
Abstract
Background
It is estimated that 20% of all cancer cases are caused by obesity. Vitamin D is thought to be one of the mechanisms underlying this association. This review aims to summarise the evidence for the mediating effect of vitamin D on the link between obesity and cancer.
Methods
Three literature searches using PubMed and Embase were conducted to assess whether vitamin D plays an important role in the pathway between obesity and cancer: (1) obesity and cancer; (2) obesity and vitamin D; and (3) vitamin D and cancer. A systematic review was performed for (1) and (3), whereas a meta-analysis including random effects analyses was performed for (2).
Results
(1) 32 meta-analyses on obesity and cancer were identified; the majority reported a positive association between obesity and risk of cancer. (2) Our meta-analysis included 12 original studies showing a pooled relative risk of 1.52 (95% CI: 1.33-1.73) for risk of vitamin D deficiency (<50 nmol/L) in obese people (body mass index >30 kg/m2). (3) 21 meta-analyses on circulating vitamin D levels and cancer risk were identified with different results for different types of cancer.
Conclusion
There is consistent evidence for a link between obesity and cancer as well as obesity and low vitamin D. However, it seems like the significance of the mediating role of vitamin D in the biological pathways linking obesity and cancer is low. There is a need for a study including all three components while dealing with bias related to dietary supplements and vitamin D receptor polymorphisms.
Similar content being viewed by others

Background
Over recent decades, the increasing prevalence of obesity has been implicated in the risk of cancer incidence and mortality [1–3]. The link between obesity and cancer mortality is well-established [4, 5]. A prospective cohort study including >900,000 adults in the U.S, estimated that being overweight or obese could account for 14% of deaths from cancer in men and 20% in women [6]. In the UK, an estimated 17,294 excess cancer cases occurring in 2010, were due to overweight and obesity (5.5% of all cancers) [7]. However, the mechanisms that link excess body weight and carcinogenesis are not fully elucidated. Vitamin D is one of the factors suggested to play a role in this pathway [8], but the nature of this association is not fully understood [2]. The immune system and vitamin D receptor (VDR) are only two of the suggested mechanisms for a link between vitamin D and cancer which may also be connected to obesity [9–12].
To evaluate whether vitamin D explains how obesity affects cancer risk, one needs to assess if vitamin D is a mediator variable for the association between obesity (exposure) and cancer (outcome) [13, 14]. In a traditional epidemiological approach, mediation analyses would estimate the excess risk of obesity on cancer explained by vitamin D, by calculating the risk ratio for the association between obesity and cancer in a crude model, and a model adjusted for vitamin D [13]. To our knowledge, no mediation analyses have been published to date for this question, with the exception of one study focusing on breast cancer-specific mortality and one study estimating the attributable fraction of vitamin D in obese people [1, 15]. These studies were not set out as mediation analyses, but suggested that low vitamin D levels contribute to about 16 to 20% of the increased cancer incidence or mortality from breast cancer in overweight and obese patients [1, 15]. This is in contrast with findings from large cohort studies suggesting no association between vitamin D and breast cancer [16].We approached the issue of mediation by vitamin D with a literature review for each association with the question of whether vitamin D plays an important role in the pathway between obesity and cancer (Figure 1): (1) obesity and cancer; (2) obesity and vitamin D; and (3) vitamin D and cancer, while addressing some of the methodological issues. Many meta-analyses have been done for (1) and (3), but limited pooled results are available for (2). Hence, we performed a meta-analysis for the association between obesity and vitamin D.

Overview of vitamin D as a potential mediator for the association between obesity and cancer. Abbreviations: TS, Thurkaa Shanmugalingam; DC, Danielle Crawley; BMI, body mass index.
Methods
Obesity and cancer
A comprehensive literature review of all published meta-analyses on the association between obesity and cancer was carried out. We used computerised search databases (PubMed search followed by an Embase search) to identify full text and abstracts focused on human subjects and published in English language within the last fifteen years. Searches were conducted both with and without MeSH terms for “obesity”, “cancer” and “meta-analysis”. This search was repeated for individual cancer types: “breast”, “colorectal”, “melanoma”, “oesophageal”, “liver”, “lung”, “ovarian”, “endometrial”, “prostate”, “pancreatic” and “kidney” cancer. Although lung cancer may not be the obvious cancer to investigate in the context of obesity [17, 18], some studies [19, 20] reported a positive association while others are inconclusive or conflicting. Hence, lung cancer was also included in this literature review.
Obesity and vitamin D: a meta-analysis
Literature search strategy
We used computerised search databases (PubMed search followed by an Embase search) to identify full text and abstracts published within the last fifteen years, of English language and used human subjects. The searches were performed with and without MeSH terms for “vitamin D”, “25 hydroxyvitamin D”, “obesity”, and “body mass index”. We also included “grey literature” such as abstracts, letters, and articles presented at relevant conferences and meetings. All references of the selected articles were checked using hand searches.
Inclusion criteria
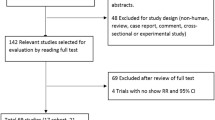
All included studies were of epidemiological nature: cohort, case–control, or cross-sectional. Furthermore, all studies included measurements of vitamin D and body mass index (BMI) and assessed the association between the two. We only included those studies with a sufficient power, deemed as including more than twenty cancer cases. Obesity, defined as BMI >30 kg/m2, was the main exposure of interest. Low vitamin D levels were the outcome, defined using a cut off of <50 nmol/L, which encompasses both vitamin D insufficiency and deficiency.Initially, titles and abstracts of articles were reviewed by two researchers (Thurkaa Shanmugalingam - TS and Danielle Crawley - DC). If they met initial inclusion criteria both abstract and full text article were reviewed to ascertain whether all inclusion criteria were met. A detailed evaluation of methods and results was undertaken. In the case of any disagreement between the two researchers on article inclusion assessments, the full text article was reviewed by a third researcher (Mieke Van Hemelrijck - MVH). Figure 2 illustrates the study exclusion process.

Flowchart of study selection for the association of obesity and vitamin D.
Data extraction
The following details were recorded for each study: author, year of publication, country, type of study, method of vitamin D measurement, statistical tests used, number of subjects with sufficient, insufficient and deficient vitamin D status and BMI of all subjects.
Statistical methods
The association between obesity and vitamin D levels was evaluated by calculating the pooled relative risk (RR) with random effects model to allow for possible heterogeneity between studies. Potential publication bias was evaluated using Beggs Test and Eggers funnel plot. All analyses were performed with STATA version 11.0.
Vitamin D and cancer
A comprehensive literature search of all meta-analyses conducted on the association between vitamin D and cancer was performed. We used computerised search databases (PubMed search followed by an Embase search) to identify full text and abstracts focused on human subjects and published in English language within the last fifteen years. Searches were conducted both with and without MeSH terms for “vitamin D”, “cancer”, “vitamin D receptor”, “polymorphism” and “meta-analysis”. This search was repeated for specific cancer types: “breast”, “colorectal”, “melanoma”, “oesophageal”, “liver”, “lung”, “ovarian”, “endometrial”, “prostate”, “pancreatic” and “kidney” cancer. Moreover, we also searched clinicaltrials.gov for clinical trials focused on “vitamin D supplements” and “cancer” or “neoplasm” [21].
