
Abstract
Background
Breastfeeding behaviour is multifactorial, and a wide range of socio-cultural and physiological variables impact on a woman's decision and ability to breastfeed successfully. An association has been reported between maternal obesity and low breastfeeding rates. This is of public health concern because obesity is rising in women of reproductive age and the apparent association with increased artificial feeding will lead to a greater risk of obesity in children. The aim of this paper is to examine the relationship between maternal overweight and obesity and breastfeeding intention and initiation and duration.
Methods
A systematic review was conducted in January and February 2007, using the following databases: Medline, CINAHL and the Australian Breastfeeding Association's Lactation Resource Centre. Studies which have examined maternal obesity and infant feeding intention, initiation, duration and delayed onset of lactation were tabulated and summarised.
Results
Studies have found that obese women plan to breastfeed for a shorter period than normal weight women and are less likely to initiate breastfeeding. Of the four studies that examined onset of lactation, three reported a significant relationship between obesity and delayed lactogenesis. Fifteen studies, conducted in the USA, Australia, Denmark, Kuwait and Russia, have examined maternal obesity and duration of breastfeeding. The majority of large studies found that obese women breastfed for a shorter duration than normal weight women, even after adjusting for possible confounding factors.
Conclusion
There is evidence from epidemiological studies that overweight and obese women are less likely to breastfeed than normal weight women. The reasons may be biological or they may be psychological, behavioral and/or cultural. We urgently need qualitative studies from women's perspective to help us understand women in this situation and their infant feeding decisions and behaviour.
Similar content being viewed by others


Background
Infants not breastfed have increased risks of ill-health – both short- (e.g. gastrointestinal infections [1]) and long-term (such as diabetes [2]). Recent systematic reviews have shown a dose-dependent association between longer duration of breastfeeding and decrease in the risk of overweight in later life [3, 4]. Looking at the population impact, it has been estimated that 13,639 cases of obesity (95%CI 7,838, 19,308) could be prevented in England and Wales over 9 years if all infants were breastfed for at least three months [5].
Obesity is an increasing problem globally: populations in poor countries as well as affluent ones are at risk [6]. Reports of obesity among pregnant women in the USA range from 18.5% to 38.3%, making it one of the most frequent high-risk obstetric situations [7]. A recent Australian study reported that 34% of pregnant women were overweight or obese; overweight/obese women had increased adverse maternal and neonatal outcomes, resulting in increased costs of obstetric care [8]. The increase in maternal obesity is accelerating, and is associated with socio-economic disadvantage [9]. It has been recognised that obesity may track across generations, thus prevention is an urgent priority [10].
In 1992, Rutishauser & Carlin reported a negative relationship between maternal obesity and breastfeeding duration and they stated that this was the first study to investigate the effect of over- rather than under-nutrition on the duration of breastfeeding [11]. Since then, a number of studies have found lower rates of breastfeeding in women who are overweight and obese compared to women of normal weight [12–14]. Some researchers have attributed this to physiological causes, such as delayed lactogenesis ("milk coming in") [15] and lower prolactin response [16]. However, as obese women are more likely to belong to subgroups of women with lower rates of breastfeeding than normal weight women, such as lower socioeconomic status [17] and higher depression [18], it is necessary to adjust for these potential confounding factors.
This is an important public health issue as the increasing incidence of maternal obesity and the apparent association with increased artificial feeding of infants will lead to an increasing risk of obesity in children. The aim of this paper is to examine the relationship between maternal overweight and obesity and breastfeeding intention and initiation and duration.
Methods
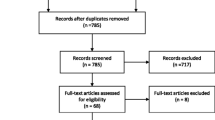
A systematic review was conducted in January and February 2007 using the key words "(obesity OR BMI) AND (breastf* OR lactation OR lactating)". The following databases were searched (all languages, from the start of the database):
-
Medline via PubMed (8 February 2007) 767 items, 24 were relevant;
-
CINAHL (Cumulative Index to Nursing & Allied Health Literature) (8 February 2007) 103 items, 11 relevant (1 additional);
-
Australian Breastfeeding Association's Lactation Resource Centre database was searched for 'obesity' (21 January 2007); 172 items, 10 relevant (3 additional).
Most of the articles found in the databases were about the relationship between breastfeeding and childhood obesity and were therefore not relevant to this review. All papers related to maternal overweight and obesity and infant feeding were located and included if appropriate. Papers that were case studies, clinical papers or reviews were not included in the tables [19–28]. Research studies were also identified from the reference lists of included articles, and the authors' literature collection was hand-searched (n = 2230; nine additional studies). Papers which had cited the original Rutishauser and Carlin study were identified (n = 6), but no new papers were revealed. The total number of research articles included in this review is 27.
