
Abstract
Background
IgAN is the most common type of glomerulonephritis in the world. Between 15 and 40 percent of adults and children diagnosed with IgAN eventually progress to ESRD. Despite the need for effective treatment strategies, very few RCTs for IgAN have been performed. The most effective therapies for IgAN appear to be corticosteroids, ACEi, and FOS that contain a high concentration of omega 3 fatty acids. While ACEi and FOS are generally well tolerated with minimal side effects, the use of high dose steroids over a long course of therapy is often associated with significant morbidity.
Objective of the study
The objective of the study is to test the hypothesis that treatment with the immunosuppressive agent, MMF, will lead to significant and sustained improvement in urinary protein excretion in patients with IgAN who have been pre-treated (and continue to be treated) with ACEi and FOS compared to a placebo control group of patients receiving comparable doses of ACEi and FOS without MMF.
Design
After a three month treatment period with the ACEi, lisinopril and the FOS, Omacor®, 100 (2 × 50) patients with IgAN and a urinary P/C ratio ≥ 0.6 (males) and ≥ 0.8 (females) and an estGFR ≥ 40 ml/min/1.73 m2 will be randomized to treatment with either MMF or placebo for one year. All patients will be followed off study drug for a second year, but will continue treatment with lisinopril and Omacor® for the two year duration of the study. The primary outcome measure of change in urine P/C ratio will be assessed at the end of years one and two.
Similar content being viewed by others


Background
IgAN is the most common type of glomerulonephritis in the world [1, 2]. Between 15 and 40 percent of adults and children diagnosed with IgAN will eventually progress to end stage renal disease (ESRD) [3–6]. Effective treatment strategies are needed to prevent ESRD in patients with this condition. To date, the following RCTs for treatment of IgAN have been completed: FOS vs. placebo with the primary endpoint of decline in kidney function [7], intravenous and oral corticosteroids with the primary endpoint of decline in kidney function [8], oral corticosteroids and azathioprine vs. supportive care with the primary endpoint of reduction in urinary protein excretion [9], "low-dose" oral corticosteroids with the primary endpoint of reduction in urinary protein excretion [10], ACEi vs. placebo with the primary endpoint of reduction of proteinuria [11], MMF vs. prednisone with the primary endpoint of reduction of proteinuria [12], MMF vs. placebo with the primary endpoint of reduction of proteinuria [13–15].
The results of this study group's first trial of FOS vs. alternate day prednisone vs. placebo with the primary endpoint of decline in kidney function [16] have recently been published in abstract form [17]. We found no significant difference with respect to decline in renal function among the alternate-day prednisone, FOS and placebo groups. We did find a significant decline in proteinuria after two years of treatment for both the prednisone and FOS groups as compared to the placebo group.
Ongoing RCTs using decline in GFR as the primary outcome measure include a European pediatric study and comparing ACEi vs. placebo [18], an Italian study comparing ACEi and prednisone to ACEi alone [19], and another Italian study examining intravenous and oral corticosteroids with and without azathioprine [20].
The most effective therapies for IgAN appear to be FOS that contain a high concentration of omega 3 fatty acids [7], corticosteroids [8–10], and ACEi [11]. However, the use of moderate to high dose steroids over a long course of therapy is may be associated with significant morbidity and the most recent results of the effect of FOS suggest that such therapy may only be successful in delaying progression for a few years rather than permanently preventing progressive disease [21]. FOS and ACEi inhibitors are widely used for the treatment of IgAN and are usually well tolerated. Hence we believe that giving both FOS and ACEi to all patients in the proposed study is warranted and will greatly enhance patient recruitment by providing some form of treatment for all subjects in the trial.
MMF is an immunosuppressive agent that acts to suppress antibody formation by B-cells through impairment of de-novo purine synthesis [22]. Case series suggest that MMF may be effective in reducing proteinuria in a variety of glomerular diseases including IgAN [23–25], and two recent Chinese RCTs found MMF to be significantly better than prednisone for reduction of proteinuria in patients with IgAN [12, 13]. However, two other recent RCTs showed no benefit for MMF in reduction in proteinuria in patients with IgAN [14, 15].
Methods/design
Objective of the study
To undertake a multicenter, RCT designed to test the hypothesis that treatment with MMF will lead to significant and sustained improvement in proteinuria in patients with IgAN who have been pre-treated (and continue to be treated) with ACEi and FOS compared to a placebo control group of patients receiving comparable doses of ACEi and FOS without MMF.
