
Abstract
Background
Rare, heterozygous germline mutations in the RAD51C gene have been found in breast and ovarian cancer families. In the Finnish population, we have identified two founder mutations in RAD51C that increase the risk of ovarian cancer but not breast cancer in the absence of ovarian cancer. Risk for other cancers has not been studied.
Methods
To study the role of RAD51C mutations in other common cancer types, we genotyped the Finnish RAD51C founder mutations c.837 + 1G > A and c.93delG in 1083 prostate cancer patients and 802 colorectal cancer patients using TaqMan Real-Time PCR.
Results
No RAD51C mutations c.837 + 1G > A or c.93delG were detected among the prostate or colorectal cancer patients.
Conclusions
The results suggest that the RAD51C mutations do not predispose to prostate or colorectal cancer.
Similar content being viewed by others


Background
Mutations in cancer susceptibility genes may predispose the carriers to different cancer types. The most important high penetrance breast and ovarian cancer susceptibility genes are BRCA1 and BRCA2[1] but, in addition to breast and ovarian cancer, germline mutations in these genes also increase the risk of prostate cancer [2, 3] and in BRCA2 also of pancreatic cancer [4]. In addition to the hereditary breast and ovarian cancer syndrome caused by germline mutations in BRCA1 and BRCA2, ovarian cancer is also present in the Lynch syndrome that is caused by germline mutations in DNA mismatch repair genes and characterized by susceptibility to colorectal cancer [5]. Increased risk of breast cancer is also present in other rare cancer predisposition syndromes, namely Li-Fraumeni, Cowden and Peutz-Jeghers syndrome and ataxia-telangiectasia, which also predispose to other cancer types as well [1].
Biallelic mutations in BRCA2 and in moderate penetrance breast cancer susceptibility genes PALB2 and BRIP1 cause Fanconi anemia, a chromosomal instability disorder characterized by developmental abnormalities, bone marrow failure, and cancer susceptibility, while heterozygous germline mutations increase the risk of breast cancer [6]. In addition to breast cancer, heterozygous mutations in PALB2 also increase the risk of pancreatic cancer [4] but not prostate cancer [7, 8]. In RAD51C, heterozygous germline mutations have been identified in breast and ovarian cancer families [9] and a homozygous missense mutation was found in a Fanconi anemia like disorder [10]. Following the original report, we and others have found rare deleterious mutations among breast and/or ovarian cancer families [11–17] but quite a few studies have not identified any clearly pathogenic mutations [18–24]. Indeed, the RAD51C mutations seem to be very rare. The association with ovarian cancer is well-established but whether the mutations also confer a risk for breast cancer remains controversial. Meindl et al. [9, 25] and Osorio et al. [16] state that RAD51C mutations predispose to breast and ovarian cancer whereas Loveday et al. [17] estimated the relative risk of ovarian cancer for RAD51C protein truncating mutation carriers to be 5.88 but no elevated risk for breast cancer.
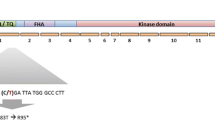
We recently sequenced the RAD51C gene in 277 Finnish breast and/or ovarian cancer families and identified two recurrent deleterious, protein truncating mutations c.837 + 1G > A and c.93delG and subsequently genotyped the mutations in a large series of breast and ovarian cancer patients and families [12]. The mutations significantly increased the risk of ovarian cancer but not breast cancer in the absence of ovarian cancer family history, indicating RAD51C as the first moderate penetrance susceptibility gene for ovarian cancer. The mutation carrier families shared a common haplotype indicating a founder effect for the mutations. Moreover, many of the mutation carriers had family history of various cancer types, including for instance colon and prostate cancer. Here we have genotyped the RAD51C mutations c.837 + 1G > A and c.93delG in 1083 prostate and 802 colorectal cancer patients to assess the risk for these cancer types. To our knowledge, the role of RAD51C mutations in other cancer types than breast and ovarian cancer has not been studied so far.
