treatment strategy for advanced stage head and neck rhabdomyosarcomas in children: results of the AMORE protocol. Eur J Cancer. 2003, 39: 1594-1602. 10.1016/S0959-8049(03)00363-0.
Smith SC, Lindsley SK, Felgenhauer J, Hawkins DS, Douglas JG: Intensive induction chemotherapy and delayed irradiation in the management of parameningeal rhabdomyosarcoma. J Pediatr Hematol Oncol. 2003, 25: 774-779. 10.1097/00043426-200310000-00006.
Raney RB, Anderson JR, Barr FG, Donaldson SS, Pappo AS, Qualman SJ, Wiener ES, Maurer HM, Crist WM: Rhabdomyosarcoma and undifferentiated sarcoma in the first two decades of life: a selective review of intergroup rhabdomyosarcoma study group experience and rationale for Intergroup Rhabdomyosarcoma Study V. J Pediatr Hematol Oncol. 2001, 23: 215-220. 10.1097/00043426-200105000-00008.
Wolden SL, Wexler LH, Kraus DH, Laquaglia MP, Lis E, Meyers PA: Intensity-modulated radiotherapy for head-and-neck rhabdomyosarcoma. Int J Radiat Oncol Biol Phys. 2005, 61: 1432-1438. 10.1016/j.ijrobp.2004.08.005.
Yock T, Schneider R, Friedmann A, Adams J, Fullerton B, Tarbell N: Proton radiotherapy for orbital rhabdomyosarcoma: clinical outcome and a dosimetric comparison with photons. Int J Radiat Oncol Biol Phys. 2005, 63: 1161-1168. 10.1016/j.ijrobp.2005.03.052.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2407/7/177/prepub
Acknowledgements
This paper is dedicated to the Dietmar Hopp Foundation with gratitude for the support.
All funding for the study and for the manuscript preparation was taken over by the Department of Radiation Oncology, University Hospital of Heidelberg, Heidelberg, Germany.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The author(s) declare that they have no competing interests.
Authors' contributions
SEC, WB, AEK, PEH, JD and DSE treated the patients and/or performed radiotherapy treatment planning. SEC and DSE collected the clinical data useful for the analysis; SEC and DSE performed the analysis and wrote the manuscript. WB, AEK, PEH and JD revised the article critically for important intellectual content. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
{kind=link}
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Combs, S.E., Behnisch, W., Kulozik, A.E. et al. Intensity Modulated Radiotherapy (IMRT) and Fractionated Stereotactic Radiotherapy (FSRT) for children with head-and-neck-rhabdomyosarcoma. BMC Cancer 7, 177 (2007). https://doi.org/10.1186/1471-2407-7-177
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2407-7-177