Five papers were excluded as they did not define overweight or obesity (e.g. presented body mass index (BMI, kg/m2) as a continuous variable [29–32] or used vague terms, such as "heavy before becoming pregnant" [33]). However, as there were very few studies on women's infant feeding intention and maternal overweight and obesity, a study which examined women's "weight concerns" was included [34] as this information was also relevant. Thus, 22 papers are included in the tables (27 less 5).
Most studies based their evaluation of maternal obesity on the World Health Organization (WHO) definition of obesity [35]: normal weight BMI<25, overweight BMI 25 ≤ 30, obese BMI > 30, or the US Institute of Medicine (IOM) definition [36]: underweight/normal weight BMI < 26.1, overweight BMI 26.1 – 29.0, obese BMI > 29.0.
The papers have been grouped according to the content of the study and presented in tables alphabetically by the first author. As women's infant feeding intention has been found to be the strongest single predictor of breastfeeding behaviour [37], all studies reporting infant feeding intention and maternal obesity, including those with "vague" definitions, have been included in Table 1 (Included studies on maternal obesity and women's infant feeding intentions).
The indicators suggested for monitoring breastfeeding have been described as:
-
Initiation (the infant's first intake of breast milk)
-
Intensity (the degree of exclusiveness of breast milk as the source of nourishment for the infant) and
-
Total duration (the total length of time that an infant receives any breast milk at all [38].
Authorities recommend that breastfeeding initiation is defined as "ever breastfed/ever given breast milk" so that infants who only went to the breast once or only received expressed breast milk are included [38]. However, research studies have used a range of definitions, including breastfeeding at hospital discharge [12], breastfeeding at four days [39], feeding in last five feeds in hospital [40]. Table 2 (Included studies on maternal obesity and initiation of breastfeeding) includes the studies which have reported breastfeeding initiation (however defined), and the authors' definition when it varies from "ever breastfed". Where the authors have not presented an odds ratio (OR) for breastfeeding initiation we have calculated one using data from their publication (labelled as "our calculation of overweight/obese women not initiating breastfeeding"). These are unadjusted odds ratios as we did not have the data to adjust for potential confounding factors such as income or method of birth. We have not performed a meta-analysis as the definitions of initiation are inconsistent.
It has been hypothesised that the onset of lactation occurs later in obese women than other women, therefore all studies which have investigated this are listed in Table 3 (Included studies on maternal obesity and delayed onset of lactation).
The final table (Table 4. Included studies on maternal obesity and duration of breastfeeding) includes studies which report total duration of breastfeeding and, where reported, exclusive breastfeeding; multivariate analysis has been included when this has been conducted.
Results
There were three studies that examined pregnant women's body mass index [41, 42] or "weight concerns" [34] and their infant feeding intentions (Table 1. Included studies on maternal obesity and women's infant feeding intentions). In a large population-based study in the UK, women identified as having "marked concern" about body shape and weight on a questionnaire were significantly less likely to intend to breastfeed their infant up to four months after adjusting for a range of variables [34]. A small US study found that obese women planned to breastfeed for a shorter duration (6.9 months) than other women (9.3 to 9.8 months) [42].
Nine of the ten studies of breastfeeding initiation found that overweight and obese women were less likely to commence breastfeeding (Table 2. Included studies on maternal obesity and initiation of breastfeeding). The exception was one study in Russia where virtually all women initiated breastfeeding [43]; the other studies were conducted in the USA (n = 5), Australia (n = 3) and the UK (n = 1). The difference was statistically significant in most studies, but not for black women in the US in the study by Kugyelka [40], nor for women in two studies in Western Australia [44, 45]. The estimated size of the effect (OR of not commencing compared with normal weight women) ranged from 1.19 to 2.17 for overweight women and from 1.38 to 3.09 for obese women in these studies (see Table 2).
Table 3 shows the five studies which have examined the relationship between obesity and a delayed onset of lactogenesis (the arrival of a copious milk supply). All studies were conducted in the USA and the sample size ranged from 40 to 280. Delayed onset was found in three studies [15, 46, 47]. Overweight/obese women were more likely to have late arrival of milk (33%) than normal women (16%), with a relative risk of 2.46 on multivariate analysis [47]. Infants of overweight/obese women were more likely to have suboptimal feeding behaviour on multivariate analysis (RR 2.58) [47]. One study found that overweight/obese women fed their infants for longer (23 minutes) than normal weight women (15 minutes) and had a lower prolactin response to suckling at 48 hours, but not 7 days, compared to normal weight women [16]. One study didn't have enough power to detect a difference [42]. No study found a faster onset of lactation or improved infant feeding in overweight or obese women.
