
Abstract
Background
Transforming growth factor beta 1 (TGF-β1) gene play an important role in the acute myocardial infarction (AMI), however no investigation has been conducted so far in young AMI patients.
In this study, we evaluated the influence of TGF-β1 polymorphisms/haplotypes on the onset and progression of AMI in young Italian population.
Methods
201 cases and 201 controls were genotyped for three TGF-β1 polymorphisms (G-800A, C-509T and Leu10Pro). The main follow-up end-points (mean follow-up, 107 ± 49 months) were death, myocardial infarction or revascularization procedures.
Results
Significant risk factors were smoking (p < 10-4), family history for coronary artery disease (p < 10-4), hypercholesterolemia (p = 0.001) and hypertension (p = 0.002). The C-509T and Leu10Pro polymorphisms showed significant differences (p = 0.026 and p = 0.004) between cases and controls.
The most common haplotypes revealed a possible protective effect (GCT, OR 0.75, 95% CI 0.57–0.99, p = 0.042) and an increased risk of AMI (GTC, OR 1.51, 95% CI 1.13–2.02, p = 0.005), respectively.
No statistical differences were observed in genotype distribution in the follow-up study between the two groups: 61 patients with subsequent events (13 deaths) and 108 without events.
Conclusion
Even though our results need to be further confirmed in larger studies, this is the first study reporting on a possible role of TGFβ1 common haplotypes in the onset of AMI in young patients.
Similar content being viewed by others


Background
AMI at young age (< 45 years) is a multifaceted disorder characterized by low mortality rates, less extensive coronary artery disease (CAD), good residual left ventricular function, and a favourable prognosis [1]. In addition, young patients show lower occurrence of diabetes and hypertension, but in contrast family history of CAD, hypercholesterolemia, and smoking are more frequent [2].
Genes regulating vascular function, lipid metabolism, coagulation, fibrinolysis and inflammation factors have been only partially investigated in AMI at young age, reporting controversial results [3]. Some polymorphisms in prothrombin gene seem to be associated with increased risk of AMI at young age and Factor VII Leiden polymorphisms seem to be protective, whereas contrasting results have been reported for the polymorphism G894T in the nitric oxide synthase (eNOS) gene and polymorphism C677T in the 5,10-methylenetetrahydrofolate reductase (MTHFR) gene.
A recent promising trend of research was the study of genes involved in inflammatory response related to CAD and atherosclerosis [4]. However, the role of TGF-β1 genetic variants in the occurrence of AMI at young age was not investigated so far.
TGF-β1 is a cytokine expressed by a broad variety of cells, including platelets, connective, haematopoietic and endothelial tissue cells [5]. TGF-β1 is the most abundant isoform of the TGFβ family, and it is a multifunctional cytokine regulating cell growth, differentiation and matrix production [6]. TGF-β1 has been found to enhance the expression of mRNA encoding endothelin in vascular endothelial cells [7] and the synthesis of extracellular matrix components such as collagen, fibronectin, and proteoglycan [8].
Recent evidence suggests that pathological misregulation of the transforming growth factor-β (TGF-β) pathway could be implicated in the development of several major diseases, including myocardial infarction [9], fibrotic disease [10], and inflammation processes [4]. In particular, higher levels of serum or plasma TGF-β1 have been observed in subjects with hypertension, in association with cardiac and renal disease [11, 12] or in dilated cardiomyopathy [13], both exacerbated by smoke, although leading to conflicting conclusions.
Even if a clear causative role of TGF-β1 was not demonstrated, changes in the structure and activity of TGF-β1, caused by genetic variants, could influence the biologic processes involving the protein.
We selected three TGF-β1 variants, two of them (G-800A and C-509T) being in the promoter region, near to the consensus DR1 or DR5 nuclear hormone receptor binding sites, crucial for influencing the TGF-β1 synthesis. The third selected polymorphism Leu10Pro (T > C transition) is located into the peptide signal sequence and could interfere with its activity by influencing the transport of the preprotein to the endoplasmic reticulum [14].