Rationale for using change in proteinuria as a primary endpoint
The most obvious endpoint for treatment failure in patients with IgAN is progression to ESRD. However, since the period from diagnosis to ESRD in patients with normal renal function at onset may be over 10 years, most studies of therapy for IgAN have used surrogate endpoints, such as improvement or stability of serum creatinine, or decline in amount of proteinuria. Deterioration in renal function, (e.g., 50% loss of function), has been the surrogate endpoint that most closely associates with the primary endpoint of progression to ESRD.
Considerable data from clinical trials suggest that renal function will be protected and proteinuria reduced in patients with non-diabetic glomerular disease treated with ACEi [26–28]. An unproved assumption is that significant lowering of urinary protein excretion will result in preservation of renal function. If this assumption is in fact true, then reduction in protein excretion in a short term study of two years may be associated with preservation of renal function for a much longer (5 to 20 years) or even indefinite period of time. This is the basis for our decision to use reduction in proteinuria as the primary outcome measure in this study.
Study design
This is a multicenter, double-blind placebo-controlled, RCT designed to test the efficacy of MMF in patients with IgAN who are at risk for development of progressive disease. All subjects will receive treatment with Omacor®and lisinopril during a 3-month lead in period and for the subsequent 2-year period of study. Adult subjects who are unable to tolerate lisinopril may exit the study or may be converted to losartan and continue in the study. Each subject will receive a year of treatment with the study drug (MMF) or placebo followed by a year of follow-up off study drug. This multicenter clinical trial will be conducted in up to 50 clinical centers where patients will be recruited and studied. The study will be coordinated by the ACC at Medical City Dallas Hospital, Dallas, TX.
Primary outcome measure
The primary outcome measure will be change from entry level in urine P/C ratio. Data for this outcome will be examined every 6 months until the end of the study two years after randomization.
Secondary outcome measure
The secondary outcome measure will be change in estGFR [29]. We realize that the likelihood of detecting significant changes in GFR in this short-term study is remote.
Summary of study phases
There are four phases of study for each subject. Phase 1 or the screening phase will be from one to four week duration. During this phase each potential subject will be evaluated to determine if he/she is eligible for the study. The renal biopsy report will be examined to confirm the diagnosis of IgAN and to determine the severity of renal injury at the time of biopsy. Subjects are eligible for entry if proteinuria determined in the central laboratory is over 1 gm per day on a 24-hour collection or the UPr/Cr ratio on an aliquot from that collection is ≥0.6 in a male taking an ACEi or >0.8 female in a taking an ACEi. The minimum acceptable estGFR at entry is ≥50 ml/min/1.73 m2 for subjects who are not taking an ACEi and ≥40 ml/min/1.73 m2 for subjects who are taking an ACEi.
Phase 2 or the lisinopril/Omacor® lead-in phase will last for three months. During this phase each subject will be established on a stable dose of both lisinopril (or losartan if necessary) and Omacor®. At the end of this phase male subjects with a UPr/Cr ratio ≥ 0.6 and female subjects with a UPr/C ratio ≥ 0.8 will be eligible for randomization. The estGFR must be ≥40 ml/min/1.73 m2 prior to randomization.
Phase 3 is the study drug treatment phase and will last for 12 months. Due to the large number of centers required to recruit sufficient subjects, stratification by center is impractical. Block randomization will be performed in equal blocks of 4 for each of the two strata. After the ACC has determined that the patient is eligible for the study, the biostatistician, based upon the randomization scheme constructed using a computer-based pseudo-random number generator, will determine the treatment group assignment. The biostatistician will notify the study pharmacist of the assignment and he/she will arrange for delivery of the appropriate study medication (MMF or matched placebo) the center investigator responsible for management of the patient. Subjects will receive MMF or placebo at a dose that is based on body size.
During phase 4, the post-treatment Phase subjects will be monitored carefully to determine if they show changes in urine Pr/Cr ratio or estGFR after MMF/placebo has been discontinued. (They will still receive Omacor® and lisinopril (or losartan if necessary).