A medical record review in the US found that obese women were less likely to have put the baby to the breast within the first two hours than normal weight women [40].
The studies reporting on maternal obesity and duration of breastfeeding are presented in Table 4. There were fifteen studies, of which seven were conducted in the USA, five in Australia, and one each in Denmark, Kuwait and Russia. The majority of large studies found that obese women breastfed for a shorter duration than normal weight women, even after adjusting for possible confounding factors [11–13, 39, 44, 48, 49]. Studies in Russia [43] and Denmark [50] with high breastfeeding initiation rates found no difference in breastfeeding duration according to maternal obesity. A recent Australian study of 764 women found that obese women were less likely to be breastfeeding at six months than women with a normal BMI [48]. Obese women had an odds of 0.49 (95%CI 0.28, 0.85) for breastfeeding at six months compared to women with a normal BMI, adjusted for a range of factors including infant feeding intention, maternal age, smoking and depression [48]. In the USA, Kugyelka and colleagues found no effect of obesity in duration of breastfeeding in black women (while they did find a relationship in Hispanic women) [40]. Only one study, in Kuwait, found that higher maternal weight (120% of standard reference weight for height) was associated with longer duration of breastfeeding [51].
Discussion
Possible reasons why overweight/obese women are less likely to breastfeed
1. Anatomical/physiological
Several studies have investigated delayed lactogenesis II (the onset of a copious milk supply) in obese women (Table 3). They reported delayed lactogenesis according to maternal perception and to physiological markers. Obesity remained associated with delayed lactogenesis after adjusting for several possible confounding factors, but infant feeding intention was not included. As obese women intend to breastfeed for shorter durations than other women, perhaps part of the delay in time to first feed [40] and tendency to give up before hospital discharge is behavioural rather than physiological.
Adipose tissue acts as a reservoir for steroid hormones and is also a site of steroid production and metabolism [52, 53]. One theory for the delay in lactogenesis II is that progesterone stored in adipose tissue leads to higher progesterone levels in obese women than normal-weight women which disrupts the usual sudden drop in progesterone leading to lactogenesis II [54]. However the only study to investigate this found no difference in serum progesterone levels between obese/overweight women and normal weight women [16].
Although women with large breasts are not necessarily obese, obese women will often have large breasts, and there are indications in the literature that large breasts have been associated with breastfeeding difficulties. Historically it was thought that wet nurses with large breasts were poor milk producers [55]. "Overly large breasts usually betrayed a true poverty of milk, for the heavy fat parts impeded the separation of the milk and its free passage through the narrow conduits to the nipples" [[55], p52]. A study of perceived insufficient milk found that women with a high BMI were more likely to experience an earlier onset of "insufficient milk" (p < 0.05), but this was not significant in multivariate survival analysis [56]. In contrast, Rutishauser and Carlin found that overweight/obese women were less likely to give "poor milk supply" as the reason for early cessation of breastfeeding than women of normal weight (p < 0.05) [11].
Women with large breasts may have practical/mechanical difficulties with attaching the baby to the breast [57, 58]. It can be awkward to support a large breast while assisting a baby to latch on; sometimes the nipple/areola may not be visible to the mother. Some women with large breasts have broad areolae (rather than conical) with short nipples making it difficult to attach the baby [19]. Lactation consultants have noticed that the weight of a large, heavy breast on the infant's chest can interfere with successful attachment [21].
2. Medical conditions
Obese and overweight women are over-represented in gynaecological and reproductive medicine clinics [53]. They are more likely to have medical conditions such as polycystic ovary syndrome (PCOS) and diabetes, and to experience obstetric complications and caesarean birth than women of normal weight [28, 59]. Women with diabetes and those who give birth by Caesarean section may be more likely to experience delayed lactogenesis or low milk supply [60–62]. Some women with PCOS have insufficient milk supply, which is thought to be related to the endocrinological changes associated with the syndrome (high levels of androgens, insulin resistance, frequently low progesterone levels) [23].