Results
Obesity and cancer
Thirty-two meta-analyses were identified from our literature search on obesity and cancer (Table 1). More specifically, all seven meta-analyses on colorectal cancer showed a positive association between BMI and colorectal cancer risk [22–28]. When looking at site-specific cancer within colorectal cancer, BMI was only significantly associated with rectal cancer in males. Also upper gastro-intestinal cancers (oesophageal, oesophageal gastric junction, gastric and gall bladder cancer) were positively associated with obesity [29–32]. The strongest link was seen for oesophageal cancer with over a two-fold increased risk reported [29, 32]. All four meta-analyses on liver cancer reported an increased risk with increasing BMI [33–36], whereas the lung cancer meta-analysis reported an inverse association with obesity (RR: 0.79; 95% CI: 0.73-0.85) [20]. Meta-analyses on pancreatic cancer reported a positive association with obesity [37–40], which is parallel to the conclusions that can be drawn for kidney cancer[41, 42]. For prostate cancer[43], a protective effect of obesity was reported for localised disease, whereas obesity was positively associated with metastatic disease [44]. The meta-analysis on bladder cancer reported a positive association even when adjustment for smoking was performed [45]. Some variation was observed for breast cancer depending on menopausal status and breast cancer subtype [46, 47]. A positive association between obesity and breast cancer was more distinct among postmenopausal women [48]. The meta-analysis on ovarian cancer reported a positive association with obesity, with no difference in the histological subtypes of ovarian cancer studied [49]. As for the majority of other cancers [50], there was also a positive association found for endometrial cancer[51]. However, this meta-analysis included some studies which used waist circumference as a measure of obesity instead of BMI [51]. The meta-analysis on melanoma reported a positive association in men (RR: 1.31; 95% CI: 1.19-1.44), but not in women (RR: 0.99; 95% CI 0.83-1.18) [52].
Obesity and vitamin D
The initial PubMed search produced a total of 356 (TS) and 352 (DC) papers. Further assessment of abstracts and papers based on the above-defined inclusion criteria (Figure 2) resulted in inclusion of 12 studies for primary data analysis (three cohorts, two case–control and seven cross-sectional studies) (Table 2).
The random effects analyses showed a pooled relative risk of 1.52 (95% CI: 1.33-1.73) for the association between obesity and low vitamin D status (Figure 3). The I2 statistic suggested heterogeneity (I2 = 89.4%). There was no difference between those studies looking at children and adolescents combined and those looking at an adult population (RR: 1.52; 95% CI: 1.04-2.26 and 1.53; 95% CI: 1.31-1.80, respectively).

Forest plot for the association between obesity and low vitamin D levels.
Beggs and Eggers test was used to evaluate publication bias with the funnel plot suggesting the study by Goldner et al. to be an outlier [53] (Results not shown). We performed a sensitivity analysis by excluding this study from our analysis. The pooled estimate of RR did not change drastically, although the link was strengthened to some extent (RR: 1.34; 95% CI: 1.15-1.57).
Vitamin D and cancer
From the literature search, we identified 21 meta-analyses on the association between circulating vitamin D levels and cancer risk (Table 3), showing different results for different types of cancer. We found 34 clinical trials investigating the effect of vitamin D supplementation on cancer (Table 4) [21]. From these, two studies were terminated, 18 are active, 13 have been completed, and one has an unknown status.
All six meta-analyses on colorectal cancer reported that circulating vitamin D levels were inversely associated with cancer risk [54–59]. A pooled analysis from multiple cohort studies on pancreatic cancer, suggested no significant association for participants with low vitamin D levels. Those with vitamin D levels ≥100 mmol/L were at a statistically significant twofold increase in pancreatic cancer compared to those with normal vitamin D levels [60]. The pooled analysis for kidney cancer only found a statistically significant decreased cancer risk among women when vitamin D levels was ≥75 nmol/L [61]. In contrast, all three meta-analyses on prostate cancer found no evidence for an inverse association with vitamin D levels [58, 62, 63]. Results from four out of five meta-analyses showed an inverse association for breast cancer, with the highest quartile of vitamin D levels decreasing the risk of breast cancer [58, 64–67] compared to the lowest quartile. However, it is interesting to note that case–control studies generally report an inverse association, whereas nested case control studies reported null-findings [58, 64–67]. The meta-analysis on ovarian cancer reported a non-statistically significant inverse association with high serum vitamin D levels [68]. Finally, the meta-analysis on total cancer incidence and mortality reports a moderate inverse relationship with circulating vitamin D concentrations [69].
From the 13 completed clinical trials evaluating the effect of vitamin D supplementation on cancer risk, only two have reported results [70, 71]. One randomised trial focused on risk of colorectal cancer over a period of seven years in a double-blinded, placebo-controlled setting, where one group of postmenopausal women received calcium and vitamin D3 supplementation and the other group received placebo [70]. The study found no statistically significant effects of calcium or vitamin D3 supplementation on the incidence of colorectal cancer. The other completed trial had a similar design, but focused on risk of all cancers in postmenopausal woman receiving 1400–1500 mg supplemental calcium/d alone, supplemental calcium plus 1100 IU vitamin D3/d, or placebo during a follow-up of four years [71]. In contrast, this trial found that those women on vitamin D supplementation had a lower risk of cancer, compared to the placebo group when the analysis was confined to cancers diagnosed after the first 12 months (RR: 0.23; 95% CI: 0.09-0.60). No statistical analyses were performed for specific types of cancer [71].
Discussion
To date no mediation analyses have been performed for the effect of obesity on cancer risk through vitamin D. Even though we could not find the question addressed in one single study, it is still of interest to discuss study design and methodology of studies published on any of the three questions, (Figure 1) to interpret the validity of a potential mediation effect of vitamin D [72].
Obesity and cancer
The majority of meta-analyses included in our review reported positive associations between obesity and risk of cancer, showing that the strength of this association varies between cancer sites, sex, and in breast cancer, the menopausal status. The World Cancer Research Fund (WCRF) suggests that obesity is associated with increased risk of oesophageal adenocarcinoma, pancreatic, colorectal, postmenopausal breast, endometrial and renal cancer [73].
There are several molecular mechanisms suggested to explain the increased risk of cancer in obese people. The most commonly postulated being the “insulin–cancer hypothesis” [74], suggesting that obesity results in chronic hyperinsulinaemia. Prolonged hyperinsulinaemia leads to raised insulin like growth factor 1 (IGF-1) levels, which are known to produce cellular changes leading to carcinogenesis via increased mitosis and reduced apoptosis. Secondly, in hormonally-driven cancers, such as endometrial and post-menopausal breast cancer, the increased risk may be partly explained by an increase in circulating levels of sex steroid hormones. In the post-menopausal state, the majority of oestrogen is derived from adipose tissue rather than from the ovaries, potentially explaining the discrepancy between pre- and post-menopausal women. Thirdly, obesity is thought to result in a state of chronic inflammation and this has an effect on the cytokine microenvironment. These changes lead to an increase in tumour cell motility, invasion and metastasis. The change in the cytokine milieu has been suggested as a possible mechanism in several cancers including post-menopausal breast cancer [75].
The majority of the meta-analyses in our literature review included a substantial number of studies, with consistent study design. However, the meta-analysis on endometrial cancer [51] only included five studies of which some used other markers than BMI to define obesity (i.e. waist circumference). None of the studies to date included additional information on vitamin D status.
In summary, there is consistent accumulating evidence for an association between obesity and risk of certain cancer with several suggested molecular mechanisms that can potentially explain these raised risks. However, the role of vitamin D is not addressed in detail in these studies.