Inclusion criteria
Criteria for inclusion in the study are: 1) patient age above 7 and less than 70 years, 2) renal biopsy diagnostic for IgAN based on immunohistologic staining for IgA that is greater than or equal to staining for IgG and IgM after the biopsy report has be evaluated by one of the study pathologists (entry into the study does not depend upon any specific time interval between the time of the renal biopsy and the time of entry), 3) ability to swallow the oral medications used in the study, 4) signed informed consent by subjects ≥ 18 years of age, and parent/guardian of any subject < 18 years of age with a subject aged ≥ 7 years to <18 years of age also signing an age-appropriate assent form, 5) urine Pr/Cr ratio ≥ 0.6 for males and ≥ 0.8 for females prior to randomization, 6) for female subjects of childbearing potential a negative pregnancy test one week prior to starting lisinopril, and again less than one week before starting MMF or placebo.
Exclusion criteria
Criteria for exclusion from the study are: 1) clinical and histologic evidence of systemic lupus erythematosus, 2) well-documented history of Henoch-Schönlein purpura (previous non-specific abdominal pain or rash does not exclude a subject), 3) cirrhosis, chronic active liver disease, hepatitis B, hepatitis C, 4) history of significant gastrointestinal disorder (e.g.: severe chronic diarrhea or active peptic ulcer disease, 5) HIV, 6) any systemic infection or history of serious infection within one month of entry 6) ANC < 2000/mm3, 7) HCT < 28% (anemic subjects may be reevaluated after the anemia has been treated), 8) estGFR < 40 ml/min/1.73 m2 at time of randomisation (it is acceptable for the estGFR to fall to less than 40/ml/min1.73 m2 during treatment with MMF or placebo provided the level prior to randomization is still ≥60% of the pre-entry value), 9) known contraindication to the administration of MMF, OMACOR® or lisinopril (or losartan if used instead of lisinopril), 10) other major organ system disease or malignancy except skin cancer fully excised more than 5 years prior to entry, 11) current or prior treatment with MMF or azathioprine, 12) pregnancy or breast feeding at time of entry or unwillingness to comply with measures for contraception, 13) current or recent (within 30 days) exposure to any investigational drug.
Exit criteria (reasons for permanently discontinuing study medication)
Reasons for permanently discontinuing study medication are: 1) ingestion of prohibited medication (MMF, azathioprine, cyclophosphamide, cholestyramine; NSAIDs, Cox 2 inhibitors, cimetidine, vitamin E in doses greater than those provided in a daily multivitamin tablet, 2) a lipid lowering medication other than cholestyramine (e.g. a statin) begun after study entry (such medication may be continued if the subject was receiving it at the time of entry, 3) corticosteroid therapy to treat the IgAN, (a short course (<7 days) may be given for an acute non-renal condition e.g., an acute asthma episode), 4) a major adverse event (e.g., life-threatening infection, allergic reaction to MMF, severe gastrointestinal disorder, or development of any malignancy, 5) persistent gastrointestinal disorder of moderate severity after MMF dose Step 2 reduction for 2 weeks, 6) HCT persistently lower than 25% after MMF dose Step 2 reduction for 2 weeks, 7) ANC persistently lower than 1500/mm3 after MMF Step 2 reduction for 2 weeks, 8) ANC lower than 1000/mm3 at any time (see page 6 for MMF step reductions in dosage), 9) administration of a live viral vaccine, 10) patient/parent withdrawal of consent to participate, 11) patient moving out of the area to a location with participating center within a reasonable distance, 11) pregnancy, 12) sexually active female not using two forms of birth control, 13) interruptions of MMF treatment for 28 days or more cumulatively, or any single interruption of more than 21 consecutive days, 14) inability to tolerate lisinopril (or losartan in adult patients), 15) estGFR less than 60% of level reported at pre-entry visit at any time during the study confirmed on a repeat specimen one month later.
Study medications
The dose of MMF to be given during most of the study will be between 25 mg/kg/day and 36 mg/kg/day with a maximum dose 1 gm BID. The initial dose to be used (in the first 2 weeks of therapy) will be approximately 1/2–2/3 of the full dose (as shown in the Table below). Roche Laboratories will provide MMF capsules and matching placebo capsules. Capsules are produced in strength of 250 mg and the dose used will be based upon the weight of the subject (Table 1).
If a subject develops gastrointestinal toxicity from MMF or HCT is <25% or ANC is 1000–1500, the dose will be reduced in accordance with Step 1 of a specific protocol (Table 2). If after 2 weeks, any of these abnormalities persist, the dose of MMF will be reduced again in accordance with Step 2 of the protocol (Table 2). If any of the problems persist 2 weeks after the Step 2 reduction, MMF will be discontinued.