Some studies have taken this into account by recruiting only women without medical conditions [30, 39] or using multivariate analysis to adjust for these factors [12]. Studies have found that women with early-onset obesity (eg prior to menarche) are more likely to have ovulatory disturbances than women with later-onset obesity [52]. Animal studies have also found that early-onset obesity may negatively affect adult function. Cows with high rates of growth before puberty have less mammary development (as measured by mammary DNA) [63, 64]. A meta-analysis of eight experimental studies of prepubertal weight gain in Holstein heifers, found that first-lactation production increased as weight gains increased up to 799 g/day, however higher weight gains were associated with lower milk production [65]. In humans, breastfeeding success (or duration) has not been studied in relation to the onset of obesity in the mother (i.e. in childhood before the development of the breasts) or in later life
3. Socio-cultural
Women who are obese are more likely to belong to social groups who are less likely to breastfeed, such as lower socio-economic status [66, 67] and less likely to have been breastfed themselves [31, 68]. As with women who smoke, obese women have lower intention to breastfeed [37, 69]. Obese women are less likely to participate in preventative health behaviours such having Pap smears and mammography [70]. This may relate to their health beliefs or to feelings of embarrassment with exposure of body parts; it is likely that overweight/obese women may feel more uncomfortable with the idea of breastfeeding in public. Furthermore, large breasts may make if difficult to breastfeed "discretely" and thus "modesty" may another reason for some women to avoid breastfeeding.
Yet in some cultures, maternal weight appears to have no relationship with infant feeding. Indigenous women in Canada have high levels of overweight and obesity and high levels of breastfeeding [71].
4. Psychological
Obese women tend to have greater body image dissatisfaction compared with non-obese women [72]. Women with increased concern about their body shape or weight are less likely to intend to breastfeed [34].
Obese women tend to have lower self-esteem [73] and poorer mental health than normal weight women [74]. Obese mothers are more likely to have postpartum depression [18]; depressed mothers are less likely to continue breastfeeding than non-depressed mothers [75]. A small study of obese formula-feeding mothers found that they spent less time interacting with infants over a 24 hour testing period than non-obese mothers [76].
What to do about it?
Clinicians need to be aware that obese women are at high risk of not breastfeeding, yet a recent study found clinicians did not manage obese women differently from normal weight women [26]. A new review of maternal obesity in pregnancy acknowledged "the increased risk of lactation failure and delay in establishing lactation postdelivery" [[77] p1137], yet did not mention infant feeding in their management guidelines. Obese women may experience a delay in the onset of lactation but in supportive environments breastfeeding can be successfully established.
Future physiological and epidemiological studies could focus on obese women with a strong intention to breastfeed and without medical or obstetric complications in order to compare breastfeeding success in these women with similar women with normal BMI. To date, no studies have examined this issue from the women's perspective. We urgently need qualitative studies to help us understand obese women and their infant feeding decisions and behaviour. Any potential interventions aimed at helping overweight and obese women to breastfeed successfully need to be evaluated in randomised controlled trials.
Conclusion
Breastfeeding behaviour is multifactorial, and a wide range of socio-cultural and physiological variables impact on a woman's decision and ability to breastfeed successfully. Breastfeeding rates vary from population group to group – the variation is usually due to social rather than biological factors. Our analysis of maternal smoking and breastfeeding found that maternal infant feeding intention was a more powerful predictor of breastfeeding duration than whether the mother smoked or not [78]. Smokers with a strong intention to breastfeed were more likely to continue breastfeeding that non-smokers with a low intention to breastfeed, i.e. the social factors were more important than the possible negative physiological effects of nicotine on breast milk supply [78].
Evidence suggests that lactational performance is not compromised by low BMI [79]; it is still unclear if obesity per se has a role in reduced lactation in overweight and obese women. There are many psychological, behavioral and cultural reasons that may be responsible for reduced lactation in obese women. It is clear that there is a relationship between obesity and variables associated with lower rates of breastfeeding: lower income, depression, body image concerns. Evidence such as obese women's lower intention [34, 41, 42] and a 10% greater chance of not putting the baby to the breast in the first two hours of life [40] will lead to physiological differences between obese women and normal weight women – but the differences may not be due to obesity per se.
However a number of epidemiological [11–13, 39, 44, 48, 49] and animal studies [80, 81] do suggest that maternal obesity is detrimental to lactation. One possibility is that the impact of obesity on lactation is related to the age of development of obesity, as prepubertal obesity is detrimental to lactation in dairy cows [65]. Further studies into the timing of obesity during women's reproductive lifetime may help to clarify this. In addition, qualitative studies as well as quantitative studies should be undertaken to explore the relationship between maternal obesity and breastfeeding.
References
Kramer MS, Chalmers B, Hodnett ED, Sevkovskaya Z, Dzikovich I, Shapiro S, et al, PROBIT Study Group (Promotion of Breastfeeding Intervention Trial): Promotion of Breastfeeding Intervention Trial (PROBIT): a randomized trial in the Republic of Belarus. JAMA. 2001, 285 (4): 413-420. 10.1001/jama.285.4.413.