Methods
Subjects
The RAD51C mutations c.837 + 1G > A and c.93delG were genotyped in 1083 Finnish prostate cancer cases and 802 colorectal cancer cases. The prostate cancer patients included 894 unselected cases and 189 prostate cancer families. The unselected cases were collected from the Pirkanmaa Hospital District. The patients had been diagnosed with prostate cancer at the urology out-patient clinic at the Tampere University Hospital between years 1980 and 2008. All families included two or more affected members (the youngest affected male from each family was included in the analysis) and were collected as previously described [26]. The samples were genomic DNA isolated from peripheral blood with the Puregene kit, according to the manufacturer’s instructions (Gentra Systems, Inc., Minneapolis, MN, USA).
The colorectal cancer patients studied included 509 consecutive patients collected between May 1994 and April 1996 and 535 consecutive patients collected between March 1996 and June 1998 at nine large regional hospitals in southeastern Finland as described previously [27, 28]. DNA was isolated from normal mucosa or blood by conventional DNA extraction methods. DNA was available from 802 patients. All the samples were screened for microsatellite instability (MSI) and the MSI positive cases were screened for MLH1 and MSH2 mutations. Of the 802 patients, 104 had family background of colorectal cancer and MLH1 and MSH2 mutations were identified in 19 cases.
This study was carried out according to the Helsinki declaration with informed consents from the patients and with permissions from Institutional Review Board of the Tampere University Hospital, The Ministry of Health and Social Affairs, National Authority for Medical Affairs, National Institute for Health and Welfare and Helsinki University Hospital Ethics Committee.
Genotyping
We used TaqMan Custom Assays and TaqMan Genotyping MasterMix (Applied Biosystems, Foster City, CA, USA) to genotype the c.837 + 1G > A and c.93delG mutations. PCR was performed in 7500 Fast Real-Time PCR System or in 9800 Fast Thermal Cycler and genotype calling was performed with 7500 Fast Real-Time PCR System and ABI Prism 7500 SDS v1.4 software (Applied Biosystems, Foster City, CA, USA).
Results and discussion
Most moderate penetrance mutations identified so far, including mutations in RAD51C, appear to be very rare with mostly unique mutations in out-bread populations. This poses considerable challenges for investigating them in large series of patients with different cancer types to determine association also with other cancers. We took here advantage of the RAD51C founder mutations in Finland and genotyped the c.837 + 1G > A and c.93delG mutations in 1083 prostate and 802 colorectal cancer patients, including also familial cases. No mutations were detected among the patients.
We previously detected the RAD51C c.837 + 1G > A or c.93delG mutations in 1.4% of Finnish ovarian cancer patients (in 1% of unselected ovarian cancer patients and in 25% of ovarian cancer families) compared to 0.2% in controls, indicating a significantly increased risk of ovarian cancer with also clinical implications for the carriers [12]. Moreover, the mutation carrier families were found to share a common haplotype indicating a shared ancestry for the families and a founder effect for the mutations in the Finnish population. Founder mutations are typical for isolated populations, such as the Finnish population, and they may explain a major fraction of all mutations in specific genes [29, 30]. In the Finnish population, strong founder mutations have been detected for instance in the breast cancer susceptibility genes BRCA1 and BRCA2[31] as well as in PALB2[32].
Some of the RAD51C mutation carriers in our previous study [12] had family history of diverse cancer types (abdomen, brain, bone marrow, cervical, colon, female genital, kidney, leukemia, liver, lung, melanoma, pancreas, prostate, skin, stomach, tongue, and ventricle) but unfortunately we did not have available samples for genotyping of these relatives. Few other studies have also identified RAD51C mutation carrier families with diverse cancer types [9, 11, 13, 15–17]. This prompted us to study the effect of the mutations also on other common cancer types besides breast and ovarian cancer by screening of the founder mutations in an extensive series of prostate and colorectal cancer cases.
There is a clear genetic component in prostate cancer susceptibility and several common low-risk genomic loci for prostate cancer susceptibility have been found but no high-penetrance genes have been identified [33, 34]. Linkage studies have suggested that a prostate cancer susceptibility gene may be located on chromosome 17q22 [35, 36], a region including also the RAD51C locus, whereas genome-wide association studies (GWAS) have identified common low risk variants in 17q12 and 17q24 regions [37, 38]. Finnish as well as other Northern European patients have been included both in the linkage and in the GWA studies [35, 36, 38]. Several low-risk loci have also been identified for colorectal cancer but 17q22 has not been implicated in colorectal cancer susceptibility [39]. It has been estimated that 15–30% of colorectal cancer may be hereditary and approximately one-quarter of the familial cases occur as part of inherited colorectal tumor syndromes, mainly the Lynch syndrome caused by mutations in DNA mismatch repair genes, such as MSH2 and MLH1, and the familial adenomatous polyposis syndrome caused by mutations in the APC gene [40]. The absence of the RAD51C founder mutations among the prostate and colorectal cancer patients genotyped here suggests that RAD51C does not contribute to prostate or colorectal cancer predisposition. However, we cannot fully exclude a possible role of RAD51C as there might be mutation specific effects on cancer risk. To fully assess the role of RAD51C in susceptibility to other cancer types, screening of the whole coding region of the gene in large sample sets would be needed.