In a case of severe signs of MMF toxicity, more rapid reduction of MMF is allowed. If ANC is <1000, MMF must be stopped immediately. After a dose reduction or interruption, unless medically contra-indicated, MMF will be reinstituted within 14 to 21 days in increments until the protocol recommended MMF dose is achieved. The dose will be increased in reverse order to that given in the above table until the optimal tolerable dose is found. A maximum stepwise increments of 500 mg is used for subjects ≥ 55 kg and 250 mg for subjects < 55 kg.
Occurrence of gastrointestinal toxicity requires a decision as to whether or not to alter MMF dosing. This decision is based on several factors. Diarrhea will be treated as follows: infectious causes (e.g., C. difficile and enteropathogens) should be ruled out and treated if necessary. Once these infectious causes have been excluded, agents such as Lomotil or tincture of opium may be used to decrease diarrhea so that MMF dosing can be maintained. Finally, if diarrhea persists, the MMF dose will be reduced as per the above protocol.
Omacor® (omega-3 fatty acids) is provided by the study and dispensed at a dose of 4 grams per day for all patients with body surface area ≥1 m2. The dose will be adjusted to the nearest number of capsules corresponding to the body surface area in patients less than 1 m2. The active ingredient in Omacor® capsules is an oil which consists of ethyl esters, mainly EPA and (DHA). The concentration of EPA ethyl ester is approximately 47% and DHA ethyl ester approximately 37%. In addition the concentrate contains ethyl esters of other omega-3 fatty acids, and also ethyl esters of other fatty acids. Four mg of α-tocopherol is added as an antioxidant.
Lisinopril will be dispensed at an initial dose of 5–20 mg per day depending on the size of the subject (Table 3). If this is well tolerated the dose will be doubled after 1 month of therapy to 10–40 mg per day. For subjects that are hypertensive after the "higher dose" of lisinopril has been given for one month, the dose may be further increased to twice the "higher dose" (maximum 20 – 80 mg/day depending on size of subject).
Treatment of hypertension
Hypertension will initially be treated with lisinopril, using the doses listed above. If a patient is on an anti-hypertensive medication other than lisinopril at the time of entry, that medication will be stopped and, if possible, control of the patient's hypertension will be obtained using lisinopril. Persistent hypertension will be defined by a systolic BP > 135 mm/Hg, a diastolic BP > 85 mm/Hg, or either level at > 95th percentile for age on two consecutive visits. For subjects who have persistent hypertension despite receiving the higher dose of lisinopril, additional BP medication will be used with the selection of medication based upon the local physician's preference. However, the use of lisinopril doses greater than 20–80 mg/day, and/or angiotensin receptor blockers (other than losartan substitution for lisinopril) is prohibited by the study.
This strategy of treatment for hypertension in patients entered into this study with a non-ACEi medication is both ethical and will reduce the chance of the treatment given for hypertension becoming a confounding variable for the trial.
Clinical safety monitoring
Participating investigators will report within 72 hours all serious adverse events that occur after study medication starts. Members of the SMC evaluate this information. They will disseminate reports of serious adverse drug reactions to all participating centers for submission to their respective IRBs. This centralized function permits ongoing evaluation of risks associated for patients with IgAN taking MMF and will enhance prompt dissemination of information as appropriate. Uniform reporting of all serious adverse events to the ACC in this study will make possible a much more accurate determination of the degree to which any SAE that may be encountered is, in fact, drug related.
The investigator is required to report all treatment-emergent adverse events that are observed or reported during study phase 2 (i.e., treatment phase). This applies regardless of a) the clinical significance or b) the assessment of study drug causality. All such events must be recorded on the AEF.
An adverse event is defined as any untoward medical occurrence in a patient who takes the study medication. It does not necessarily have to have a causal relationship with this treatment. This may be any unfavorable and unintended sign (e.g., abnormal laboratory finding), symptom or disease, which is observed after exposure to the study medication, whether or not considered, related to the treatment.
An adverse drug reaction is defined as a noxious and unintended response to a study medication, at any dose. A causal relationship between the study medication and the adverse event must be at least a reasonable possibility, i.e., the relationship cannot be ruled out.