Obesity and vitamin D
To our knowledge this is the largest meta-analysis to date on the association between circulating vitamin D levels and obesity. The pooled estimates suggest an inverse relationship between vitamin D and obesity.
The possible relationship between vitamin D and obesity was firstly described by Rosenstreich et al. in 1971 [76], who suggested that adipose tissue serves as a large storage site for vitamin D to protect against toxicity from vitamin overdose. The inverse association between obesity and vitamin D is thus thought to be a result of increased metabolic clearance in adipose tissue [77]. However, it has recently been suggested that this association is more complex since bariatric surgery solely has temporary effect on improving circulating vitamin D levels [78]. It is also postulated that obese individuals are less likely to engage in outdoor physical activity and dress differently than non-obese individuals, hence leading to decreased sun exposure [79, 80]. Wortsman et al. have shown that the bioavailability of cutaneously synthesised vitamin D decreases by >50% in obese people [81]. Even though exposure to sunlight is the main source of vitamin D synthesis [82, 83], its ultraviolet radiation is also known to increase risk of developing malignant melanoma of the skin [83]. In general, epidemiological studies have described that the highest incidence of melanoma is seen in fair-skinned population living closest to the equator [82, 84]. Within this population the highest risk is seen in those who report sunburn or intermittent sun exposure [85–87]. Furthermore, Newton-Bishop et al. found that low vitamin D levels were associated with a thicker and more aggressive melanoma, with a poorer outcome [88]. Overall, vitamin D levels are known to be lower in obese individuals and several studies have observed that increased BMI is associated with an increased risk of developing melanoma [89–91]. However, to date it has not been clarified whether the risk of melanoma in obese individuals is due to lower vitamin D levels associated with high BMI or less sun exposure.
Furthermore, certain vitamin D receptor (VDR) polymorphisms are associated with obesity [92, 93]. Upon ligation with calcitriol, the VDR couples with the retinoid X receptor (RXR) forming the VDR/RXR complex. This complex then further recruits other molecules, and finally binds to vitamin D response elements in the nucleus to activate the transcription of vitamin D target genes [92, 93]. Preclinical studies report expression of human VDR in mature mice adipocytes. This results in increased adipose mass and decreased energy expenditure [94] and expression of VDR in preadipocyte cell lines; this inhibits adipocyte differentiation [95]. A positive association between obesity and the Taq1 gene was also reported in a Greek case–control study [96].
In contrast, some suggest that low vitamin D itself promotes obesity. Kong and Li demonstrated that vitamin D levels may block the expression of downstream adipocyte components such as fatty acid synthase, which consequently suppresses adipogenesis [97]. One interventional study investigated the effects of vitamin D on weight loss and showed that those with higher baseline vitamin D experienced a greater degree of weight loss than those with lower baseline vitamin D [98].
In conclusion, our meta-analysis reports a modest inverse association between obesity and low vitamin D levels. The underlying biological mechanisms are unknown. The majority of studies point towards the hypothesis that, vitamin D stored in fat tissue increases local vitamin D concentrations causing activation of the VDR in adipocytes. This may lead to low energy usage and further promotion of obesity [94].
Vitamin D and cancer
In this literature review only those meta-analyses focusing on colorectal cancer found a consistent inverse association between circulating vitamin D levels and cancer risk [54–59]. In contrast, of the two completed clinical trials for which results are published to date, one showed no effect on colorectal cancer risk and one showed a protective effect for all cancer risk [70, 71].
A protective effect of vitamin D in colorectal cancer was first reported by Garland and Garland [99]. Despite the inconsistency in epidemiological findings [54–61, 64–68], there is preclinical evidence linking vitamin D and cancer, suggesting that vitamin D has anti-proliferative effects via mechanisms such as G0/G1 arrest, differentiation, and induction of apoptosis [100].
More specifically, it is suggested that vitamin D has anti-tumour effects through its binding with the VDR. Several animal and cell culture models showed that VDR plays a key role in the anticancer effects of circulating vitamin D [9–11]. For instance, it has been reported that downregulation of VDR correlates with poor prognosis in colon cancer [101], suggesting that some of the discrepancy observed in epidemiological studies can be explained through gene polymorphisms [102]. VDR polymorphisms have been associated, both positively and inversely, with risk of cancer depending on the type of cancer, polymorphism, and other factors such as sun exposure or circulating vitamin D levels [8, 103]. For instance, a meta-analysis for prostate cancer found no association between the recessive genotype and the risk of prostate cancer relative to the dominant genotype of Fok1 [104]. To date, the importance of the role of VDR polymorphisms in carcinogenesis is unclear [101], but when analysed with additional factors like VDR haplotype combinations, vitamin D serum levels and other confounders, polymorphisms have been shown to play an important factor in cancer prognosis [105–107].
Interestingly, several parts of the immune system (i.e. macrophages, neutrophils, or natural killer cells) also express the VDR, but the related effects remain to be elucidated [12]. It has for instance been suggested that vitamin D can weaken antigen presentation by dendritic cells, which results in suppression of their capacity to activate T cells. Furthermore, activation of the VDR promotes a shift towards T helper 2 responses, leading to antibody-mediated immunity and promoting a chronic state of disease [108, 109]. Hence, it is plausible that vitamin D has an immunosuppressive effect, which leaves tumour cells without the necessary immunosurveillance to stop them from proliferating. Thus, this suggests that the above-described potential anti-cancer effect of vitamin D most likely occurs through different mechanisms than the immune system. Most literature to date on vitamin D and the immune system has focused on autoimmune and infectious diseases, with scarce literature focusing on cancer.
In 2008, the International Agency for Research on Cancer concluded that evidence for an association between vitamin D and cancer was inconclusive, and highlighted the need for a clinical trial with specific focus on vitamin D and colorectal cancer [101]. The inconsistent findings from two trials for which results are published to date [70, 71] may be explained by the lower dose of vitamin D in the first study (i.e. 400 IU vs. 1100 IU). Furthermore, baseline vitamin D levels were lower in the second trial (i.e. 42 nmol/L vs. 71.8 nmol/L). Thus, despite the large amount of preclinical studies trying to establish a link between vitamin D and cancer, the contradictive findings from large epidemiological studies indicate that it is prudent to wait for more results from the 34 currently on-going trials to draw a reliable conclusion.
Is vitamin D a mediator for the association between obesity and cancer?
When assessing the three conditions required for vitamin D to be a mediator we found only partial fulfilment [110]. The literature shows consistent evidence for an association between vitamin D and obesity. However, there was lack of studies showing a consistent link between vitamin D and cancer after adjustment for obesity. To date, only two clinical trials have published their results with inconsistent findings. Furthermore, to our knowledge no study has assessed the mediation effect of vitamin D by quantifying the extent of obesity on cancer, which could be explained by a potential mediator.