Taylor JS, Kacmar JE, Nothnagle M, Lawrence RA: A systematic review of the literature associating breastfeeding with type 2 diabetes and gestational diabetes. J Am Coll Nutr. 2005, 24 (5): 320-326.
Harder T, Bergmann R, Kallischnigg G, Plagemann A: Duration of breastfeeding and risk of overweight: A meta-analysis. Am J Epidemiol. 2005, 162: 397-403. 10.1093/aje/kwi222.
Owen CG, Martin RM, Whincup PH, Davey Smith G, Cook DG: Effect of infant feeding on the risk of obesity across the life course: A quantitative review of published evidence. Pediatrics. 2005, 115 (5): 1367-1377. 10.1542/peds.2004-1176.
Akobeng AK, Heller RF: Assessing the population impact of low rates of breastfeeding on asthma, coeliac disease and obesity: the use of a new statistical method. Arch Dis Child. 2007, 92 (6): 483-485. 10.1136/adc.2006.097667.
World Health Organization: Obesity: preventing and managing the global epidemic: report of a WHO consultation. World Health Organ Tech Rep Ser. 2000, 894: i-253.
Galtier-Dereure F, Boegner C, Bringer J: Obesity and pregnancy: complications and cost. Am J Clin Nutr. 2000, 71(suppl): 1242S-48S.
Callaway LK, Prins JB, Chang AM, McIntyre HD: The prevalence and impact of overweight and obesity in an Australian population. Med J Aust. 2006, 184 (2): 56-59.
Heslehurst N, Ells LJ, Batterham A, Wilkinson J, Summerbell CD: Trends in maternal obesity incidence rates, demographic predictors, and health inequalities in 36 821 women over a 15-year period . BJOG. 2007, 114 (2): 187-194. 10.1111/j.1471-0528.2006.01180.x.
Johnson DB, Gerstein DE, Evans AE, Woodward-Lopez G: Preventing obesity: A life cycle perspective. J Am Diet Assoc. 2006, 106: 97-102. 10.1016/j.jada.2005.09.048.
Rutishauser IHE, Carlin JB: Body mass index and duration of breast feeding: a survival analysis during the first six months of life. J Epidemiol Community Health. 1992, 46: 559-565.
Hilson JA, Rasmussen KM, Kjolhede CL: Maternal obesity and breast-feeding success in a rural population of white women. Am J Clin Nutr. 1997, 66: 1371-1378.
Donath SM, Amir LH: Does maternal obesity adversely affect breastfeeding initiation and duration?. J Paediatr Child Health. 2000, 36: 482-486. 10.1046/j.1440-1754.2000.00562.x.
Sebire NJ, Jolly M, Harris JP, Wadsworth J, Joffe M, Beard RW, Regan L, Robinson S: Maternal obesity and pregnancy outcome: a study of 287,213 pregnancies in London. Int J Obes Relat Metab Disord. 2001, 25 (8): 1175-1182. 10.1038/sj.ijo.0801670.
Chapman DJ, Perez-Escamilla R: Identification of risk factors for delayed onset of lactation. J Am Diet Assoc. 1999, 99: 450-454. 10.1016/S0002-8223(99)00109-1.
Rasmussen KM, Kjolhede CL: Prepregnant overweight and obesity diminish the prolactin response to suckling in the first week postpartum. Pediatrics. 2004, 113: e465-e471. 10.1542/peds.113.5.e465.
Rennie KL, Jebb SA: Prevalence of obesity in Great Britain. Obesity Reviews. 2005, 6: 11-12. 10.1111/j.1467-789X.2005.00164.x.
LaCoursiere DY, Baksh L, Bloebaum L, Varnier MW: Maternal body mass index and self-reported postpartum depressive symptoms. Matern Child Health J. 2006, 10 (4): 385-390. 10.1007/s10995-006-0075-1.
Coates MM: Assisting the newborn to latch on to the very large breast: HELP!. J Hum Lact. 1989, 5 (3): 131-132. 10.1177/089033448900500310.
Durkin D: Lactation compromised in obese mothers. Central Lines. 2004, 20 (4): 8-
Hoover K: Latch-on difficulties: a clinical observation (Letter). J Hum Lact. 2000, 16 (1): 6-10.1177/089033440001600102.
Loveday CA: Is maternal obesity a cause of poor lactation performance?. Nutrition Reviews. 2005, 63 (10): 352-355. 10.1301/nr.2005.oct.352-355.
