
Abstract
Background
There have been sporadic reports about synchronous as well as metachronous gastric adenocarcinoma and primary gastric lymphoma. Many reports have dealt with metachronous gastric adenocarcinoma in mucosa-associated lymphoid tissue lymphoma of stomach. But to our knowledge, there have been no reports that document the increased incidence of metachronous gastric adenocarcinoma in patients with gastric diffuse large B-cell lymphoma. This retrospective study was conducted to estimate the incidence of metachronous gastric adenocarcinoma after primary gastric lymphoma treatment, especially in diffuse large B-cell lymphoma.
Methods
The retrospective cohort study of 139 primary gastric lymphoma patients treated with radiotherapy at our hospital. Mean observation period was 61.5 months (range: 3.7-124.6 months). Patients profile, characteristics of primary gastric lymphoma and metachronous gastric adenocarcinoma were retrieved from medical records. The risk of metachronous gastric adenocarcinoma was compared with the risk of gastric adenocarcinoma in Japanese population.
Results
There were 10 (7.2%) metachronous gastric adenocarcinoma patients after treatment of primary gastric lymphomas. It was quite high risk compared with the risk of gastric carcinoma in Japanese population of 54.7/100,000. Seven patients of 10 were diffuse large B-cell lymphoma and other 3 patients were mixed type of diffuse large B-cell lymphoma and mucosa associated lymphoid tissue lymphoma. Four patients of 10 metachronous gastric adenocarcinomas were signet-ring cell carcinoma and two patients died of gastric adenocarcinoma. Metachronous gastric adenocarcinoma may have a more malignant potential than sporadic gastric adenocarcinoma. Old age, Helicobacter pylori infection and gastric mucosal change of chronic gastritis and intestinal metaplasia were possible risk factors for metachronous gastric adenocarcinoma.
Conclusion
There was an increased risk of gastric adenocarcinoma after treatment of primary gastric lymphoma, especially of diffuse large B-cell lymphoma.
Similar content being viewed by others


Background
There have been sporadic reports about synchronous as well as metachronous gastric adenocarcinoma (GA) and primary gastric lymphoma (PGL) [1–16]. Regarding synchronous GA and PGL, Ishihama et al. reported that GA was seen synchronously in 3.3% of PGL patients (4/121 patients) [8]. Concerning the metachronous GA and PGL, the largest study is that of Capelle LG et al. which reported that metachronous GA risk was six times higher in the patients with gastric mucosa associated lymphoid tissue (MALT) lymphoma than in the Dutch general population [16]. Many reports have dealt with metachronous GA in MALT lymphoma of stomach. But to our knowledge, there have been no reports that document the increased incidence of metachronous GA in patients with gastric diffuse large B-cell lymphoma (DLBCL). This retrospective study was conducted to estimate the incidence of metachronous GA after PGL treatment, especially in DLBCL.
Methods
The radiation oncology department database from 2000 to 2010 was searched for PGL patients who underwent radiotherapy. Patient’s profiles at the time of PGL diagnosis (age, sex, lymphoma histology, stage, treatment and outcome) were retrieved retrospectively. After treatment of PGL, patients underwent regular follow-ups including endoscopic examinations and CT scannings. The date of GA diagnosis, interval between PGL and GA, stage of GA, treatment of GA and outcome were also investigated. One of the authors, an experienced gastrointestinal pathologist, reviewed the biopsy slides at the time of PGL and GA diagnosis and the presence of atrophic gastritis and intestinal metaplasia was diagnosed. In the 10 patients with metachronous GA after PGL, the presence of Helicobacter pylori (HP) infection was diagnosed retrospectively by pathology findings of the biopsy specimens or by results of the various laboratory tests.
Estimated risk of GA after PGL was calculated in comparison to the incidence of GA in Japanese population. Our institutional review board (National Cancer Center Institutional Review Board) approved this study.