Several other difficulties occur when assessing the mediation effect of vitamin D in the context of obesity and cancer. Dichotomisation of vitamin D exposure (low versus normal) could lead to misclassification in exposure levels. Those with extreme high values of vitamin D may have been included in the “normal” group. Hence, bias can occur when there is misclassification of the mediator [13]. Studies to date have used different cut-offs to define vitamin D deficiency, which can potentially be addressed with a dose–response assessment of this mediator. Unfortunately, it was not possible in this meta-analysis to use dose–response data [111] as the number of relevant studies available to date was small, and the qualitative classifications of circulating vitamin D levels varied. Furthermore, the effects of dietary supplements on circulating vitamin D levels needs to be accounted for, and very few studies took this into account [112]. The latter does not necessarily affect blood levels of vitamin D, but it may influence the biological role of vitamin D. Within-person variation may also affect the results of our meta-analysis, as only one measurement in time might not be representative of a person’s average vitamin D level. Moreover, it is important to address potential important confounders for the different associations studied [13, 72]. For instance, when evaluating the effect of the mediator (vitamin D) on the outcome (cancer), one has to consider age, sex, use of dietary supplements, ethnic variations, calcium intake and sun exposure [113], as they may be effect modifiers for the association between obesity and vitamin D. It has been argued that it is also important to address the strength of the association between these mediator-exposure confounders and both the exposure (obesity) and the outcome (cancer) [13]. With respect to the mediation effect of vitamin D, one also needs to evaluate whether there is a potential interaction affecting the link between the exposure (obesity) and the mediator (vitamin D) [13]. Effect modification may also have an effect on the link between the mediator (vitamin D) and the outcome (cancer), as is suggested by the different polymorphisms affecting the VDR [8].
Additionally, the current systematic literature reviews are prone to the heterogeneity related to observational studies. For example, for the studies focused on vitamin D and obesity the included studies recruited adults residing in a particular town [114], from medical centres [115–117], from sample surveys [2, 118], and those undergoing bariatric surgery [53]. Children were recruited from schools [119, 120], hospitals [121, 122], and sample surveys [123]. Vitamin D levels were measured using either an immunoassay [2, 53, 114, 115, 118–121, 123] or a high-performance liquid chromatography [116, 122]. Anthropometric data, including weight, height, waist circumference and BMI, were recorded for all participants [119, 120, 122]. Furthermore, information on dietary, physical activity and sun exposure were collected either by parental report during in-person interviews [123], and interview-administered questionnaires [114, 122]. These questionnaires may be subject to recall bias, as participants may not always give accurate data [124, 125] due to the time interval, degree of detail, personal characteristics, significance of events, social desirability or interviewing techniques [126]. Furthermore, despite proven validation, many food questionnaires have been found to be imprecise [127], due to the fact that people tend to answer these type of questions based on what their dietary routines are, more than on the real consumption. These memories are usually influenced by sex, age, and concerns about weight or body image [128].
A strength of these systematic reviews and meta-analysis is that we made all possible efforts to include all relevant publications available to date through various sources, including grey literature, and the two main online databases (PubMed and Embase). In addition, clearly defined objective criteria for exposure, outcome, and other study characteristics were specified a priori.
Conclusion
To understand how vitamin D may play a role in the association between obesity and carcinogenesis, we assessed the strength of these three associations: 1) There was a consistent positive association between obesity and cancer with relative risks varying between 1.10 and 1.90 when addressing the existing literature; (2) Our new meta-analysis illustrated an association as strong as 1.50 between obesity and low vitamin D levels; (3) The literature for vitamin D status and cancer risk only showed consistent evidence for an inverse association with colorectal cancer. From these reviews, it seems that the significance of the mediating role of vitamin D in the biological pathways linking obesity and cancer is low. This review emphasises that further research specifically addressing the relationship between obesity, vitamin D and cancer risk in one study is needed.
Abbreviations
- VDR:
-
Vitamin D receptor
- BMI:
-
Body mass index
- RR:
-
Relative risk
- WCRF:
-
World cancer research fund
- IGF-1:
-
Insulin like growth factor 1
- RXR:
-
Retinoid X receptor
- ca/co:
-
Case–control.
References
Lagunova Z, Porojnicu AC, Grant WB, Bruland O, Moan JE: Obesity and increased risk of cancer: does decrease of serum 25-hydroxyvitamin D level with increasing body mass index explain some of the association?. Mol Nutr Food Res. 2010, 54: 1127-1133.
Mai XM, Chen Y, Camargo CA, Langhammer A: Cross-sectional and prospective cohort study of serum 25-hydroxyvitamin D level and obesity in adults: the HUNT study. Am J Epidemiol. 2012, 175: 1029-1036.
Obesity Fact File. [http://www.who.int/features/factfiles/obesity/facts/en/index1.html]
Lew EA, Garfinkel L: Variations in mortality by weight among 750,000 men and women. J Chronic Dis. 1979, 32: 563-576.
Carroll KK: Obesity as a risk factor for certain types of cancer. Lipids. 1998, 33: 1055-1059.
Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ: Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N Engl J Med. 2003, 348: 1625-1638.
Parkin DM, Boyd L: 8. Cancers attributable to overweight and obesity in the UK in 2010. Br J Cancer. 2011, 105 (Suppl 2): S34-S37.
Kostner K, Denzer N, Muller CS, Klein R, Tilgen W, Reichrath J: The relevance of vitamin D receptor (VDR) gene polymorphisms for cancer: a review of the literature. Anticancer Res. 2009, 29: 3511-3536.
Costa JL, Eijk PP, van de Wiel MA, Ten Berge D, Schmitt F, Narvaez CJ, Welsh J, Ylstra B: Anti-proliferative action of vitamin D in MCF7 is still active after siRNA-VDR knock-down. BMC Genomics. 2009, 10: 499-
Koren R, Wacksberg S, Weitsman GE, Ravid A: Calcitriol sensitizes colon cancer cells to H2O2-induced cytotoxicity while inhibiting caspase activation. J Steroid Biochem Mol Biol. 2006, 101: 151-160.
Zinser GM, Welsh J: Effect of Vitamin D3 receptor ablation on murine mammary gland development and tumorigenesis. J Steroid Biochem Mol Biol. 2004, 89–90: 433-436.
Cantorna MT, Zhu Y, Froicu M, Wittke A: Vitamin D status, 1,25-dihydroxyvitamin D3, and the immune system. Am J Clin Nutr. 2004, 80: 1717S-1720S.
Richiardi L, Bellocco R, Zugna D: Mediation analysis in epidemiology: methods, interpretation and bias. Int J Epidemiol. 2013, 42: 1511-1519.
Cole SR, Hernan MA: Fallibility in estimating direct effects. Int J Epidemiol. 2002, 31: 163-165.
Morton ML, Thompson CL: Decreasing 25-hydroxy-vitamin D levels account for portion of the effect of increasing body mass index on breast cancer mortality. Mol Nutr Food Res. 2013, 57: 260-266.
Abbas S, Linseisen J, Rohrmann S, Chang-Claude J, Peeters PH, Engel P, Brustad M, Lund E, Skeie G, Olsen A, Tjønneland A, Overvad K, Boutron-Ruault MC, Clavel-Chapelon F, Fagherazzi G, Kaaks R, Boeing H, Buijsse B, Adarakis G, Ouranos V, Trichopoulou A, Masala G, Krogh V, Mattiello A, Tumino R, Sacerdote C, Buckland G, Suárez MV, Sánchez MJ, Chirlaque MD: Dietary intake of vitamin D and calcium and breast cancer risk in the European Prospective Investigation into Cancer and Nutrition. Nutr Cancer. 2013, 65: 178-187.
Rigotti NA: Cigarette smoking and body weight. N Engl J Med. 1989, 320: 931-933.
Knekt P, Heliovaara M, Rissanen A, Aromaa A, Seppanen R, Teppo L, Pukkala E: Leanness and lung-cancer risk. Int J Cancer. 1991, 49: 208-213.
Rauscher GH, Mayne ST, Janerich DT: Relation between body mass index and lung cancer risk in men and women never and former smokers. Am J Epidemiol. 2000, 152: 506-513.