A SAE or reaction is any untoward medical occurrence (at any dose) that: a) results in death, b) is life-threatening, c) requires inpatient hospitalization or prolongs an existing hospitalization, d) results in persistent or significant disability/incapacity or, is a congenital anomaly or birth defect in an infant exposed prenatally. Other events that places the subject in jeopardy or that require intervention to prevent one of the above outcomes (e.g., pregnancy) should also be considered serious. All SAE are reported to the ACC within 72 hours.
A treatment-emergent event is any sign, symptom or disease that either a) is not present prior to exposure to study medication, or b) if already present, worsens in either intensity or frequency following exposure to study medication.
The initial report of the SAE may be communicated by phone, but is followed up as soon as possible by sending an "initial" report on the SAE Form to the ACC. The nature and severity of each event is compared with known adverse reactions already published in the current product information pages supplied by Roche. If it is determined that an unexpected, serious adverse event has occurred, a report is provided to investigators at all study sites. Each investigator should forward the information to the local IRB.
Situations requiring the use of excluded medications
If it is medically necessary to treat a patient with an excluded medication that is known to interact with MMF or affects the action of MMF, the study drug may be interrupted or the dose decreased as deemed necessary by the investigator.
If it is medically necessary to treat the patient with an excluded medication that affects the primary outcome measure, the investigator should again proceed in accordance with the medical needs of the patient. An interruption of study medication of no more than 14 consecutive days is permissible. If the interruption is longer, the patient should not resume taking MMF, and should be seen in the clinic as soon as possible. Then resume regular scheduled visits.
Data management
Data arrives at the ACC in two forms – CRFs and LabCorp generated reports. The CRFs are used to record the following: 1) demographic history, 2) physical examination variables, 3) study and concurrent medications, 4) adverse events
LabCorp will report all laboratory data on standardized report forms. LabCorp will send reports of laboratory values directly to the ACC. The Data Manager and a clinical coordinator at the ACC will double enter data into the database. Irrecoverable missing values will be documented with appropriate codes in the database. Periodic computerized audit reports will be run to monitor quality and completeness. The database is stored on a network drive that is backed up to tape daily by the Information Systems Department at Medical City Dallas Hospital.
In order to insure confidentiality, data from each patient will be recorded in the computer database with a unique contributing center code, study code, sequence number and patient initials. Patient names are never given to LabCorp or the ACC. Each study center is assigned a code number. The ACC assigns a unique patient identification code when the screening evaluation checklist is received.
Sample size calculation
The primary study outcome is the change in urinary protein excretion (urine Pr/Cr ratio) at the conclusion of the three-month "lead-in" period and the level obtained at each year of the study. A current examination of data from patients with IgAN entered in our previous study indicates mean baseline urine P/C ratio of 1.90 (SD = 1.80; External Advisory Committee Report, 2001). Although a urine P/C ratio of 1.90 reflects a reasonable baseline measure, we expect that urine P/C ratios will fall during the three-month "lead-in" period in response to lisinopril and to a lesser extent, Omacor®. Previous research indicates that more than half of patients who received ACEi for a period of twelve months displayed a twenty-five percent reduction in their urinary protein excretion ratios [30]. In addition, at least one study indicates that a further reduction of UPr/Cr ratios can be expected in response to FOS [31]. Based on this previous research, we expect that patients receiving ACEi and the FOS will display nearly a forty percent reduction in urine P/C ratio upon conclusion of the three-month "lead in" period. Based on this assumption, we hypothesize that the mean urine P/C ratio for all patients will be 1.20 upon conclusion of the three-month "lead-in" period. We further hypothesize that the mean urine P/C ratio for the ACEi/FOS plus MMF group will be 0.50 (reduction of 0.70) after one year of MMF. In contrast, we hypothesize that for the ACEi/FOS plus placebo group the urine P/C ratio will remain constant at 1.20 after one year of placebo. Assuming a 15% attrition rate and a 1.80 population standard deviation, a sample size of 50 patients per group would be required to obtain a 0.05 significance level with a power of 0.80.