Results
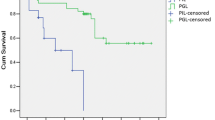
There were 139 patients with PGL (MALT lymphoma in 51 patients, DLBCL in 83, peripheral T-cell lymphoma (PTCL) in one, adult T-cell lymphoma (ATL) in 2 and follicular lymphoma (FL) in 2). Eighteen patients with MALT lymphoma were treated by radiation therapy because of the residual tumors after HP eradication, and the remaining 33 patients underwent radiation therapy because they were HP negative. Patient characteristics are shown in Table 1. Mean observation length was 61.5 months (range: 3.7-124.6 months). All PGLs in the current study were treated by radiotherapy and almost all patients except MALT were treated with chemo-radiotherapy. There were seen 10 patients with GA developed after treatment of PGL. No synchronous GA was found in this study. Tables 2 and 3 show the details of metachronous GA. The mean latent period between PGL and GA was 43.1 months (range: 7.9-90.8 months) (Figure 1). The histological types of GA were well differentiated adenocarcinoma in 4 patients, well to moderate differentiated adenocarcinoma in one, well to poorly differentiated adenocarcinoma in one, and signet-ring cell carcinoma in 4. In 9 patients, GA was classified as stage I and the remaining one was diagnosed as stage II. About the lymphoma histology, seven patients were classified as DLBCL and the remaining 3 showed a mixture of DLBCL and MALT lymphoma. For the GA, endoscopic resection was performed in 6 patients with no relapses. Four patients underwent surgery with relapses seen in 2 patients. Both of them succumbed to distant metastasis 9 and 37 months after surgery despite chemotherapy. Two- and 5-year overall survivals of GA were 90.0% and 75.0%. The 5-year overall survivals of DLBCL and MALT lymphoma were 89.6% and 97.7% respectively. Eight of the 83 DLBCL patients died, of which 5 were from non-lymphoma causes. Two of the 5 died from metachronous GA.

Incidence of GA/ all PGL and DLBCL. GA: gastric adenocarcinoma, PGL: primary gastric lymphoma, DLBCL: diffuse large B-cell lymphoma.
In the 10 patients with metachronous GA after PGL, mucosal findings at the time of PGL showed atrophic gastritis in 9 patients and intestinal metaplasia in 6. In contrast, the mucosa at the time of GA diagnosis showed atrophic gastritis and intestinal metaplasia in all 10 patients. Of 10 patients who developed GA after PGL, 5 had HP infection, and the remaining 5 patients had no information of HP infection but the background gastric mucosal changes of atrophic gastritis and intestinal metaplasia suggested possible presence of HP infection (Table 3).
Table 4 compared factors between the whole patients and the patients with metachronous GA. The incidence of metachronous GA was higher in the patients with age over 60 years, DLBCL, presence of HP infection, chemotherapy and stage II-IV with a statistical significance and the presence of intestinal metaplasia of gastric mucosa with a marginal significance (p=0.07).
The risk of metachronous GA after PGL was 10/139(=7.2%). If confined to DLBCL, the risk was 10/83(=12.0%) (Figure 1). The risk of GA in Japanese population is about 54.7/100,000 [17]. The relative risk was 131 (95% confidence interval: 68–251). If confined to DLBCL, the relative risk was 219 (95% confidence interval: 116–415).
Discussion
There were 10 patients developing metachronous GA after treatment of PGL. The risk of metachronous GA was higher in the patients with age over 60 years, DLBCL, HP infection, use of chemotherapy, Stage II-IV of PGL. In this study, MALT lymphomas were treated by radiation therapy after HP eradication as described in European Gastro-Intestinal Lymphoma Study (EGILS) group consensus report [18]. HP eradication and HP negative may explain that MALT lymphomas in this study showed no increased risk of metachronous GA. Increased risk of GA in Stage II-IV and patients treated with chemotherapy can be explained by the fact that only the patients with DLBCL showed advanced stages and treated by chemotherapy. Multivariate analysis to estimate factors for metachronous GA showed no statistical significance due to small number.
HP infection is well known in causing atrophic gastritis and intestinal metaplasia which might lead to GA. Not only the ongoing HP infection, but also radiation and chemotherapy could have contributed the mucosal change.
Old patients with primary gastric diffuse large B-cell lymphoma (PGDLBCL) who remains HP-infection positive and have mucosal change of atrophic gastritis and intestinal metaplasia should be followed up cautiously early to find metachronous GA and eradication of HP infection should be considered.
The increased risk of GA after PGL might be possibly explained by 2 theories. One is that damages to gastric mucosa by HP infection, chemotherapy, or radiotherapy increase GA risk [19–21], and the other is that GA remained undetected at the time of PGL because GA was so small [22–24]. Risk of treatment-related solid cancer increases more than 5 years after the primary treatment. The interval of GA and PGL was within 5 years in 7 patients. These patients with short interval may have undetected small GA at the time of PGL and the patients with longer interval could be caused by continuing HP infection and/or treatment.