Marasco L, Marmet C, Shell E: Polycystic ovary syndrome: A connection to insufficient milk supply?. J Hum Lact. 2000, 16 (2): 143-148. 10.1177/089033440001600211.
Rasmussen KM, Hilson JA, Kjolhede CL: Obesity may impair lactogenesis II. J Nutr. 2001, 131: 3009S-3011S.
Rasmussen KM, Hilson JA, Kjolhede CL: Obesity as a risk factor for failure to initiate and sustain lactation. Adv Exp Med Biol. 2002, 503: 217-222.
Rasmussen KM, Lee VE, Ledkovsky TB, Kjolhede CL: A description of lactation counseling practices that are used with obese mothers. J Hum Lact. 2006, 22 (3): 322-327. 10.1177/0890334406290177.
Seidman DS: BMI and duration of breast feeding (letter). J Epidemiol Community Health. 1993, 47 (6): 508-
Yu CKH, Teoh TG, Robinson S: Obesity in pregnancy. BJOG. 2006, 113 (10): 1117-1125. 10.1111/j.1471-0528.2006.00991.x.
Michaelsen KF, Larsen PS, Thomsen BL, Samuelson G: The Copenhagen cohort study on infant nutrition and growth: duration of breastfeeding and influencing factors. Acta Pædiatr. 1994, 83 (6): 565-571.
Perez-Escamilla R, Segura-Millan S, Pollitt E, Dewey KG: Determinants of lactation performance across time in an urban population from Mexico. Soc Sci Med. 1993, 37 (8): 1069-1078. 10.1016/0277-9536(93)90441-6.
Riva E, Banderali G, Agostoni C, Silano M, Radaelli G, Giovannini M: Factors associated with initiation and duration of breastfeeding in Italy. Acta Paediatr. 1999, 88: 411-415. 10.1080/08035259950169792.
Thorsdottir I, Gunnarsdottir I, Palsson GI: Association of birth weight and breastfeeding with coronary heart disease risk factors at the age of 6 years. Nutr Metab Cardiovasc Dis. 2003, 13: 267-272. 10.1016/S0939-4753(03)80030-3.
Ferris AM, McCabe LT, Allen LH, Pelto GH: Biological and sociocultural determinants of successful lactation among women in eastern Connecticut. J Am Diet Assoc. 1987, 87 (3): 316 -3121.
Barnes J, Stein A, Smith T, Pollock JI, ALSPAC Study Team: Extreme attitudes to body shape, social and psychological factors and a reluctance to breast feed. J R Soc Med. 1997, 90: 551-559.
World Health Organization Expert Committee: Physical status: the use and interpretation of anthropometry. World Health Organ Tech Rep Ser. 1995, 854 (1-452):
Institute of Medicine: Nutrition during Pregnancy. 1990, Washington DC , National Academy Press
Donath SM, Amir LH, ALSPAC Study Team: Relationship between prenatal infant feeding intention and initiation and duration of breastfeeding: a cohort study. Acta Paediatr. 2003, 92 (3): 352-356. 10.1080/08035250310009293.
Webb K, Marks GC, Lund-Adams M, Rutishauser IHG, Abraham B: Towards a National System for Monitoring Breastfeeding in Australia: Recommendations for Population Indicators, Definitions and Next Steps. 2001, AusInfo, Canberra , Australian Food and Nutrition Monitoring Unit, University of Queensland
Hilson JA, Rasmussen KM, Kjolhede CL: Excessive weight gain during pregnancy is associated with earlier termination of breast-feeding among white women. J Nutr. 2006, 136: 140-146.
Kugyelka JG, Rasmussen KM, Frongillo EA: Maternal obesity is negatively associated with breastfeeding success among Hispanic but not black women. J Nutr. 2004, 134: 1746-1753.
Foster SF, Slade P, Wilson K: Body image, maternal fetal attachment, and breast feeding. J Psychosom Res. 1996, 41 (2): 181-184. 10.1016/0022-3999(96)00035-9.
Hilson JA, Rasmussen KM, Kjolhede CL: High prepregnant body mass index is associated with poor lactation outcomes among white, rural women independent of psychosocial and demographic correlates. J Hum Lact. 2004, 20 (1): 18-29. 10.1177/0890334403261345.
Grjibovski AM, Yngve A, Bygren LO, Sjostrom M: Socio-demographic determinants of initiation and duration of breastfeeding in northwest Russia. Acta Paediatr. 2005, 94: 588-594. 10.1080/08035250410023296.