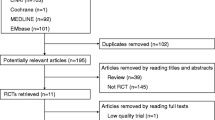
Although a final sample size of 50 patients per group will be needed at the commencement of phase three, many more patients will be initially required. We expect to screen approximately 200 patients during the phase one screening. Based on our experience with the previous IgAN treatment trial, we anticipate twenty-five percent of these 200 patients will not meet the initial inclusion criteria. The exclusion of these 50 patients will leave approximately 150 for inclusion in the phase two "lead-in" period. Upon conclusion of the three-month "lead-in" period, we expect that a third of these patients will fail to meet the inclusion criteria. These patients will have already displayed clinically significant benefit (i.e., urine P/C ratio less than 0.6 for males and 0.8 for females) from the "lead-in" treatment regimen. In summary, we plan to screen 200 patients, to include 150 patients in the "lead-in" phase, and to randomize 100 patients into one of two comparison groups.
Statistical approach
Following the conclusion of the first year of the study, a statistical summary report will be prepared. This report will summarize the progress of the study, study patient characteristics, and safety issues.
Baseline comparability between the two treatment groups will be evaluated with respect to entry criteria (e.g., demographics, laboratory results). Chi-square and t-test will be used to assess differences between the two groups on the baseline variables. Any variables that are found to be discrepant between the two groups and that are related to the outcome variables will be treated as covariates in later analyses.
In order to evaluate the patients' change in urine P/C ratios, two strategies will be employed. We hypothesize that patients treated with ACEi, FOS, and MMF will demonstrate nearly a sixty percent decrease in their UPr/Cr ratios. In contrast, we expect those patients treated with ACEi, FOS, and placebo to maintain relatively constant urine P/C ratios. The Kaplan-Meier method will be used to estimate the time in which patients are likely to display the 60% decrease in urine P/C ratio during the two-year study period. Secondly, rate of change (slopes) in the primary outcome measures will be estimated for each patient. These estimates will then be compared between groups to assess for differences in rate of change between the two treatment groups.
Publication of study results
All publications will be authored by members of the scientific advisory committee. Co-authors will have contributed to the design, analysis and actual reporting of the study.
Study investigators
Steering committee: RJ Hogg, N Nardelli, C Adkins, L Fitzgibbons, D Parrott, J Miller
Scientific planning committee: RJ Hogg, WA Briggs, DC Cattran, JC Chan, JJ Dillon, RJ Falk, L Fitzgibbons, RJ Glassock, JC Jennette, BA Julian, R Sibley, RJ Wyatt
Safety monitoring committee: JC Chan, JV Donadio, RJ Glassock, L Fitzgibbons, J Miller, D Parrott
Discussion
We report the protocol of a RCT designed to test the efficacy of MMF in reducing proteinuria in patients with IgAN. This study utilizes the novel approach of examining the use of an immunosuppressive agent (MMF) that is not being used in conjunction with corticosteroid therapy. In the previous study form our group, subject recruitment was hampered by the unwillingness of some subjects to consider the possibility of corticosteroid treatment assignment and the difficulty some patients or their parents had in being assigned to a placebo group. We anticipate better acceptance of this protocol since corticosteroids will not be used and subjects in both groups will be treated with ACEi and FOS.
The use of change in urine P/C ratio as primary outcome measure, rather than decrease in kidney function will allow for completion of the study and analysis of data within in a relatively short period of 4 to 5 years as opposed to 6 to 10 years for studies that utilize change in renal function as the primary outcome measure.
Abbreviations
- IgAN:
-
IgA nephropathy
- ESRD:
-
end stage renal disease
- RCTs:
-
Randomized controlled trials
- FOS:
-
fish oil supplements
- ACEi:
-
angiotensin converting enzyme inhibitor
- MMF:
-
mycophenolate mofetil
- P/C:
-
protein to creatinine
- ACC:
-
administrative co-ordinating center
- estGFR:
-
estimated glomerular filtration rate
- HIV:
-
human immunodeficiency virus
- ANC:
-
absolute neutrophil count
- HCT:
-
hematocrit
- NSAID:
-
non-steroid anti-inflammatory drug
- EPA:
-
eicosapentaenoic acid
- DHA:
-
docosahexaenoic acid
- SMC:
-
safety monitoring committee
- IRB:
-
institutional review board
- AEF:
-
adverse event form
- SAE:
-
serious adverse event
- CRF:
-
case report form
References
D'Amico G: The commonest glomerulonephritis in the world: IgA nephropathy. Quart J Med. 1987, 64: 709-727.
Levy M, Berger J: Worldwide perspective of IgA nephropathy. Am J Kidney Dis. 1988, 12: 340-347.