Conclusions
In conclusion, we did not detect the Finnish founder mutations in the RAD51C gene among 1083 prostate and 802 colorectal cancer patients suggesting that the RAD51C mutations do not predispose to prostate or colorectal cancer. These results have clinical value in assessing the cancer risks associated with RAD51C mutations in the mutation carrier families.
References
Stratton MR, Rahman N: The emerging landscape of breast cancer susceptibility. Nat Genet. 2008, 40: 17-22. 10.1038/ng.2007.53.
Leongamornlert D, Mahmud N, Tymrakiewicz M, Saunders E, Dadaev T, Castro E, Goh C, Govindasami K, Guy M, O’Brien L, Sawyer E, Hall A, Wilkinson R, Easton D, Goldgar D, Eeles R, Kote-Jarai Z, The UKGPCS Collaborators: Germline BRCA1 mutations increase prostate cancer risk. Br J Cancer. 2012, 106: 1697-1701. 10.1038/bjc.2012.146.
Kote-Jarai Z, Leongamornlert D, Saunders E, Tymrakiewicz M, Castro E, Mahmud N, Guy M, Edwards S, O’Brien L, Sawyer E, Hall A, Wilkinson R, Dadaev T, Goh C, Easton D, Goldgar D, Eeles R, UKGPCS Collaborators: BRCA2 is a moderate penetrance gene contributing to young-onset prostate cancer: implications for genetic testing in prostate cancer patients. Br J Cancer. 2011, 105: 1230-1234. 10.1038/bjc.2011.383.
Klein AP: Genetic susceptibility to pancreatic cancer. Mol Carcinog. 2012, 51: 14-24. 10.1002/mc.20855.
Lynch HT, Casey MJ, Snyder CL, Bewtra C, Lynch JF, Butts M, Godwin AK: Hereditary ovarian carcinoma: heterogeneity, molecular genetics, pathology, and management. Mol Oncol. 2009, 3: 97-137. 10.1016/j.molonc.2009.02.004.
D’Andrea AD: Susceptibility pathways in Fanconi’sanemia and breast cancer. N Engl J Med. 2010, 362: 1909-1919. 10.1056/NEJMra0809889.
Tischkowitz M, Sabbaghian N, Ray AM, Lange EM, Foulkes WD, Cooney KA: Analysis of the gene coding for the BRCA2-interacting protein PALB2 in hereditary prostate cancer. Prostate. 2008, 68: 675-678. 10.1002/pros.20729.
Pakkanen S, Wahlfors T, Siltanen S, Patrikainen M, Matikainen MP, Tammela TL, Schleutker J: PALB2 Variants in hereditary and unselected Finnish prostate cancer cases. J Negat Results Biomed. 2009, 8: 12-10.1186/1477-5751-8-12.
Meindl A, Hellebrand H, Wiek C, Erven V, Wappenschmidt B, Niederacher D, Freund M, Lichtner P, Hartmann L, Schaal H, Ramser J, Honisch E, Kubisch C, Wichmann HE, Kast K, Deissler H, Engel C, Muller-Myhsok B, Neveling K, Kiechle M, Mathew CG, Schindler D, Schmutzler RK, Hanenberg H: Germline mutations in breast and ovarian cancer pedigrees establish RAD51C as a human cancer susceptibility gene. Nat Genet. 2010, 42: 410-414. 10.1038/ng.569.
Vaz F, Hanenberg H, Schuster B, Barker K, Wiek C, Erven V, Neveling K, Endt D, Kesterton I, Autore F, Fraternali F, Freund M, Hartmann L, Grimwade D, Roberts RG, Schaal H, Mohammed S, Rahman N, Schindler D, Mathew CG: Mutation of the RAD51C gene in a fanconianemia-like disorder. Nat Genet. 2010, 42: 406-409. 10.1038/ng.570.