In the present study we evaluated the potential role of the above genetic variants in the occurrence and the prognosis of AMI at young age.
Methods
Patients and controls
The sample of cases was composed by 201 patients (age 40 ± 4 years), who satisfied the World Health Organization criteria for the diagnosis of myocardial infarction [15], and who were consecutively admitted between 1992 and 2005 to the Coronary Care Unit of the University Cardiology Division of St. Giovanni Battista Hospital of Turin [16].
The 201 patients were matched with healthy control subjects, recruited by General Practitioners, by sex, diabetes status and age (± 1 year). The study complies with the Declaration of Helsinki and was approved by the Inter-hospital Ethical Board, San Giovanni Battista/C.T.O./C.R.F./Maria Adelaide hospitals (President of the Ethical Board Prof. Alessandro Pileri). The subjects gave informed consent and no sex-based or ethnic-based differences were present, although most of them are of Caucasoid origins.
Information on the following conventional risk factors were collected: age, sex, body mass index, smoking habits, history of hypercholesterolemia (total cholesterol levels > 220 mg/dl or use of hypocholesterolemic drugs), diabetes status, hypertension treatment [17], personal and family history of CAD.
A positive family history was considered if the patient had a first-degree relative with CAD at the age of ≤ 55 years for men or at ≤ 65 years for women.
Patients with ascertained congenital hypercoagulable status, with a proved disease limiting life expectance or with declared cocaine abuse were excluded. Control subjects with CAD and any neoplasm, cardiomyopathy or severe illness limiting life expectance or refusing consent were excluded.
Follow-up (mean 107 ± 49 months) was possible until 2005 for 169 cases (84% of the initial population study), and was performed investigating new hospital admissions, performing telephone interview of patients and periodic ambulatory visits.
Endpoint events considered were death, new myocardial infarction and revascularization procedure (angioplasty or coronary artery bypass graft surgery) that occurred after discharge from the index event.
Laboratory analyses
Blood samples were collected ≥ 6 hours after fasting and 3 months after the index AMI event to avoid influence of acute event on lipid parameters. Total cholesterol, triglycerides, high-density lipoprotein and low-density lipoprotein cholesterol, apolipoprotein B, and apolipoprotein A1 were measured by conventional methods of clinical chemistry.
Genomic DNA was extracted from 200 μl of peripheral blood lymphocytes according to a standard salting-out method [18]. For the 3 polymorphisms, DNA were amplified by Polymerase Chain Reaction and digested with specific restriction endonucleases, as previously reported [19].
Statistical analysis
We calculated allele and genotype frequencies of the G-800A, C-509T and Leu10Pro polymorphisms by direct gene counting; the chi-square statistics was used to test for Hardy-Weinberg equilibrium.
Haplotype reconstruction and their frequencies were estimated from genotypes data by using a Bayesian statistical method based on the coalescence theory, implemented in the PHASE package version 2.0 (default settings were used).
Linkage disequilibrium parameters (D' and r2 statistics) were calculated by the Haploview version 3.31 software.
A Pearson chi square test or Fisher exact test when appropriate (a P value ≤ 0.05 was considered significant) were performed to compare the distribution of the patients and control for each polymorphism and for each risk factor, both in the acute and follow-up study.
A logistic regression analysis was performed to calculate Odds Ratio (OR) and 95% Confidence Intervals (95% CI), and adjusting genetic risks for smoking habits, family history, hypercholesterolemia and hypertension. With 201 cases and 201 controls, a power of 80% and α = 0.05 we are able to detect an increase in OR = 1.7–2.24 depending on the allele frequencies of the three polymorphisms.
Cox regression was also performed for the follow-up analysis taking into account the time variable. All the analyses were performed by the statistical package SPSS v.13.0.
Results
Prevalence of classical risk factors among cases and controls are reported in Table 1.
We have found a statistically significant difference between cases and controls for smoking (79.1% in cases vs 59.7% in controls, p < 10-4) and familial history of CAD (62.3% vs 20.2%, p < 10-4). Significant differences were observed also for hypertension (33.9% vs 16.3%, p = 0.002) and for hypercolesterolemia (54.9% vs 35.7%, p = 0.001).