Yang Y, Dong J, Sun K, Zhao L, Zhao F, Wang L, Jiao Y: Obesity and incidence of lung cancer: a meta-analysis. Int J Cancer. 2013, 132: 1162-1169.
ClinicalTrials.gov. [http://clinicaltrials.gov/]
Ma Y, Yang Y, Wang F, Zhang P, Shi C, Zou Y, Qin H: Obesity and risk of colorectal cancer: a systematic review of prospective studies. PLoS One. 2013, 8: e53916-
Matsuo K, Mizoue T, Tanaka K, Tsuji I, Sugawara Y, Sasazuki S, Nagata C, Tamakoshi A, Wakai K, Inoue M, Tsugane S, Development and Evaluation of Cancer Prevention Strategies in Japan: Association between body mass index and the colorectal cancer risk in Japan: pooled analysis of population-based cohort studies in Japan. Ann Oncol. 2012, 23: 479-490.
Ning Y, Wang L, Giovannucci EL: A quantitative analysis of body mass index and colorectal cancer: findings from 56 observational studies. Obes Rev. 2010, 11: 19-30.
Harriss DJ, Atkinson G, George K, Cable NT, Reilly T, Haboubi N, Zwahlen M, Egger M, Renehan AG, Group CC: Lifestyle factors and colorectal cancer risk (1): systematic review and meta-analysis of associations with body mass index. Colorectal Dis. 2009, 11: 547-563.
Moghaddam AA, Woodward M, Huxley R: Obesity and risk of colorectal cancer: a meta-analysis of 31 studies with 70,000 events. Cancer Epidemiol Biomarkers Prev. 2007, 16: 2533-2547.
Dai Z, Xu YC, Niu L: Obesity and colorectal cancer risk: a meta-analysis of cohort studies. World J Gastroenterol. 2007, 13: 4199-4206.
Larsson SC, Wolk A: Obesity and colon and rectal cancer risk: a meta-analysis of prospective studies. Am J Clin Nutr. 2007, 86: 556-565.
Hoyo C, Cook MB, Kamangar F, Freedman ND, Whiteman DC, Bernstein L, Brown LM, Risch HA, Ye W, Sharp L, Wu AH, Ward MH, Casson AG, Murray LJ, Corley DA, Nyrén O, Pandeya N, Vaughan TL, Chow WH, Gammon MD: Body mass index in relation to oesophageal and oesophagogastric junction adenocarcinomas: a pooled analysis from the International BEACON Consortium. Int J Epidemiol. 2012, 41: 1706-1718.
Yang P, Zhou Y, Chen B, Wan HW, Jia GQ, Bai HL, Wu XT: Overweight, obesity and gastric cancer risk: results from a meta-analysis of cohort studies. Eur J Cancer. 2009, 45: 2867-2873.
Larsson SC, Wolk A: Obesity and the risk of gallbladder cancer: a meta-analysis. Br J Cancer. 2007, 96: 1457-1461.
Kubo A, Corley DA: Body mass index and adenocarcinomas of the esophagus or gastric cardia: a systematic review and meta-analysis. Cancer Epidemiol Biomarkers Prev. 2006, 15: 872-878.
Rui R, Lou J, Zou L, Zhong R, Wang J, Xia D, Wang Q, Li H, Wu J, Lu X, Li C, Liu L, Xia J, Xu H: Excess body mass index and risk of liver cancer: a nonlinear dose–response meta-analysis of prospective studies. PLoS One. 2012, 7: e44522-
Chen Y, Wang X, Wang J, Yan Z, Luo J: Excess body weight and the risk of primary liver cancer: an updated meta-analysis of prospective studies. Eur J Cancer. 2012, 48: 2137-2145.
Larsson SC, Wolk A: Overweight, obesity and risk of liver cancer: a meta-analysis of cohort studies. Br J Cancer. 2007, 97: 1005-1008.
Wang Y, Wang B, Shen F, Fan J, Cao H: Body mass index and risk of primary liver cancer: a meta-analysis of prospective studies. Oncologist. 2012, 17: 1461-1468.
Aune D, Greenwood DC, Chan DS, Vieira R, Vieira AR, Navarro Rosenblatt DA, Cade JE, Burley VJ, Norat T: Body mass index, abdominal fatness and pancreatic cancer risk: a systematic review and non-linear dose–response meta-analysis of prospective studies. Ann Oncol. 2012, 23: 843-852.
Genkinger JM, Spiegelman D, Anderson KE, Bernstein L, van den Brandt PA, Calle EE, English DR, Folsom AR, Freudenheim JL, Fuchs CS, Giles GG, Giovannucci E, Horn-Ross PL, Larsson SC, Leitzmann M, Männistö S, Marshall JR, Miller AB, Patel AV, Rohan TE, Stolzenberg-Solomon RZ, Verhage BA, Virtamo J, Willcox BJ, Wolk A, Ziegler RG, Smith-Warner SA: A pooled analysis of 14 cohort studies of anthropometric factors and pancreatic cancer risk. Int J Cancer. 2011, 129: 1708-1717.
Jiao L, Berrington de Gonzalez A, Hartge P, Pfeiffer RM, Park Y, Freedman DM, Gail MH, Alavanja MC, Albanes D, Beane Freeman LE, Chow WH, Huang WY, Hayes RB, Hoppin JA, Ji BT, Leitzmann MF, Linet MS, Meinhold CL, Schairer C, Schatzkin A, Virtamo J, Weinstein SJ, Zheng W, Stolzenberg-Solomon RZ: Body mass index, effect modifiers, and risk of pancreatic cancer: a pooled study of seven prospective cohorts. Cancer Causes Control. 2010, 21: 1305-1314.
Berrington de Gonzalez A, Sweetland S, Spencer E: A meta-analysis of obesity and the risk of pancreatic cancer. Br J Cancer. 2003, 89: 519-523.
Mathew A, George PS, Ildaphonse G: Obesity and kidney cancer risk in women: a meta-analysis (1992–2008). Asian Pac J Cancer Prev. 2009, 10: 471-478.
Bergstrom A, Hsieh CC, Lindblad P, Lu CM, Cook NR, Wolk A: Obesity and renal cell cancer–a quantitative review. Br J Cancer. 2001, 85: 984-990.
MacInnis RJ, English DR: Body size and composition and prostate cancer risk: systematic review and meta-regression analysis. Cancer Causes Control. 2006, 17: 989-1003.
Discacciati A, Orsini N, Wolk A: Body mass index and incidence of localized and advanced prostate cancer–a dose–response meta-analysis of prospective studies. Ann Oncol. 2012, 23: 1665-1671.
Qin Q, Xu X, Wang X, Zheng XY: Obesity and risk of bladder cancer: a meta-analysis of cohort studies. Asian Pac J Cancer Prev. 2013, 14: 3117-3121.
Pierobon M, Frankenfeld CL: Obesity as a risk factor for triple-negative breast cancers: a systematic review and meta-analysis. Breast Cancer Res Treat. 2013, 137: 307-314.
Cheraghi Z, Poorolajal J, Hashem T, Esmailnasab N, Irani AD: Effect of body mass index on breast cancer during premenopausal and postmenopausal periods: a meta-analysis. PLoS One. 2012, 7: e51446-
Key TJ, Appleby PN, Reeves GK, Roddam A, Dorgan JF, Longcope C, Stanczyk FZ, Stephenson HE, Falk RT, Miller R, Schatzkin A, Allen DS, Fentiman IS, Key TJ, Wang DY, Dowsett M, Thomas HV, Hankinson SE, Toniolo P, Akhmedkhanov A, Koenig K, Shore RE, Zeleniuch-Jacquotte A, Berrino F, Muti P, Micheli A, Krogh V, Sieri S, Pala V, Venturelli E: Body mass index, serum sex hormones, and breast cancer risk in postmenopausal women. J Natl Cancer Inst. 2003, 95: 1218-1226.