Romero A, Perez-Segura P, Tosar A, Garcia-Saenz JA, Diaz-Rubio E, Caldes T, de la Hoya M: A HRM-based screening method detects RAD51C germ-line deleterious mutations in Spanish breast and ovarian cancer families. Breast Cancer Res Treat. 2011, 129: 939-946. 10.1007/s10549-011-1543-x.
Pelttari LM, Heikkinen T, Thompson D, Kallioniemi A, Schleutker J, Holli K, Blomqvist C, Aittomaki K, Butzow R, Nevanlinna H: RAD51C is a susceptibility gene for ovarian cancer. Hum Mol Genet. 2011, 20: 3278-3288. 10.1093/hmg/ddr229.
Vuorela M, Pylkas K, Hartikainen JM, Sundfeldt K, Lindblom A, von WachenfeldtWappling A, Haanpaa M, Puistola U, Rosengren A, Anttila M, Kosma VM, Mannermaa A, Winqvist R: Further evidence for the contribution of the RAD51C gene in hereditary breast and ovarian cancer susceptibility. Breast Cancer Res Treat. 2011, 130: 1003-1010. 10.1007/s10549-011-1677-x.
Walsh T, Casadei S, Lee MK, Pennil CC, Nord AS, Thornton AM, Roeb W, Agnew KJ, Stray SM, Wickramanayake A, Norquist B, Pennington KP, Garcia RL, King MC, Swisher EM: Mutations in 12 genes for inherited ovarian, fallopian tube, and peritoneal carcinoma identified by massively parallel sequencing. Proc Natl Acad Sci U S A. 2011, 108: 18032-18037. 10.1073/pnas.1115052108.
Thompson ER, Boyle SE, Johnson J, Ryland GL, Sawyer S, Choong DY, Chenevix-Trench G, Trainer AH, Lindeman GJ, Mitchell G, James PA, Campbell IG, kConFab: Analysis of RAD51C germline mutations in high-risk breast and ovarian cancer families and ovarian cancer patients. Hum Mutat. 2012, 33: 95-99. 10.1002/humu.21625.
Osorio A, Endt D, Fernandez F, Eirich K, Hoya MD, Schmutzler R, Caldes T, Meindl A, Schindler D, Benitez J: Predominance of pathogenic missense variants in the RAD51C gene occurring in breast and ovarian cancer families. Hum Mol Genet. 2012, 21: 2889-2898. 10.1093/hmg/dds115.
Loveday C, Turnbull C, Ruark E, Xicola RM, Ramsay E, Hughes D, Warren-Perry M, Snape K, Eccles D, Evans DG, Gore M, Renwick A, Seal S, Antoniou AC, Rahman N, Breast Cancer Susceptibility Collaboration (BCSC) (UK): Germline RAD51C mutations confer susceptibility to ovarian cancer. Nat Genet. 2012, 44: 475-476. 10.1038/ng.2224.
Zheng Y, Zhang J, Hope K, Niu Q, Huo D, Olopade OI: Screening RAD51C nucleotide alterations in patients with a family history of breast and ovarian cancer. Breast Cancer Res Treat. 2010, 124: 857-861. 10.1007/s10549-010-1095-5.
Akbari MR, Tonin P, Foulkes WD, Ghadirian P, Tischkowitz M, Narod SA: RAD51C germline mutations in breast and ovarian cancer patients. Breast Cancer Res. 2010, 12: 404-10.1186/bcr2619.
Wong MW, Nordfors C, Mossman D, Pecenpetelovska G, Avery-Kiejda KA, Talseth-Palmer B, Bowden NA, Scott RJ: BRIP1, PALB2, and RAD51C mutation analysis reveals their relative importance as genetic susceptibility factors for breast cancer. Breast Cancer Res Treat. 2011, 127: 853-859. 10.1007/s10549-011-1443-0.
Pang Z, Yao L, Zhang J, Ouyang T, Li J, Wang T, Fan Z, Fan T, Lin B, Xie Y: RAD51C germline mutations in Chinese women with familial breast cancer. Breast Cancer Res Treat. 2011, 129: 1019-1020. 10.1007/s10549-011-1574-3.
