
Abstract
Background
central loop of the gastrocnemius-soleus H-reflex latency (Tc) that looks promising in the diagnosis of S1 radiculopathy; has been investigated in a few studies and only two of them have focused on the constitutional factors affecting it. Although leg length has been shown to contribute to the Tc, the role of age is controversial. More confusing, none of the previously performed studies have used strict criteria to rule out subclinical neuropathy, so the results could be misleading. This study has been performed to determine the influence of leg length and age on Tc among a carefully selected group of healthy volunteers.
Methods
after screening forty six volunteers by taking history, physical examination and a brief electrophysiologic study; forty of them were selected to enroll into the study. Tc was obtained in all the study subjects and leg length and age were recorded for correlational analyses.
Results
this group was consisted of 26 males (65%) and 14 females (35%) with the age range of 19–65 years (Mean ± SD: 37 ± 10.7) and leg length range of 29.5–43 centimeters (36.4 ± 3.4).
Mean ± SD for Tc was 6.78 ± 0.3. We found a significant correlation between Tc and leg length (p value= 0.003, r = 0.49 and confidence interval 95% = 0.59–0.88), no significant correlation was found between age and Tc (p value= 0.48, r = 0.11), also we obtained the regression equation as: Tc = 0.04L + 5.28
Conclusions
in contrast to leg length, age was not correlated with Tc. Future studies are required to delineate other contributing factors to Tc.
Similar content being viewed by others


Background
The H-Reflex evaluates S1 radiculopathy [1]. The measured latency, however, is neither specific nor sensitive for S1 spinal nerve disease, as it traverses a long pathway. Pease et al [2] were the first who described the central loop of the gastrocnemius-soleus H-Reflex latency (Central S1 loop latency or Tc) and suggested it might be promising in the diagnosis of S1 radiculopathy [1, 2].
Unfortunately, Tc has been the subject of few studies, and as far as we know, only 5 articles [2–6] have been published on this issue so far. Among them, two have specifically evaluated the constitutional factors contributing to Tc. Leg length has been shown to have a significant effect on Tc. It is controversial whether age entails a similar effect. Wang et al [5] found a direct correlation between age and Tc. This observation was not confirmed by Ghavanini et al in an independent study [6].
The current study has been performed to determine the influence of leg length and age on Tc.
Methods
We enrolled 46 volunteers to this study after obtaining informed consent. Following a standard history taking, all of them underwent physical examination and a brief electrophysiologic evaluation [7] to rule out asymptomatic polyneuropathy, including determination of: right peroneal nerve conduction velocity (PNCV), distal motor latency of right deep peroneal nerve (PDML) and standard gastrocnemius-soleus H reflex latency (Tp). We defined our exclusion criteria as: history of sacral radiculopathy or diabetes mellitus or any other disease with potential to cause neuropathy, any abnormality in neurological or musculoskeletal physical examination, or any of the following findings: PNCV less than 40 m/s, PDML more than 5 ms or prolonged Tp (according to Braddom and Johnson's study [8].
Since we were supposed to rule out subclinical peripheral neuropathy and one component of the related electrodiagnostic study was measuring the distal motor latency for the deep peroneal nerve, the temperature at the dorsum of the foot was kept almost at 32°Celsius.
The leg length of each person was measured as the distance from middle of the midpopliteal crease to the point at the most proximal part of the medial malleolus, in centimeters.
Subject's age to the nearest year was also recorded.