We genotyped three TGF-β1 polymorphisms in 201 young patients with diagnosed AMI and 201 matched controls (mean age 40 ± 4 years, range 25–45 years). All the polymorphisms were in Hardy-Weinberg equilibrium.
No statistical difference has been observed in the distribution of conventional risk factors by stratifying cases and controls for genotypes (data not shown).
The genotype frequencies (Table 2) appeared significantly different between cases and controls for Leu10Pro (3 × 2 contingency table, p = 0.005), with a significant increased risk as crude Odds Ratios for the CC vs TT genotype (OR 2.35, 95% CI 1.34–4.12, p = 0.003).
A borderline significance has been observed for C-509T polymorphism (3 × 2 contingency table, p = 0.06), with an interesting increased risk for the TT genotype vs the wild-type CC homozygotes (OR 1.93, 95% CI 1.10–3.41, p = 0.02). However, after Bonferroni correction only Leu10Pro was still significant.
After adjusting for smoking habits, family history, hypercholesterolemia and hypertension, results for C-509T and Leu10Pro polymorphisms were no more significant (Table 2).
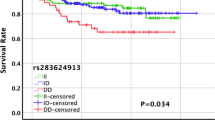
No significant association has been observed for the three TGF-β1 genotypes (Table 3) and for haplotypes (not shown) in the follow-up analysis between the group of 61 patients with a second event after AMI and 108 patients without other events both at univariate and multivariate analysis.
No statistical significant association has been reported for G-800A (p = 0.57). In fact, LD pairwise comparison showed stronger significant values between C-509T and Leu10Pro markers, but lower LD value between these two single nucleotide polymorphisms and C-800A (C-800A/G-509T = 0.02, G-800A/Leu10Pro = 0.03, C-509T/Leu10Pro = 0.59, LD values referred to r2 statistic).
Haplotypes were reconstructed and the difference in their distribution between case and control groups was investigated (Table 4). A total of seven haplotypes, with two of them being the most prevalent, were estimated in both groups.
Only the two most common haplotypes (GCT and GTC) showed statistical differences between the two groups. The frequency of the GCT haplotype carrying the wild type allele at both C-509T and Leu10Pro polymorphism was higher in the control groups (48.7%) than in cases (41.6%) (OR 0.75, 95% CI 0.57–0.99; p = 0.042). On the contrary, the GTC haplotype, carrying the two variant alleles at the above positions, had a higher frequency in the case group (40.7% vs 31.2% in controls; OR 1.51, 95% CI 1.13–2.02, p = 0.005). Both haplotypes carry the wild-type allele of the G-800A polymorphism.
Out of the 61 patients with subsequent events, we registered 13 deaths. Most of the classical risk factors were not considered in the follow-up study due to the adoption of controlled therapies. Cox regression was also performed in the follow-up phase but no significance was observed (data not shown).
Discussion
To our knowledge, this is the first study investigating the possible involvement of TGF-β1 gene in the occurrence and the prognosis of AMI at young age, although an association has been already described in older patients [9].
TGF-β1 is involved in many biological processes and misregulations in the TGF-β pathways have been investigated in pathologic states such as cardiac hypertrophy [20], atherosclerosis [21] and inflammation processes [4]. Increased TGF-β1 mRNA expression was also observed in human restenotic lesions [22]; on the other hand, it was postulated that increased expression of TGF-β1 at the artery wall level, by inhibition of vascular smooth muscle cells (VSMC), could consequently inhibit the accumulation of lipid in vessel wall [14].
Various TGFβ1 polymorphisms were so far investigated to ascertain their possible involvement in the occurrence of several cardiovascular diseases [23], and they were selected on the basis of their peculiar localization. Even if the relevance of other polymorphisms, as Arg25Pro, has been ascertained in the cardiovascular studies, in our preliminary study we focused only on some of them.