Olsen CM, Green AC, Whiteman DC, Sadeghi S, Kolahdooz F, Webb PM: Obesity and the risk of epithelial ovarian cancer: a systematic review and meta-analysis. Eur J Cancer. 2007, 43: 690-709.
Renehan AG, Tyson M, Egger M, Heller RF, Zwahlen M: Body-mass index and incidence of cancer: a systematic review and meta-analysis of prospective observational studies. Lancet. 2008, 371: 569-578.
Esposito K, Chiodini P, Capuano A, Bellastella G, Maiorino MI, Giugliano D: Metabolic syndrome and endometrial cancer: a meta-analysis. Endocrine. 2014, 45: 28-36.
Sergentanis TN, Antoniadis AG, Gogas HJ, Antonopoulos CN, Adami HO, Ekbom A, Petridou ET: Obesity and risk of malignant melanoma: a meta-analysis of cohort and case–control studies. Eur J Cancer. 2013, 49: 642-657.
Goldner WS, Stoner JA, Thompson J, Taylor K, Larson L, Erickson J, McBride C: Prevalence of vitamin D insufficiency and deficiency in morbidly obese patients: a comparison with non-obese controls. Obes Surg. 2008, 18: 145-150.
Gorham ED, Garland CF, Garland FC, Grant WB, Mohr SB, Lipkin M, Newmark HL, Giovannucci E, Wei M, Holick MF: Optimal vitamin D status for colorectal cancer prevention: a quantitative meta analysis. Am J Prev Med. 2007, 32: 210-216.
Touvier M, Chan DS, Lau R, Aune D, Vieira R, Greenwood DC, Kampman E, Riboli E, Hercberg S, Norat T: Meta-analyses of vitamin D intake, 25-hydroxyvitamin D status, vitamin D receptor polymorphisms, and colorectal cancer risk. Cancer Epidemiol Biomarkers Prev. 2011, 20: 1003-1016.
Lee JE, Li H, Chan AT, Hollis BW, Lee IM, Stampfer MJ, Wu K, Giovannucci E, Ma J: Circulating levels of vitamin D and colon and rectal cancer: the Physicians’ Health Study and a meta-analysis of prospective studies. Cancer Prev Res (Phila). 2011, 4: 735-743.
Yin L, Grandi N, Raum E, Haug U, Arndt V, Brenner H: Meta-analysis: longitudinal studies of serum vitamin D and colorectal cancer risk. Aliment Pharmacol Ther. 2009, 30: 113-125.
Gandini S, Boniol M, Haukka J, Byrnes G, Cox B, Sneyd MJ, Mullie P, Autier P: Meta-analysis of observational studies of serum 25-hydroxyvitamin D levels and colorectal, breast and prostate cancer and colorectal adenoma. Int J Cancer. 2011, 128: 1414-1424.
Ma Y, Zhang P, Wang F, Yang J, Liu Z, Qin H: Association between vitamin D and risk of colorectal cancer: a systematic review of prospective studies. J Clin Oncol. 2011, 29: 3775-3782.
Stolzenberg-Solomon RZ, Jacobs EJ, Arslan AA, Qi D, Patel AV, Helzlsouer KJ, Weinstein SJ, McCullough ML, Purdue MP, Shu XO, Snyder K, Virtamo J, Wilkins LR, Yu K, Zeleniuch-Jacquotte A, Zheng W, Albanes D, Cai Q, Harvey C, Hayes R, Clipp S, Horst RL, Irish L, Koenig K, Le Marchand L, Kolonel LN: Circulating 25-hydroxyvitamin D and risk of pancreatic cancer: Cohort Consortium Vitamin D Pooling Project of Rarer Cancers. Am J Epidemiol. 2010, 172: 81-93.
Gallicchio L, Moore LE, Stevens VL, Ahn J, Albanes D, Hartmuller V, Setiawan VW, Helzlsouer KJ, Yang G, Xiang YB, Shu XO, Snyder K, Weinstein SJ, Yu K, Zeleniuch-Jacquotte A, Zheng W, Cai Q, Campbell DS, Chen Y, Chow WH, Horst RL, Kolonel LN, McCullough ML, Purdue MP, Koenig KL: Circulating 25-hydroxyvitamin D and risk of kidney cancer: Cohort Consortium Vitamin D Pooling Project of Rarer Cancers. Am J Epidemiol. 2010, 172: 47-57.
Gilbert R, Martin RM, Beynon R, Harris R, Savovic J, Zuccolo L, Bekkering GE, Fraser WD, Sterne JA, Metcalfe C: Associations of circulating and dietary vitamin D with prostate cancer risk: a systematic review and dose–response meta-analysis. Cancer Causes Control. 2011, 22: 319-340.
Yin L, Raum E, Haug U, Arndt V, Brenner H: Meta-analysis of longitudinal studies: Serum vitamin D and prostate cancer risk. Cancer Epidemiol. 2009, 33: 435-445.
Chen P, Li M, Gu X, Liu Y, Li X, Li C, Wang Y, Xie D, Wang F, Yu C, Li J, Chen X, Chu R, Zhu J, Ou Z, Wang H: Higher blood 25(OH)D level may reduce the breast cancer risk: evidence from a Chinese population based case–control study and meta-analysis of the observational studies. PLoS One. 2013, 8: e49312-
Yin L, Grandi N, Raum E, Haug U, Arndt V, Brenner H: Meta-analysis: serum vitamin D and breast cancer risk. Eur J Cancer. 2010, 46: 2196-2205.
Chen P, Hu P, Xie D, Qin Y, Wang F, Wang H: Meta-analysis of vitamin D, calcium and the prevention of breast cancer. Breast Cancer Res Treat. 2010, 121: 469-477.
Bauer SR, Hankinson SE, Bertone-Johnson ER, Ding EL: Plasma vitamin D levels, menopause, and risk of breast cancer: dose–response meta-analysis of prospective studies. Medicine (Baltimore). 2013, 92: 123-131.
Yin L, Grandi N, Raum E, Haug U, Arndt V, Brenner H: Meta-analysis: Circulating vitamin D and ovarian cancer risk. Gynecol Oncol. 2011, 121: 369-375.
Yin L, Ordonez-Mena JM, Chen T, Schottker B, Arndt V, Brenner H: Circulating 25-hydroxyvitamin D serum concentration and total cancer incidence and mortality: a systematic review and meta-analysis. Prev Med. 2013, 57: 753-764.
Wactawski-Wende J, Kotchen JM, Anderson GL, Assaf AR, Brunner RL, O’Sullivan MJ, Margolis KL, Ockene JK, Phillips L, Pottern L, Prentice RL, Robbins J, Rohan TE, Sarto GE, Sharma S, Stefanick ML, Van Horn L, Wallace RB, Whitlock E, Bassford T, Beresford SA, Black HR, Bonds DE, Brzyski RG, Caan B, Chlebowski RT, Cochrane B, Garland C, Gass M, Hays J: Calcium plus vitamin D supplementation and the risk of colorectal cancer. N Engl J Med. 2006, 354: 684-696.