Droz D: Natural history of primary glomerulonephritis with mesangial deposits of IgA. Contrib Nephrol. 1977, 2: 150-157.
Velo M, Lozano L, Egido J, Gutierrez-Milet V, Hernando L: Natural history of IgA nephropathy followed up for more than 10 years in Spain. Semin Nephrol. 1987, 7: 346-50.
Wyatt RJ, Kritchevsky SB, Woodford SY, Miller PM, Roy S, Holland NH, Jackson E, Bishof NA: IgA nephropathy: Long-term prognosis for pediatric patients. J Pediatr. 1995, 127: 913-919.
Radford MG, Donadio JV, Bergstralh EJ, Grande JP: Predicting renal outcome in IgA nephropathy. J Am Soc Nephrol. 1997, 8: 199-207.
Donadio JV, Bergstralh EJ, Offord KP, Spencer DC, Holley KE: A controlled trial of fish oil in IgA nephropathy. N Engl J Med. 1994, 331: 1194-9. 10.1056/NEJM199411033311804.
Pozzi C, Bolasco PG, Fogazzi GB, Andrulli S, Altieri P, Ponticelli C, Locatelli F: Corticosteroids in IgA nephropathy: a randomised controlled trial. Lancet. 1999, 353: 883-887. 10.1016/S0140-6736(98)03563-6.
Yoshikawa N, Ito H, Sakai T, Takekoshi Y, Honda M, Awazu M, Ito K, Iitaka K, Koitabashi Y, Yamaoka K, Nakagawa K, Nakamura H, Matsuyama S, Seino Y, Takeda N, Hattori S, Ninomiya M: A controlled trial of combined therapy for newly diagnosed severe childhood IgA nephropathy. The Japanese Pediatric IgA Nephropathy Treatment Study Group. J Am Soc Nephrol. 1999, 10: 101-109.
Katafuchi R, Ikeda K, Mizumasa T, Tanaka H, Ando T, Yanase T, Masutani K, Kubo M, Fujimi S: Controlled, prospective trial of steroid treatment in IgA nephropathy: A limitation of low-dose prednisolone therapy. Am J Kidney Dis. 2003, 41: 972-983. 10.1016/S0272-6386(03)00194-X.
Maschio G, Cagnoli L, Claroni F, Fusaroli M, Rugiu C, Sanna G, Sasdelli M, Zuccala A, Zucchelli P: ACE inhibition reduces proteinuria in normotensive patients with IgA nephropathy: a multicentre, randomized, placebo-controlled study. Nephrol Dial Transplant. 1994, 9: 265-269.
Chen X, Chen P, Cai G, Wu J, Cui Y, Zhang Y, Liu S, Tang L: A randomized control trial of mycophenolate mofetil treatment in severe IgA nephropathy. Zhonghua Yi Xue Za Zhi. 2002, 82: 796-801.
Tang S, Leung JCK, Tang AWC, Ho YW, Chan LYY, Chan TM, Lai KN, for the Hong Kong Immunoglobulin A Study Group: A prospective, randomized, case-controlled study on the efficacy of mycophenolate mofetil (MMF) for IgA nephropathy (IgAN) patients with persistent proteinuria despite angiotensin blockade. J Am Soc Nephrol. 2003, 14: 752A-753A.
Frisch G, Lin J, Rosenstock J, Markowitz G, D'Agati V, Radhakrishan J, Valeri A, Appel G: Mycophenolate mofetil vs. placebo in patients at high risk for progressive IgA nephropathy: A double blind RCT. J Am Soc Nephrol. 2003, 14: 753A-
Maes BD, Evenepoel P, Kuypers D, Messiaen T: A prospective placebo-controlled randomised single center study of mycophenolate mofetil treatment for IgA nephropathy: Lack of clinical efficacy after two years. J Am Soc Nephrol. 2001, 12: 114A-10.1159/000047690.
Hogg RJ, for the Scientific Planning Committee of the IgA Nephropathy Study: A randomized, placebo-controlled, multicenter trial evaluating alternate-day prednisone and fish oil supplements in young patients with immunoglobulin A nephropathy. Am J Kidney Dis. 1995, 26: 792-796.