The G-800A variant, occurring at 800 base pairs upstream the 5' principal transcription start site, is located in a crucial consensus CREB half-site [24]; the A allele could inhibit the binding to the transcription factors CRE-BP, which appeared implicated in the regulation of other TGFβ-gene family elements. As the G-800A, so the C-509T variant is a promoter polymorphism, located in a transcription factor consensus binding site; the T allele could affect the TGFβ1 expression levels [14]. Both polymorphisms are situated close to the consensus DR1 or DR5 nuclear hormone receptor binding sites, known as crucial sequences in the regulation of the TGF-β1 synthesis in vitro [24] and in vivo [24].
The coding Leu10Pro polymorphism, located in the codon 10 of the gene, fall in the signal peptide sequence, necessary to address the synthesized protein to the endoplasmic reticulum. In the past years, consistent conclusions deriving from the study of these TGF-β1 variants were produced, even if the results appear controversial.
In a study of Yokota et al. [14] it was reported a correlation of the wild type allele of C-509T with low TGF-β1 plasmatic concentration. According to these results, the T allele of C-509T was found associated with higher circulating TGF-β1 levels [24], often related to hypertension, and in association with cardiac disease [12] or to dilated cardiomyopathy [13]. The C-509T polymorphism (and its haplotypes) was also recently found associated with myocardial infarction in men [9], even after adjustment for smoking habits, age, hypertension, diabetes and hypercholesterolemia. This result is in agreement with a possible described correlation between genetic variants in the inflammatory genes and the risk modulation of ischaemic heart disease [4]. Moreover, the Leu10Pro variant [14] was found in association with myocardial infarction (MI) in Japanese patients (OR = 3.5 p < 0.0001), although a previous European study [25] did not show any association between this polymorphism and MI.
We have found that both C-509T and Leu10Pro polymorphisms could modulate genetic susceptibility to juvenile AMI, whereas no significant differences was observed for G-800A, in agreement with some studies [9, 14], but not with others [25].
Contrasting results could be partly explained by the heterogeneity of the studies, due both to different prevalence of classical risk factors or to different genetic and ethnic backgrounds.
Our results on C-509T and Leu10Pro polymorphisms seem to support the possible relevance of this gene. In fact Leu10Pro does not change the amino-acidic polarity [25], but it is located in a crucial position [14], as above mentioned.
The relevance of C-509T and Leu10Pro is also strengthened by the haplotype results indicating a possible increased risk of AMI conferred by the GTC haplotype and a protective effect of the GCT haplotype. According to these results the putative "protective" haplotype (GCT) carries both the C-509T and Leu10Pro wild type alleles, whereas the putative "predisposing" haplotype GTC carries the mutated alleles. Moreover the two haplotypes were the most common both in cases and in controls, supporting the idea that common variants/haplotypes could be really important in determining common diseases [26]. Although the above described crucial location of the G-800A variant in the genome sequence, we did not observe a significant association between G-800A and AMI.
The lack of significant results for TGF-β1 polymorphisms/haplotypes in the follow-up analysis seems to suggest that different genetic mechanisms could be responsible for the progression of AMI.
Conclusion
In conclusion, although it is clear that AMI is a multifactorial disease due to the combination of many genetic and well known environmental risk factors, this is the first study reporting on a significant association between TGF-β1 polymorphisms/haplotypes and the occurrence of AMI at young age.
Although these results warrant further investigation on larger sample size and in-depth biochemical analysis relating, for example, haplotypes to the TGF-β1 serum levels, they indicate also the need to better clarify the role of TGF-β pathway in AMI.
References
Brscic E, Bergerone S, Gagnor A, Colajanni E, Matullo G, Scaglione L, Cassader M, Gaschino G, Di Leo M, Brusca A, Pagano GF, Piazza A, Trevi GP: Acute myocardial infarction in young adults: prognostic role of angiotensin-converting enzyme, angiotensin II type I receptor, apolipoprotein E, endothelial constitutive nitric oxide synthase, and glycoprotein IIIa genetic polymorphisms at medium-term follow-up. Am Heart J. 2000, 139 (6): 979-984. 10.1067/mhj.2000.106165.