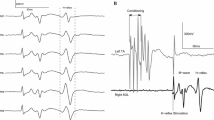
For obtaining Tc, we used DANTEC 2000 c equipment, the sensitivity, sweep, and filter were set at: 0.2–1mv/div, 5ms/div, and 2–10,000Hz respectively. The technique was the same as described in the Literature [1, 2]. Briefly: the volunteers lied prone on the examining table with the feet off the edge of the plinth. The E1 was placed at the middle of the line connecting midpoint of popliteal crease to the point at the most proximal part of the medial malleolus, and the E2 over the Achilles tendon (both were surface electrodes). The ground electrode was posed proximal to E1 and a disc electrode (anode) was placed on the anterior superior iliac spine. Then we inserted a monopolar 70mm needle (cathode) at a point 1cm medial to the posterior superior iliac spine, perpendicular to the frontal plane, and retracted it just a little after reaching the sacrum. Stimulus duration of 1 ms at 0.5 HZ was then applied while increasing current intensity to obtain both H and M waves simultaneously. M wave is the earlier wave and H is the later one. The interpeak latency was measured in milliseconds (ms) and recorded as Tc. This measurement was only performed on the right lower extremity.
Descriptive statistics were applied to depict Mean ± SD of age, leg length and Tc. The independent effect of leg length and age on Tc was assessed by multiple regression model. The analyses were performed using SPSS 10.0 software. Kolmogrov-Smirnov test was used for evaluating the normal distribution of the variables.
Results
From 46 subjects who volunteered to participate in this study; five cases were excluded after history taking and physical examination (two because of history of sacral radiculopathy, two because of diabetes mellitus and one because of asymmetry in ankle reflexes) and one case after electrophysiologic evaluation; thus we completed the study with 40 subjects. Subjects' characteristics are shown in table 1.
The group consisted of 26 males (65%) and 14 females (35%). Kolmogrov-Smirnov test showed normal distribution of the variables.
You are provided with the information below: (Mean ± SD) Age: 37.0 ± 10.7 years (range: 19–65); leg length: 36.4 ± 3.4 cm (range: 29.5–43); Tc= 6.78 ± 0.3 There was a significant correlation between Tc and leg length (P value = 0.003, r= 0.49, CI 95% = 0.59–0.88).
There was no correlation between Tc and age (p value = 0.48, r = 0.11) We also found this regression equation: Tc = 0.04L + 5.28 (L is leg length in centimeters, Tc is represented in milliseconds.)
Discussion
In this study we found a significant correlation between leg length and Tc, but we were unable to show such a relation between age and Tc.
Pease et al were the first, studied Tc [2, 4], and reported Mean ± SD of 7 ± 0.3ms which is very close to our results (Tc= 6.78 ± 0.3). They didn't specifically consider the leg length, age or any other potential confounding variables to Tc.
Zhu et al [3] evaluated 60 persons and reported Mean Tc: 6.8 ms and its SD: 0.33 ms, again close to our results. They also reported that Tc and person's height were correlated but didn't study any correlation between age and Tc.
Wang et al [5] evaluated 40 persons and found this regression equation:
Tc = 0.02A + 0.003H + 0.92 (H: Height and A: Age), and stated that age is a contributing factor on Tc.
Another research was performed by Ghavanini et al [6], in which 39 subjects were evaluated. The reported Tc ± SD was 6.9 ± 0.4; two regression equations were also suggested: Tc = 0.097Tp + 4.045 and Tc = 0.051L + 4.92 (L=leg length in centimeters); results are close to ours, and age was not found to affect Tc.
A summary of the above data plus detailed demographic data are provided in the table 2.
Limitations
In this study we focused on age and leg length as potential contributing factors on the Tc. we didn't control, randomize or observe other possible confounding (contributing) factors with potential to affect this parameter.
We observed a significant correlation between leg length and Tc (P value = 0.003, r= 0.49, CI 95% = 0.59–0.88), that is compatible to a previous published work [3] (r = 0.54, p value less than 0.01).
Had we found any association between Tc and age, the question might have been raised that subclinical neuropathy of old age could have been contributive; obviously, this is not the case in our study.
Although F-wave has been used to evaluate the possibility of proximal neuropathy; it was not measured in this study. Alternatively, we measured H-reflex latency to exclude proximal neuropathy [11].
It should be emphasized that noninvasive methodologies for the diagnosis of subclinical S1 radiculopathy are now available [12]. It is also acceptable to stimulate the S1 spinal nerve at the S1 foramen by magnet, instead of deep tissue needling; nevertheless, we used more popular techniques for this study.