Lappe JM, Travers-Gustafson D, Davies KM, Recker RR, Heaney RP: Vitamin D and calcium supplementation reduces cancer risk: results of a randomized trial. Am J Clin Nutr. 2007, 85: 1586-1591.
Gelfand LA, Baraldi AN: Height as a sex-cancer mediator? Interpret with caution. J Natl Cancer Inst. 2013, 105: 843-844.
McMichael AJ: Food, nutrition, physical activity and cancer prevention. Authoritative report from World Cancer Research Fund provides global update. Public Health Nutr. 2008, 11: 762-763.
Renehan AG, Frystyk J, Flyvbjerg A: Obesity and cancer risk: the role of the insulin-IGF axis. Trends Endocrinol Metab. 2006, 17: 328-336.
Gilbert CA, Slingerland JM: Cytokines, obesity, and cancer: new insights on mechanisms linking obesity to cancer risk and progression. Annu Rev Med. 2013, 64: 45-57.
Rosenstreich SJ, Rich C, Volwiler W: Deposition in and release of vitamin D3 from body fat: evidence for a storage site in the rat. J Clin Invest. 1971, 50: 679-687.
Blum M, Dolnikowski G, Seyoum E, Harris SS, Booth SL, Peterson J, Saltzman E, Dawson-Hughes B: Vitamin D(3) in fat tissue. Endocrine. 2008, 33: 90-94.
Lin E, Armstrong-Moore D, Liang Z, Sweeney JF, Torres WE, Ziegler TR, Tangpricha V, Gletsu-Miller N: Contribution of adipose tissue to plasma 25-hydroxyvitamin D concentrations during weight loss following gastric bypass surgery. Obesity (Silver Spring). 2011, 19: 588-594.
Song Q, Sergeev IN: Calcium and vitamin D in obesity. Nutr Res Rev. 2012, 25: 130-141.
Kull M, Kallikorm R, Lember M: Body mass index determines sunbathing habits: implications on vitamin D levels. Intern Med J. 2009, 39: 256-258.
Wortsman J, Matsuoka LY, Chen TC, Lu Z, Holick MF: Decreased bioavailability of vitamin D in obesity. Am J Clin Nutr. 2000, 72: 690-693.
Field S, Davies J, Bishop DT, Newton-Bishop JA: Vitamin D and melanoma. Dermatoendocrinol. 2013, 5: 121-129.
Lindqvist PG, Epstein E, Landin-Olsson M, Ingvar C, Nielsen K, Stenbeck M, Olsson H: Avoidance of sun exposure is a risk factor for all-cause mortality: results from the Melanoma in Southern Sweden cohort. J Intern Med. 2014, 276: 77-86.
Oliveria SA, Saraiya M, Geller AC, Heneghan MK, Jorgensen C: Sun exposure and risk of melanoma. Arch Dis Child. 2006, 91: 131-138.
Chang YM, Barrett JH, Bishop DT, Armstrong BK, Bataille V, Bergman W, Berwick M, Bracci PM, Elwood JM, Ernstoff MS, Gallagher RP, Green AC, Gruis NA, Holly EA, Ingvar C, Kanetsky PA, Karagas MR, Lee TK, Le Marchand L, Mackie RM, Olsson H, Østerlind A, Rebbeck TR, Sasieni P, Siskind V, Swerdlow AJ, Titus-Ernstoff L, Zens MS, Newton-Bishop JA: Sun exposure and melanoma risk at different latitudes: a pooled analysis of 5700 cases and 7216 controls. Int J Epidemiol. 2009, 38: 814-830.
Elwood JM, Jopson J: Melanoma and sun exposure: an overview of published studies. Int J Cancer. 1997, 73: 198-203.
Gandini S, Sera F, Cattaruzza MS, Pasquini P, Picconi O, Boyle P, Melchi CF: Meta-analysis of risk factors for cutaneous melanoma: II. Sun exposure. Eur J Cancer. 2005, 41: 45-60.
Newton-Bishop JA, Beswick S, Randerson-Moor J, Chang YM, Affleck P, Elliott F, Chan M, Leake S, Karpavicius B, Haynes S, Kukalizch K, Whitaker L, Jackson S, Gerry E, Nolan C, Bertram C, Marsden J, Elder DE, Barrett JH, Bishop DT: Serum 25-hydroxyvitamin D3 levels are associated with breslow thickness at presentation and survival from melanoma. J Clin Oncol. 2009, 27: 5439-5444.
Gallus S, Naldi L, Martin L, Martinelli M, La Vecchia C, Oncology Study Group of the Italian Group for Epidemiologic Research in D: Anthropometric measures and risk of cutaneous malignant melanoma: a case–control study from Italy. Melanoma Res. 2006, 16: 83-87.
Dennis LK, Lowe JB, Lynch CF, Alavanja MC: Cutaneous melanoma and obesity in the Agricultural Health Study. Ann Epidemiol. 2008, 18: 214-221.
Randerson-Moor JA, Taylor JC, Elliott F, Chang YM, Beswick S, Kukalizch K, Affleck P, Leake S, Haynes S, Karpavicius B, Marsden J, Gerry E, Bale L, Bertram C, Field H, Barth JH, Silva Idos S, Swerdlow A, Kanetsky PA, Barrett JH, Bishop DT, Bishop JA: Vitamin D receptor gene polymorphisms, serum 25-hydroxyvitamin D levels, and melanoma: UK case–control comparisons and a meta-analysis of published VDR data. Eur J Cancer. 2009, 45: 3271-3281.
Picotto G, Liaudat AC, Bohl L, Tolosa de Talamoni N: Molecular aspects of vitamin D anticancer activity. Cancer Invest. 2012, 30: 604-614.
Lips P: Vitamin D physiology. Prog Biophys Mol Biol. 2006, 92: 4-8.
Wong KE, Kong J, Zhang W, Szeto FL, Ye H, Deb DK, Brady MJ, Li YC: Targeted expression of human vitamin D receptor in adipocytes decreases energy expenditure and induces obesity in mice. J Biol Chem. 2011, 286: 33804-33810.
Sato M, Hiragun A: Demonstration of 1 alpha,25-dihydroxyvitamin D3 receptor-like molecule in ST 13 and 3 T3 L1 preadipocytes and its inhibitory effects on preadipocyte differentiation. J Cell Physiol. 1988, 135: 545-550.
Vasilopoulos Y, Sarafidou T, Kotsa K, Papadimitriou M, Goutzelas Y, Stamatis C, Bagiatis V, Tsekmekidou X, Yovos JG, Mamuris Z: VDR TaqI is associated with obesity in the Greek population. Gene. 2013, 512: 237-239.
Kong J, Li YC: Molecular mechanism of 1,25-dihydroxyvitamin D3 inhibition of adipogenesis in 3 T3-L1 cells. Am J Physiol Endocrinol Metab. 2006, 290: E916-E924.
Earthman CP, Beckman LM, Masodkar K, Sibley SD: The link between obesity and low circulating 25-hydroxyvitamin D concentrations: considerations and implications. Int J Obes (Lond). 2012, 36: 387-396.
Garland CF, Comstock GW, Garland FC, Helsing KJ, Shaw EK, Gorham ED: Serum 25-hydroxyvitamin D and colon cancer: eight-year prospective study. Lancet. 1989, 2: 1176-1178.
Deeb KK, Trump DL, Johnson CS: Vitamin D signalling pathways in cancer: potential for anticancer therapeutics. Nat Rev Cancer. 2007, 7: 684-700.