Clague J, Wilhoite G, Adamson A, Bailis A, Weitzel JN, Neuhausen SL: RAD51C germline mutations in breast and ovarian cancer cases from high-risk families. PLoS One. 2011, 6 (9): e25632-10.1371/journal.pone.0025632.
De Leeneer K, Van Bockstal M, De Brouwer S, Swietek N, Schietecatte P, Sabbaghian N, Van den Ende J, Willocx S, Storm K, Blaumeiser B, Van Asperen CJ, Wijnen JT, Leunen K, Legius E, Michils G, Matthijs G, Blok MJ, Gomez-Garcia E, De Paepe A, Tischkowitz M, Poppe B, Claes K: Evaluation of RAD51C as cancer susceptibility gene in a large breast-ovarian cancer patient population referred for genetic testing. Breast Cancer Res Treat. 2012, 133: 393-398. 10.1007/s10549-012-1998-4.
Lu W, Wang X, Lin H, Lindor NM, Couch FJ: Mutation screening of RAD51C in high-risk breast and ovarian cancer families. Fam Cancer. 2012, 11: 381-385. 10.1007/s10689-012-9523-9.
Meindl A, Eirich K, Engert S, Becker A, Endt D, Ditsch N, Schmutzler RK, Schindler D: Germline RAD51C mutations confer susceptibility to ovarian cancer. Nat Genet. 2012, 44: 476-10.1038/ng.2223.
Matikainen MP, Sankila R, Schleutker J, Kallioniemi OP, Pukkala E: Nationwide cancer family ascertainment using Finnish cancer registry data on family names and places of birth for 35,761 prostate cancer patients. Int J Cancer. 2000, 88: 307-312. 10.1002/1097-0215(20001015)88:2<307::AID-IJC25>3.0.CO;2-7.
Aaltonen LA, Salovaara R, Kristo P, Canzian F, Hemminki A, Peltomaki P, Chadwick RB, Kaariainen H, Eskelinen M, Jarvinen H, Mecklin JP, de la Chapelle A: Incidence of hereditary nonpolyposis colorectal cancer and the feasibility of molecular screening for the disease. N Engl J Med. 1998, 338: 1481-1487. 10.1056/NEJM199805213382101.
Salovaara R, Loukola A, Kristo P, Kaariainen H, Ahtola H, Eskelinen M, Harkonen N, Julkunen R, Kangas E, Ojala S, Tulikoura J, Valkamo E, Jarvinen H, Mecklin JP, Aaltonen LA, de la Chapelle A: Population-based molecular detection of hereditary nonpolyposis colorectal cancer. J ClinOncol. 2000, 18: 2193-2200.
Arcos-Burgos M, Muenke M: Genetics of population isolates. Clin Genet. 2002, 61: 233-247. 10.1034/j.1399-0004.2002.610401.x.
Peltonen L, Jalanko A, Varilo T: Molecular genetics of the Finnish disease heritage. Hum Mol Genet. 1999, 8: 1913-1923. 10.1093/hmg/8.10.1913.
Sarantaus L, Huusko P, Eerola H, Launonen V, Vehmanen P, Rapakko K, Gillanders E, Syrjakoski K, Kainu T, Vahteristo P, Krahe R, Paakkonen K, Hartikainen J, Blomqvist C, Lopponen T, Holli K, Ryynanen M, Butzow R, Borg A, WastesonArver B, Holmberg E, Mannermaa A, Kere J, Kallioniemi OP, Winqvist R, Nevanlinna H: Multiple founder effects and geographical clustering of BRCA1 and BRCA2 families in Finland. Eur J Hum Genet. 2000, 8: 757-763. 10.1038/sj.ejhg.5200529.
Erkko H, Xia B, Nikkila J, Schleutker J, Syrjakoski K, Mannermaa A, Kallioniemi A, Pylkas K, Karppinen SM, Rapakko K, Miron A, Sheng Q, Li G, Mattila H, Bell DW, Haber DA, Grip M, Reiman M, Jukkola-Vuorinen A, Mustonen A, Kere J, Aaltonen LA, Kosma VM, Kataja V, Soini Y, Drapkin RI, Livingston DM, Winqvist R: A recurrent mutation in PALB2 in Finnish cancer families. Nature. 2007, 446: 316-319. 10.1038/nature05609.