Imazio M, Bobbio M, Bergerone S, Barlera S, Maggioni AP: Clinical and epidemiological characteristics of juvenile myocardial infarction in Italy: the GISSI experience. G Ital Cardiol. 1998, 28 (5): 505-512.
Incalcaterra E, Hoffmann E, Averna MR, Caimi G: Genetic risk factors in myocardial infarction at young age. Minerva Cardioangiol. 2004, 52 (4): 287-312.
Andreotti F, Porto I, Crea F, Maseri A: Inflammatory gene polymorphisms and ischaemic heart disease: review of population association studies. Heart. 2002, 87 (2): 107-112. 10.1136/heart.87.2.107.
Blobe GC, Schiemann WP, Lodish HF: Role of transforming growth factor beta in human disease. N Engl J Med. 2000, 342 (18): 1350-1358. 10.1056/NEJM200005043421807.
Ignotz RA, Massague J: Transforming growth factor-beta stimulates the expression of fibronectin and collagen and their incorporation into the extracellular matrix. J Biol Chem. 1986, 261 (9): 4337-4345.
Kurihara H, Yoshizumi M, Sugiyama T, Takaku F, Yanagisawa M, Masaki T, Hamaoki M, Kato H, Yazaki Y: Transforming growth factor-beta stimulates the expression of endothelin mRNA by vascular endothelial cells. Biochem Biophys Res Commun. 1989, 159 (3): 1435-1440. 10.1016/0006-291X(89)92270-5.
Border WA, Noble NA: Transforming growth factor beta in tissue fibrosis. N Engl J Med. 1994, 331 (19): 1286-1292. 10.1056/NEJM199411103311907.
Koch W, Hoppmann P, Mueller JC, Schomig A, Kastrati A: Association of transforming growth factor-beta1 gene polymorphisms with myocardial infarction in patients with angiographically proven coronary heart disease. Arterioscler Thromb Vasc Biol. 2006, 26 (5): 1114-1119. 10.1161/01.ATV.0000217747.66517.11.
Chen Y, Shi-Wen X, van Beek J, Kennedy L, McLeod M, Renzoni EA, Bou-Gharios G, Wilcox-Adelman S, Goetinck PF, Eastwood M, Black CM, Abraham DJ, Leask A: Matrix contraction by dermal fibroblasts requires transforming growth factor-beta/activin-linked kinase 5, heparan sulfate-containing proteoglycans, and MEK/ERK: insights into pathological scarring in chronic fibrotic disease. Am J Pathol. 2005, 167 (6): 1699-1711.
Peterson MC: Circulating transforming growth factor beta-1: a partial molecular explanation for associations between hypertension, diabetes, obesity, smoking and human disease involving fibrosis. Med Sci Monit. 2005, 11 (7): RA229-32.
Laviades C, Varo N, Diez J: Transforming growth factor beta in hypertensives with cardiorenal damage. Hypertension. 2000, 36 (4): 517-522.
Sanderson JE, Lai KB, Shum IO, Wei S, Chow LT: Transforming growth factor-beta(1) expression in dilated cardiomyopathy. Heart. 2001, 86 (6): 701-708. 10.1136/heart.86.6.701.
Yokota M, Ichihara S, Lin TL, Nakashima N, Yamada Y: Association of a T29-->C polymorphism of the transforming growth factor-beta1 gene with genetic susceptibility to myocardial infarction in Japanese. Circulation. 2000, 101 (24): 2783-2787.
WHO: Nomenclature and criteria for diagnosis of ischemic heart disease. Report of the Joint International Society and Federation of Cardiology/World Health Organization task force on standardization of clinical nomenclature. Circulation. 1979, 59 (3): 607-609.
Franco E, Palumbo L, Crobu F, Anselmino M, Frea S, Matullo G, Piazza A, Trevi GP, Bergerone S: Renin-angiotensin-aldosterone system polymorphisms: a role or a hole in occurrence and long-term prognosis of acute myocardial infarction at young age. BMC Med Genet. 2007, 8: 27-10.1186/1471-2350-8-27.