World Health Organization: Vitamin D and Cancer. Volume 5. 2008, Geneva, Switzerland: World Health Organization
Li WH, Gu Z, Wang H, Nekrutenko A: Evolutionary analyses of the human genome. Nature. 2001, 409: 847-849.
Guy M, Lowe LC, Bretherton-Watt D, Mansi JL, Peckitt C, Bliss J, Wilson RG, Thomas V, Colston KW: Vitamin D receptor gene polymorphisms and breast cancer risk. Clin Cancer Res. 2004, 10: 5472-5481.
Ntais C, Polycarpou A, Ioannidis JP: Vitamin D receptor gene polymorphisms and risk of prostate cancer: a meta-analysis. Cancer Epidemiol Biomarkers Prev. 2003, 12: 1395-1402.
Sahin MO, Canda AE, Yorukoglu K, Mungan MU, Sade M, Kirkali Z: 1,25 Dihydroxyvitamin D(3) receptor expression in superficial transitional cell carcinoma of the bladder: a possible prognostic factor?. Eur Urol. 2005, 47: 52-57.
Zhou W, Heist RS, Liu G, Neuberg DS, Asomaning K, Su L, Wain JC, Lynch TJ, Giovannucci E, Christiani DC: Polymorphisms of vitamin D receptor and survival in early-stage non-small cell lung cancer patients. Cancer Epidemiol Biomarkers Prev. 2006, 15: 2239-2245.
Li C, Liu Z, Wang LE, Gershenwald JE, Lee JE, Prieto VG, Duvic M, Grimm EA, Wei Q: Haplotype and genotypes of the VDR gene and cutaneous melanoma risk in non-Hispanic whites in Texas: a case–control study. Int J Cancer. 2008, 122: 2077-2084.
Hewison M: Vitamin D and the immune system: new perspectives on an old theme. Endocrinol Metab Clin North Am. 2010, 39: 365-379. table of contents
Deluca HF, Cantorna MT: Vitamin D: its role and uses in immunology. FASEB J. 2001, 15: 2579-2585.
Ho GY, Wang T, Gunter MJ, Strickler HD, Cushman M, Kaplan RC, Wassertheil-Smoller S, Xue X, Rajpathak SN, Chlebowski RT, Vitolins MZ, Scherer PE, Rohan TE: Adipokines linking obesity with colorectal cancer risk in postmenopausal women. Cancer Res. 2012, 72: 3029-3037.
Bekkering GE, Harris RJ, Thomas S, Mayer AM, Beynon R, Ness AR, Harbord RM, Bain C, Smith GD, Sterne JA: How much of the data published in observational studies of the association between diet and prostate or bladder cancer is usable for meta-analysis?. Am J Epidemiol. 2008, 167: 1017-1026.
Lamberg-Allardt C, Brustad M, Meyer HE, Steingrimsdottir L: Vitamin D - a systematic literature review for the 5th edition of the Nordic Nutrition Recommendations. Food Nutr Res. 2013, 57:
Shui IM, Mucci LA, Kraft P, Tamimi RM, Lindstrom S, Penney KL, Nimptsch K, Hollis BW, Dupre N, Platz EA, Stampfer MJ, Giovannucci E: Vitamin D-related genetic variation, plasma vitamin D, and risk of lethal prostate cancer: a prospective nested case–control study. J Natl Cancer Inst. 2012, 104: 690-699.
Shea MK, Houston DK, Tooze JA, Davis CC, Johnson MA, Hausman DB, Cauley JA, Bauer DC, Tylavsky F, Harris TB, Kritchevsky SB, Health, Aging and Body Composition Study: Correlates and prevalence of insufficient 25-hydroxyvitamin D status in black and white older adults: the health, aging and body composition study. J Am Geriatr Soc. 2011, 59: 1165-1174.
Guasch A, Bullo M, Rabassa A, Bonada A, Del Castillo D, Sabench F, Salas-Salvado J: Plasma vitamin D and parathormone are associated with obesity and atherogenic dyslipidemia: a cross-sectional study. Cardiovasc Diabetol. 2012, 11: 149-
Al-Sultan AI, Amin TT, Abou-Seif MA, Al Naboli MR: Vitamin D, parathyroid hormone levels and insulin sensitivity among obese young adult Saudis. Eur Rev Med Pharmacol Sci. 2011, 15: 135-147.
Campagna AM, Settgast AM, Walker PF, DeFor TA, Campagna EJ, Plotnikoff GA: Effect of country of origin, age, and body mass index on prevalence of vitamin D deficiency in a US immigrant and refugee population. Mayo Clin Proc. 2013, 88: 31-37.
Hypponen E, Power C: Vitamin D status and glucose homeostasis in the 1958 British birth cohort: the role of obesity. Diabetes Care. 1958, 2006 (29): 2244-2246.
Cizmecioglu FM, Etiler N, Gormus U, Hamzaoglu O, Hatun S: Hypovitaminosis D in obese and overweight schoolchildren. J Clin Res Pediatr Endocrinol. 2008, 1: 89-96.
Elizondo-Montemayor L, Ugalde-Casas PA, Serrano-Gonzalez M, Cuello-Garcia CA, Borbolla-Escoboza JR: Serum 25-hydroxyvitamin d concentration, life factors and obesity in Mexican children. Obesity (Silver Spring). 2010, 18: 1805-1811.
Olson ML, Maalouf NM, Oden JD, White PC, Hutchison MR: Vitamin D deficiency in obese children and its relationship to glucose homeostasis. J Clin Endocrinol Metab. 2012, 97: 279-285.
Poomthavorn P, Saowan S, Mahachoklertwattana P, Chailurkit L, Khlairit P: Vitamin D status and glucose homeostasis in obese children and adolescents living in the tropics. Int J Obes (Lond). 2012, 36: 491-495.
Turer CB, Lin H, Flores G: Prevalence of vitamin D deficiency among overweight and obese US children. Pediatrics. 2013, 131: e152-e161.
Grimes DA, Schulz KF: Bias and causal associations in observational research. Lancet. 2002, 359: 248-252.
Neugebauer R, Ng S: Differential recall as a source of bias in epidemiologic research. J Clin Epidemiol. 1990, 43: 1337-1341.
Coughlin SS: Recall bias in epidemiologic studies. J Clin Epidemiol. 1990, 43: 87-91.
Boynton PM, Greenhalgh T: Selecting, designing, and developing your questionnaire. BMJ. 2004, 328: 1312-1315.
Drewnowski A: Diet image: a new perspective on the food-frequency questionnaire. Nutr Rev. 2001, 59: 370-372.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2407/14/712/prepub
Acknowledgements
This research was supported by the Experimental Cancer Medicine Centre at King’s College London, the National Institute for Health Research (NIHR) Biomedical Research Centre based at Guy’s and St Thomas’ NHS Foundation Trust and King’s College London, and Cancer Research UK (CRUK). The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR, the Department of Health, or CRUK.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The author(s) declare that they have no competing interests.
Authors’ contributions
TS and DC contributed equally and designed the study, analysed the data, interpreted analysis results and wrote the paper. CB analysed and interpreted data on relevant clinical trials, performed a literature review on vitamin D receptor and supplementation and edited the manuscript. JM, SR, SC, LH edited the manuscript. MVH conceived and designed the study, interpreted analysis results and edited the manuscript. All authors read and approved the final manuscript.
Thurkaa Shanmugalingam, Danielle Crawley contributed equally to this work.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