Schaid DJ: The complex genetic epidemiology of prostate cancer. Hum Mol Genet. 2004, 13 (Suppl 1): R103-R121.
Kim ST, Cheng Y, Hsu FC, Jin T, Kader AK, Zheng SL, Isaacs WB, Xu J, Sun J: Prostate cancer risk-associated variants reported from genome-wide association studies: meta-analysis and their contribution to genetic variation. Prostate. 2010, 70: 1729-1738.
Gillanders EM, Xu J, Chang BL, Lange EM, Wiklund F, Bailey-Wilson JE, Baffoe-Bonnie A, Jones M, Gildea D, Riedesel E, Albertus J, Isaacs SD, Wiley KE, Mohai CE, Matikainen MP, Tammela TL, Zheng SL, Brown WM, Rokman A, Carpten JD, Meyers DA, Walsh PC, Schleutker J, Gronberg H, Cooney KA, Isaacs WB, Trent JM: Combined genome-wide scan for prostate cancer susceptibility genes. J Natl Cancer Inst. 2004, 96: 1240-1247. 10.1093/jnci/djh228.
Cropp CD, Simpson CL, Wahlfors T, Ha N, George A, Jones MS, Harper U, Ponciano-Jackson D, Green TA, Tammela TL, Bailey-Wilson J, Schleutker J: Genome-wide linkage scan for prostate cancer susceptibility in Finland: evidence for a novel locus on 2q37.3 and confirmation of signal on 17q21-q22. Int J Cancer. 2011, 129 (10): 2400-2407. 10.1002/ijc.25906.
Gudmundsson J, Sulem P, Steinthorsdottir V, Bergthorsson JT, Thorleifsson G, Manolescu A, Rafnar T, Gudbjartsson D, Agnarsson BA, Baker A, Sigurdsson A, Benediktsdottir KR, Jakobsdottir M, Blondal T, Stacey SN, Helgason A, Gunnarsdottir S, Olafsdottir A, Kristinsson KT, Birgisdottir B, Ghosh S, Thorlacius S, Magnusdottir D, Stefansdottir G, Kristjansson K, Bagger Y, Wilensky RL, Reilly MP, Morris AD, Kimber CH, et al: Two variants on chromosome 17 confer prostate cancer risk, and the one in TCF2 protects against type 2 diabetes. Nat Genet. 2007, 39: 977-983. 10.1038/ng2062.
Jin G, Lu L, Cooney KA, Ray AM, Zuhlke KA, Lange EM, Cannon-Albright LA, Camp NJ, Teerlink CC, Fitzgerald LM, Stanford JL, Wiley KE, Isaacs SD, Walsh PC, Foulkes WD, Giles GG, Hopper JL, Severi G, Eeles R, Easton D, Kote-Jarai Z, Guy M, Rinckleb A, Maier C, Vogel W, Cancel-Tassin G, Egrot C, Cussenot O, Thibodeau SN, McDonnell SK, et al: Validation of prostate cancer risk-related loci identified from genome-wide association studies using family-based association analysis: evidence from the international consortium for prostate cancer genetics (ICPCG). Hum Genet. 2012, 131: 1095-1103. 10.1007/s00439-011-1136-0.
Varghese JS, Easton DF: Genome-wide association studies in common cancers–what have we learnt?. Curr Opin Genet Dev. 2010, 20 (3): 201-209. 10.1016/j.gde.2010.03.012.
Fearon ER: Molecular genetics of colorectal cancer. Annu Rev Pathol. 2011, 6: 479-507. 10.1146/annurev-pathol-011110-130235.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2407/12/552/prepub
Acknowledgements
This study has been supported by the Helsinki University Central Hospital Research Fund, the Academy of Finland (132473), the Sigrid Juselius Foundation and the Finnish Cancer Society.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
LMP and HN designed the study and wrote the manuscript. LMP and RN carried out the genotyping. JS, AG and LA contributed samples and patient information. All authors read and approved the final manuscript.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Pelttari, L.M., Nurminen, R., Gylfe, A. et al. Screening of Finnish RAD51Cfounder mutations in prostate and colorectal cancer patients. BMC Cancer 12, 552 (2012). https://doi.org/10.1186/1471-2407-12-552
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2407-12-552