Hogg RJ, Lee J, Nardelli NA, Cattran D, Hirschman G, Julian BA: Multicenter placebo-controlled trial of alternate-day prednisone (QOD-PRED) or daily omega-3 fatty acids (OM-3 FA) in children and young adults with IgA nephropathy (IgAN). Report from the Southwest Pediatric Nephrology Study Group. J Am Soc Nephrol. 2003, 14: 751A-
Coppo R, Chiesa M, Peruzzi L, Amore A: Treatment of IgA nephropathy with angiotensin converting enzyme inhibitors: design of a prospective randomized multicenter trial. J Nephrol. 2001, 14: 447-452.
Manno C, Gesualdo L, D'Altri C, Rossini M, Grandaliano G, Schena FP: Prospective randomised controlled multicenter trial on steroids plus ramipril in proteinuric IgA nephropathy. J Nephrol. 2001, 14: 248-252.
Locatelli F, Pozzi C, Del Vecchio L, Andrulli S, Pani A, Fogazzi G, Altieri P, Ponticelli C: Combined treatment with steroids and azathioprine in IgA nephropathy: design of a prospective randomised multicentre trial. J Nephrol. 1999, 12: 308-311.
Donadio Jr JV, Grande JP, Bergstralh EJ, Dart RA, Larson TS, Spencer DC: The long-term outcome of patients with IgA nephropathy treated with fish oil in a controlled trial. Mayo Nephrology Collaborative Group. J Am Soc Nephrol. 1999, 10: 1772-1777.
Eugui EM, Mirkovich A, Allison AC: In vitro immunosuppressive effects of mycophenolic acid and an ester pro drug, RS-61443. Transplant Proc. 1991, 23 (suppl 2): 10-14.
Nowack R, Birck R, van der Woude FJ: Mycophenolate mofetil for systemic vasculitis and IgA nephropathy. Lancet. 1997, 349: 774-
Briggs WA, Choi MJ, Scheel Jr PJ: Successful mycophenolate mofetil treatment of glomerular disease. Am J Kidney Dis. 1998, 31: 213-217.
Choi MJ, Eustace JA, Gimenez LF, Atta MG, Scheel PJ, Sothinathan R, Briggs WA: Mycophenolate mofetil treatment for primary glomerular diseases. Kidney Int. 1114, 61: 1098-2002. 10.1046/j.1523-1755.2002.00214.x.
Rodicio JL, Alcazar JM, Ruilope LM: Influence of converting enzyme inhibition on glomerular filtration rate and proteinuria. Kidney Int. 1990, 38: 590-594.
Heeg JA, de Jong PE, van der Hem GK, de Zeeuw D: Reduction of proteinuria by angiotensin converting enzyme inhibition. Kidney Int. 1987, 32: 78-84.
Remuzzi A, Perico N, Sangalli F, Vendramin G, Moriggi M, Ruggenenti P, Remuzzi G: ACE inhibition and ANG II receptor blockade improve glomerular size-selectivity in IgA nephropathy. Am J Physiol. 1999, 276: F457-F466.
K/DOQI Clinical Practice Guidelines for Chronic Kidney Disease: Evaluation, Classification, and Stratification: Guideline 4. Estimation of GFR. Am J Kid Dis. 2002, 39: S76-S92. 10.1053/ajkd.2002.30944.
Bannister KM, Weaver A, Clarkson AR, Woodroffe AJ: lgA Nephropathy: Pathogenesis and treatment. Contrib Nephrol. 1995, 111: 184-193.
Alexopoulos E, Stangou M, Kyrmizis D: The effect of fish-oil in patients with IgA nephropathy and renal function impairment: A prospective study. J Am Soc Nephrol. 2001, 12: 89A-10.1159/000051241.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2369/5/3/prepub
Acknowledgements
C. Martin Bunke, M.D. and Rob Gordon, M.D. of Roche Laboratories, Nutley, NJ provided valuable assistance in the development of this study. The study is supported by grant from Roche Laboratories. The Omacor® capsules are provided by Pronova Biocare, Lysaker, Norway. At the University of Tennessee Health Sciences Center this study is support by the General Clinical Research Center (USPHS-RR000211).
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
Competing interests
None declared.
Ronald J Hogg and Robert J Wyatt contributed equally to this work.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Hogg, R.J., Wyatt, R.J. & Scientific Planning Committee of the North American IgA Nephropathy Study. A randomized controlled trial of mycophenolate mofetil in patients with IgA nephropathy [ISRCTN62574616]. BMC Nephrol 5, 3 (2004). https://doi.org/10.1186/1471-2369-5-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2369-5-3