To our knowledge, this is the first report which has large number of PGL and longtime follow-up and shows the high risk of GA after treatment of PGL, especially in DLBCL.
Regarding the nature of GA after PGL, cancerous infiltration was only up to mucosal layer in 8 patients. This early detection was due to the short intervals between endoscopic examinations for PGL follow-ups. However, 4 of 10 patients had signet-ring cell carcinomas that had a more aggressive behavior than differentiated adenocarcinoma. Additionally, 2 patients with submucal and serosal infiltrations succumbed to distant metastasis after gastrectomy with 2 year and 5 year overall survival of 90.0% and 75.0%, respectively. GA after PGL may have more malignant potential than sporadic GA.
Conclusion
There were 10 patients of metachronous GA after PGL and the risk of metachronous GA after PGDLBCL was 10/83(=12.0%). GA after PGL may have more malignant potential than sporadic GA. Eradication of HP infection should be considered in PGL to reduce the risk of GA.
References
Kasahara Y, Takemoto M, Morishita A, Kuyama T, Takahashi M, Tanji K: Coexisting adenocarcinoma and malignant lymphoma of the stomach: case report and review of the Japanese literature. Am J Gastroenterol. 1988, 83: 190-193.
Noda T, Akashi H, Matsueda S, Katsuki N, Shirahashi K, Kojiro M: Collision of malignant lymphoma and multiple early adenocarcinomas of the stomach. Arch Pathol Lab Med. 1989, 113: 419-422.
Nakamura S, Aoyagi K, Iwanaga S, Yao T, Tsuneyoshi M, Fujishima M: Synchronous and metachronous primary gastric lymphoma and adenocarcinoma: a clinicopathological study of 12 patients. Cancer. 1997, 79: 1077-1085. 10.1002/(SICI)1097-0142(19970315)79:6<1077::AID-CNCR4>3.0.CO;2-D.
Akosa AB, Clark DM, Desa L: Synchronous adenocarcinoma and primary malignant lymphoma of the stomach. Postgrad Med J. 1990, 66: 778-780. 10.1136/pgmj.66.779.778.
Wotherspoon AC, Isaacson PG: Synchronous adenocarcinoma and low grade B-cell lymphoma of mucosa associated lymphoid tissue (MALT) of the stomach. Histopathology. 1995, 27: 325-331. 10.1111/j.1365-2559.1995.tb01522.x.
Nishino N, Konno H, Baba S, Aoki K, Nishimura T, Arai T, Kino I: Synchronous lymphoma and adenocarcinoma occurring as a collision tumor in the stomach: report of a case. Surg Today. 1996, 26: 508-512. 10.1007/BF00311557.
Hardman WJ, Gal AA, Pascal RR: Gastric adenocarcinoma and low-grade B-cell lymphoma of mucosa-associated lymphoid tissue. South Med J. 1997, 90: 426-430. 10.1097/00007611-199704000-00014.
Ishihama T, Kondo H, Saito D, Yamaguchi H, Shirao K, Yokota T, Hosokawa K, Ono H, Iwabuchi M, Gotoda T, Matsuno Y, Boku N, Ohtsu A, Yoshida S: Clinicopathological studies on coexisting gastric malignant lymphoma and gastric adenocarcinoma: report of four cases and review of the Japanese literature. Jpn J Clin Oncol. 1997, 27: 101-106. 10.1093/jjco/27.2.101.
Kaffes A, Hughes L, Hollinshead J, Katelaris P: Synchronous primary adenocarcinoma, mucosa-associated lymphoid tissue lymphoma and a stromal tumor in a Helicobacter pylori-infected stomach. J Gastroenterol Hepatol. 2002, 17: 1033-1036. 10.1046/j.1440-1746.2002.02649.x.
Sakai T, Ogura Y, Narita J, Suto T, Kimura D, Ainai S, Fujita H, Kamada M: Simultaneous early adenocarcinoma and mucosa-associated lymphoid tissue (MALT) lymphoma of the stomach associated with Helicobacter pylori infection. Gastric Cancer. 2003, 6: 191-196. 10.1007/s10120-003-0241-8.
Suenaga M, Ohta K, Toguchi M, Sato T, Ohyama S, Yamaguchi T, Muto T, Yanagisawa A, Kato Y: Colliding gastric and intestinal phenotype well-differentiated adenocarcinoma of the stomach developing in an area of MALT-type lymphoma. Gastric Cancer. 2003, 6: 270-276. 10.1007/s10120-003-0260-5.