Oddy WH, Li J, Landsborough L, Kendall GE, Henderson S, Downie J: The association of maternal overweight and obesity with breastfeeding duration. J Pediatr. 2006, 149: 185-191. 10.1016/j.jpeds.2006.04.005.
Scott JA, Binns CW, Graham KI, Oddy WH: Temporal changes in the determinants of breastfeeding initiation. Birth. 2006, 33 (1): 37-45.
Chapman DJ, Perez-Escamilla R: Maternal perception of the onset of lactation is a valid, public health indicator of lactogenesis stage II. J Nutr. 2000, 130: 2972-2980.
Dewey KG, Nommsen LA, Heinig MJ, Cohen RJ: Risk factors for suboptimal infant breastfeeding behavior, delayed onset of lactation, and excess neonatal weight loss. Pediatrics. 2003, 112 (3): 607-619. 10.1542/peds.112.3.607.
Forster D, McLachlan H, Lumley J: Factors associated with continuing to feed any breast milk at six months postpartum in a group of Australian women. Int Breastfeed J. 2006, 1: 18-10.1186/1746-4358-1-18.
Li R, Jewell S, Grummer-Strawn L: Maternal obesity and breastfeeding practices. Am J Clin Nutr. 2003, 77 (4): 931-936.
Baker JL, Michaelsen KF, Rasmussen KM, Sorensen TIA: Maternal prepregnant body mass index, duration of breastfeeding, and timing of complementary food introduction are associated with infant weight gain. Am J Clin Nutr. 2004, 80 (6): 1579-1588.
Amine EK, Al-Awadi F, Rabie M: Infant feeding pattern and weaning practices in Kuwait. J R Soc Health. 1989, 109 (5): 178-180.
Azziz R: Reproductive endocrinologic alterations in female asymptomatic obesity. Fertil Steril. 1989, 52: 703-725.
Norman RJ, Clark AM: Obesity and reproductive disorders: a review. Reprod Fertil Dev. 1998, 10: 55-63. 10.1071/R98010.
Akre J: Infant Feeding: The Physiological Basis. 1989, Geneva , World Health Organization, 21-23.
Whitaker ED: Blood and milk: medical and popular beliefs before the First World War. Measuring Mamma's Milk: Fascism and the Medicalization of Maternity in Italy. 2000, Ann Arbor , The University of Michigan Press, 29-61.
Segura-Millan S, Dewey KG, Perez-Escamilla R: Factors associated with perceived insufficient milk in a low-income urban population in Mexico. J Nutr. 1994, 124: 202-212.
Walker M: Influence of the maternal anatomy and physiology on lactation. Breastfeeding Management for the Clinician: Using the Evidence. 2006, Sudbury, Massachusetts , Jones and Bartlett Publishers, 51-82.
McAllan A: Breastfeeding with large breasts. [http://www.breastfeeding.asn.au/bfinfo/large.html]
Pasquali R, Gambineri A, Pagotto U: The impact of obesity on reproduction in women with polycystic ovary syndrome. BJOG. 2006, 113 (10): 1148-1159. 10.1111/j.1471-0528.2006.00990.x.
Arthur PG, Smith M, Hartmann PE: Milk lactose, citrate, and glucose as markers of lactogenesis in normal and diabetic women. J Pediatr Gastroenterol Nutr. 1989, 9 (4): 488-496.
Neubauer SH, Ferris AM, Chase CG, Fanelli J, Thompson CA, Lammi-Keefe CJ, Clark RM, Jensen RG, Bendel RB, Green KW: Delayed lactogenesis in women with insulin-dependent diabetes mellitus. Am J Clin Nutr. 1993, 58: 54-60.
Rowe-Murray HJ, Fisher JRW: Baby Friendly Hospital practices: Cesarean section is a persistent barrier to early initiation of breastfeeding. Birth. 2002, 29 (2): 124-131. 10.1046/j.1523-536X.2002.00172.x.
Capuco AV, Smith JJ, Waldo DR, Rexroad CE: Influence of prepubertal dietary regimen on mammary growth of Holstein heifers. J Dairy Sci. 1995, 78: 2709-2725.
Sejrsen K, Purup S, Vestergaard M, Foldager J: High body weight gain and reduced bovine mammary growth: physiological basis and implications for milk yield potential. Domest Anim Endocrinol. 2000, 19: 93-104. 10.1016/S0739-7240(00)00070-9.
Zanton GI, Heinrichs AJ: Meta-analysis to assess effect of prepubertal average daily gain of Holstein heifers on first-lactation production. J Dairy Sci. 2005, 88: 3860-3867.