Conclusions
We found that between age and leg length, only the latter can affect Tc. It may be reasonable to consider leg length for calculating Tc and to "narrow" the normal limits.
Further studies with larger sample sizes are required for detecting other contributing factors and standardizing Tc according to leg length.
Abbreviations
- Tc :
-
central loop of the gastrocnemius-soleus H-Reflex latency
- Tp :
-
gastrocnemius-soleus H-Reflex latency
- PNCV:
-
right peroneal nerve conduction velocity
- PDML:
-
right peroneal nerve distal motor latency
References
Dumitru D, ed: Electrodiagnostic medicine. 2002, Philadelphia: Hanley and Belfus,inc., 2
Pease WS, Kozakiewicz R, Johnson EW: Central loop of the H reflex : Normal values and use in S1 radiculopathy. Am J phys Med Rehabil. 1997, 76 (3): 182-184. 10.1097/00002060-199705000-00002.
Zhu Y, Starr A, Haldeman S, Chu JK, Sugerman RA: Soleus H reflex to S1 nerve root stimulation. Electroencephalogr Clin Neurophysiol. 1998, 109: 10-14. 10.1016/S0924-980X(97)00058-1.
Pease WS, Lagattuta FP, Johnson EW: Spinal nerve stimulation in S1 radiculopathy. Am J Phys Med Rehabil. 1990, 69 (2): 77-80.
Wang R, Liu X, Guo Y: Hoffmann reflex elicited by magnetic stimulation of S1 nerve roots in the diagnosis of diabetic radiculopathy. Zhonghua Yi xue Za Zhi. 1998, 78 (7): 501-503. chinese
Ghavanini MR, Ghadi RS, Ghavanini AA: The central loop of the H reflex in the S1 spinal nerve: Normal values and constitutional influencing factors. Electromyogr clin neurophysiol. 2001, 41 (6): 259-262.
Frigns CJM, Laman DM, Van Dujin MAJ, van-Duijn H: Normal values of patellar and ankle tendon reflex latencies. Clin Neurol Neurosurg. 1997, 99: 31-36. 10.1016/S0303-8467(96)00593-8.
Braddom RL, Johnson EW: Standardization of H reflex and diagnostic use in S1 radiculopathy. Arch phys Med Rehabil. 1974, 55: 161-166.
Strakowski JA, Redd DD, Johnson EW, Pease WS: H-reflex and F wave latencies to soleus normal values and side to side differences. Am J Phys Med Rehabil. 2001, 80: 491-493. 10.1097/00002060-200107000-00004.
Buschbacher RM: Normal range for H-reflex recording from the calf muscles. Am J Phys Med Rehabil. 1999, 78 (6 Suppl): S75-79. 10.1097/00002060-199911001-00014.
Braddom RL, Johnson EW: Standardization of the H reflex and diagnostic use in s1 radiculopathy. Arch phys med rehabil. 1974, 55: 161-166.
Mazzocchio R, Scarfo GB, Mariottini A, Muzii FM, Palma L: recruitment curve of the soleus H reflex in chronic back pain and lumbosacral radiculopathy. BMC musculoskeletal disorders. 2001, 2: 4-10.1186/1471-2474-2-4.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2377/4/11/prepub
Acknowledgements
The authors would like to thank:
Ali Bidari, MD, assistant professor of rheumatology, Iran university of medical sciences, for his great help in the revision of the manuscript
Mojtaba Mahjoob, MD, resident of surgery, and Masoome Rostamzade, English instructor, for translating the manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
None declared.
Authors' contribution
SS: examining the cases, calculation of TC, writing the paper.
MRAG: suggesting the research, supervision and helping with calculation of TC.
AA: examining the cases, calculation of TC
PJ: statistical consultant (data analysis)
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Sadeghi, S., Ghavanini, M., Ashraf, A. et al. Effects of age and leg length upon central loop of the Gastrocnemius-soleus H-reflex latency. BMC Neurol 4, 11 (2004). https://doi.org/10.1186/1471-2377-4-11
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2377-4-11