The fifth report of the Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure (JNC V). Arch Intern Med. 1993, 153 (2): 154-183. 10.1001/archinte.153.2.154.
Miller SA, Dykes DD, Polesky HF: A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acids Res. 1988, 16 (3): 1215-10.1093/nar/16.3.1215.
Carturan S, Roccatello D, Menegatti E, Di Simone D, Davit A, Piazza A, Sena LM, Matullo G: Association between transforming growth factor beta1 gene polymorphisms and IgA nephropathy. J Nephrol. 2004, 17 (6): 786-793.
He ZY, Feng B, Yang SL, Luo HL: Intracardiac basic fibroblast growth factor and transforming growth factor-beta 1 mRNA and their proteins expression level in patients with pressure or volume-overload right or left ventricular hypertrophy. Acta Cardiol. 2005, 60 (1): 21-25. 10.2143/AC.60.1.2005044.
Agrotis A, Kalinina N, Bobik A: Transforming growth factor-beta, cell signaling and cardiovascular disorders. Curr Vasc Pharmacol. 2005, 3 (1): 55-61. 10.2174/1570161052773951.
Nikol S, Isner JM, Pickering JG, Kearney M, Leclerc G, Weir L: Expression of transforming growth factor-beta 1 is increased in human vascular restenosis lesions. J Clin Invest. 1992, 90 (4): 1582-1592. 10.1172/JCI116027.
Syrris P, Carter ND, Metcalfe JC, Kemp PR, Grainger DJ, Kaski JC, Crossman DC, Francis SE, Gunn J, Jeffery S, Heathcote K: Transforming growth factor-beta1 gene polymorphisms and coronary artery disease. Clin Sci (Lond). 1998, 95 (6): 659-667.
Grainger DJ, Heathcote K, Chiano M, Snieder H, Kemp PR, Metcalfe JC, Carter ND, Spector TD: Genetic control of the circulating concentration of transforming growth factor type beta1. Hum Mol Genet. 1999, 8 (1): 93-97. 10.1093/hmg/8.1.93.
Cambien F, Ricard S, Troesch A, Mallet C, Generenaz L, Evans A, Arveiler D, Luc G, Ruidavets JB, Poirier O: Polymorphisms of the transforming growth factor-beta 1 gene in relation to myocardial infarction and blood pressure. The Etude Cas-Temoin de l'Infarctus du Myocarde (ECTIM) Study. Hypertension. 1996, 28 (5): 881-887.
Zwick ME, Cutler DJ, Chakravarti A: Patterns of genetic variation in Mendelian and complex traits. Annu Rev Genomics Hum Genet. 2000, 1: 387-407. 10.1146/annurev.genom.1.1.387.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2350/9/13/prepub
Acknowledgements
This work has been partially supported in the framework of a Contract by the European Commission (QLRT-2000-00916). The authors acknowledge all the volunteers who participated in this study as blood donors.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The author(s) declare that they have no competing interests.
Authors' contributions
FC participated in the design of the study, carried out the molecular genetic studies, participated in the statistical analysis, drafted and revised the manuscript; LP partecipated in the design of the study, in the clinical evaluation and selection of patients, in the follow-up interviews, in the selection of healthy controls, revised the maniscript; EF partecipated in the design of the study, in the clinical evaluation and selection of patients, in the follow-up interviews, revised the maniscript; SB partecipated in the clinical evaluation of patients, in the follow-up interviews, revised the manuscript; SC participated in molecular genetic studies and revised the manuscript; SG molecular genetic studies and revised the manuscript; SF partecipated in the clinical evaluation of patients, in the follow-up interviews; GPT partecipated in the clinical evaluation of patients, revised the manuscript; AP partecipated in the design of the study, revised the manuscript; GM partecipated in the design of the study, in the statistical analysis, revised the manuscript.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Crobu, F., Palumbo, L., Franco, E. et al. Role of TGF-β1 haplotypes in the occurrence of myocardial infarction in young Italian patients. BMC Med Genet 9, 13 (2008). https://doi.org/10.1186/1471-2350-9-13
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2350-9-13