Wadden TA, Brownell KD, Foster GD: Obesity: responding to the global epidemic. J Consult Clin Psychol. 2002, 70 (3): 510-525. 10.1037/0022-006X.70.3.510.
Donath S, Amir LH: Rates of breastfeeding in Australia by State and socioeconomic status: evidence from the 1995 National Health Survey. J Paediatr Child Health. 2000, 36 (2): 164-168. 10.1046/j.1440-1754.2000.00486.x.
Jones DA, West RR, Newcombe RG: Maternal characteristics associated with the duration of breast-feeding. Midwifery. 1986, 2: 141-146. 10.1016/S0266-6138(86)80005-5.
Amir LH, Donath SM: Does maternal smoking have a negative physiological effect on breastfeeding? The epidemiological evidence. Birth. 2002, 29 (2): 112-123. 10.1046/j.1523-536X.2002.00152.x.
Wee CC, McCarthy EP, Davis RB, Phillips RS: Screening for cervical and breast cancer: is obesity an unrecognized barrier to preventive care?. Ann Intern Med. 2000, 132 (9): 697-704.
Vallianatos H, Brennand EA, Raine K, Stephen Q, Petawabano B, Dannenbaum D, Willows ND: Beliefs and practices of first nation women about weight gain during pregnancy and lactation: Implications for women's health. The Canadian Journal of Nursing Research. 2006, 38 (1): 102-119.
Sarwer DB, Wadden TA, Foster GD: Assessment of body image dissatisfaction in obese women: specificity, severity, and clinical significance. J Consult Clin Psychol. 1998, 66 (4): 651-654. 10.1037/0022-006X.66.4.651.
Matz PE, Foster GD, Faith MS, Wadden TA: Correlates of body image dissatisfaction among overweight women seeking weight loss. J Consult Clin Psychol. 2002, 70 (4): 1040-1044. 10.1037/0022-006X.70.4.1040.
Stunkard AJ, Faith MS, Allison KC: Depression and obesity. Biol Psychiatry. 2003, 54 (3): 330-337. 10.1016/S0006-3223(03)00608-5.
Astbury J, Brown S, Lumley J, Small R: Birth events, birth experiences and social differences in postnatal depression. Aust J Public Health. 1994, 18: 176-184.
Rising R, Lifshitz F: Relationship between maternal obesity and infant feeding-interactions. Nutr J. 2005, 4: 17-10.1186/1475-2891-4-17.
Krishnamoorthy U, Schram CM, Hill SR: Maternal obesity in pregnancy: Is it time for meaningful research to inform preventive and management strategies?. BJOG. 2006, 113 (10): 1134-1140. 10.1111/j.1471-0528.2006.01045.x.
Donath SM, Amir LH, ALSPAC Study Team: The relationship between maternal smoking and breastfeeding duration after adjustment for maternal infant feeding intention. Acta Paediatr. 2004, 93: 1514-1518. 10.1080/08035250410022125.
Prentice AM, Goldberg GR, Prentice A: Body mass index and lactation performance. Eur J Clin Nutr. 1994, 48: S78-S89.
Rasmussen KM: Effects of under- and overnutrition on lactation in laboratory rats. J Nutr. 1998, 128: 390S-93S.
Flint DJ, Travers MT, Barber MC, Binart N, Kelly PA: Diet-induced obesity impairs mammary development and lactogenesis in murine mammary gland. Am J Physiol Endocrinol Metab. 2005, 288: E1179-87. 10.1152/ajpendo.00433.2004.
Grjibovski AM, Bygren LO, Svartbo B, Magnus P: Social variations in fetal growth in a Russian setting: an analysis of medical records. Ann Epidemiol. 2003, 13: 599-605. 10.1016/S1047-2797(03)00052-8.
Li R, Ogden C, Ballew C, Gillespie C, Grummer-Strawn L: Prevalence of exclusive breastfeeding among US infants: the Third National Health and Nutrition Examination Survey (Phase II, 1991-1994). Am J Public Health. 2002, 92 (7): 1107-1110.
Scott JA, Binns CW, Oddy WH, Graham KI: Predictors of breastfeeding duration: evidence from a cohort study. Pediatrics. 2006, 117 (4): e646-55. 10.1542/peds.2005-1991.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2393/7/9/prepub
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The author(s) declare that they have no competing interests.
Authors' contributions
LHA reviewed the literature and wrote the first draft of the paper. SD calculated summary statistics and revised the paper.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Amir, L.H., Donath, S. A systematic review of maternal obesity and breastfeeding intention, initiation and duration. BMC Pregnancy Childbirth 7, 9 (2007). https://doi.org/10.1186/1471-2393-7-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2393-7-9