Sellin J, Levin B, Reckard C, Riddell R: Gastric adenocarcinoma following gastric lymphoma. Role of partial gastrectomy. Cancer. 1980, 45: 996-1000. 10.1002/1097-0142(19800301)45:5<996::AID-CNCR2820450527>3.0.CO;2-W.
Brumback RA, Gerber JE, Hicks DG, Strauchen JA: Adenocarcinoma of the stomach following irradiation and chemotherapy for lymphoma in young patients. Cancer. 1984, 54: 994-998. 10.1002/1097-0142(19840915)54:6<994::AID-CNCR2820540609>3.0.CO;2-F.
Zorlu AF, Atahan IL, Gedikoglu G, Ruacan S, Sayek I, Tekuzman G: Does gastric adenocarcinoma develop after the treatment of gastric lymphoma?. J Surg Oncol. 1993, 54: 126-131. 10.1002/jso.2930540214.
Zauber NP, Berman EL: Synchronous and metachronous primary gastric lymphoma and adenocarcinoma: a clinicopathologic study of 12 patients. Cancer. 1998, 82: 226-227. 10.1002/(SICI)1097-0142(19980101)82:1<226::AID-CNCR28>3.0.CO;2-3.
Capelle LG, de Vries AC, Looman CWN, Casparie MK, Boot H, Meijer GA, Kuipers EJ: Gastric MALT lymphoma: epidemiology and high adenocarcinoma risk in a nation-wide study. Eur J Cancer. 2008, 44: 2470-2476. 10.1016/j.ejca.2008.07.005.
Cancer incidence and incidence rates in Japan. Center for Cancer Control and Information Services, National Cancer Center, Japan, [http://ganjoho.jp/pro/statistics/en/table_download.html]
Ruskone-Fourmestraux A, Fischbach W, Aleman BM, Boot H, Du MQ, Megraud F, Montalban C, Raderer M, Savio A, Wotherspoon A: EGILS consensus report. Gastric extranodal marginal zone B-cell lymphoma of MALT. Gut. 2011, 60: 747-758. 10.1136/gut.2010.224949.
Hamaloglu E, Topaloglu S, Ozdemir A, Ozenc A: Synchronous and metachronous occurrence of gastric adenocarcinoma and gastric lymphoma: a review of the literature. World J Gastroenterol. 2006, 12: 3564-3574.
Kellum JM, Jaffe BM, Calhoun TR, Ballinger WF: Gastric complications after radiotherapy for Hodgkin’s disease and other lymphomas. Am J Surg. 1977, 134: 314-317. 10.1016/0002-9610(77)90395-6.
Brown WM, Doll R: Mortality from cancer and other causes after radiotherapy for ankylosing spondylitis. Br Med J. 1965, 2: 1327-1332. 10.1136/bmj.2.5474.1327.
Abe S, Oda I, Kinjyou Y, Suzuki H, Nonaka S, Yoshinaga S, Makazu M, Sou E, Yachida T, Yamada M, Nakamura Y, Taniguchi H, Sekine S, Kushima R: Case report of early gastric cancer which can be diagnosed easily after Helicobacter Pylori eradication (written in Japanese). Stomach and intestine. 2012, 47: 1695-1699.
Kato M, Ono S, Takahashi M, Shinada K, Haneda M, Yamamoto K, Yoshida T, Mabe K, Shimizu Y, Asaka M, Mori Y, Nakagawa M, Nakagawa S: Multiple gastric carcinoma after Helicobacter pylori eradication (written in Japanese). Stomach and intestine. 2011, 46: 75-82.
Haruma K, Suzuki T, Tsuda T, Yoshihara M, Sumii K, Kajiyama G: Evaluation of tumor growth rate in patients with early gastric carcinoma of the elevated type. Gastrointest Radiol. 1991, 16: 289-292. 10.1007/BF01887370.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2407/13/499/prepub
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
KI, YK, MM, HM, YI, MS, TU and JI have made substantial contributions to conception and design. KI, TU and JI have been involved in drafting the manuscript or revising it critically for important intellectual content. RK carried out the pathologic examination. KI, NM, KH, MK, KY, SS and KT participated in acquisition of data and interpretation of data. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an open access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Inaba, K., Kushima, R., Murakami, N. et al. Increased risk of gastric adenocarcinoma after treatment of primary gastric diffuse large B-cell lymphoma. BMC Cancer 13, 499 (2013). https://doi.org/10.1186/1471-2407-13-499
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2407-13-499