
Abstract
Background
Breast and prostate cancer are two commonly diagnosed cancers in the United States. Prior work suggests that cancer causing genes and cancer susceptibility genes can be identified.
Methods
We conducted a genome-wide association study (Affymetrix 100K SNP GeneChip) of cancer in the community-based Framingham Heart Study. We report on 2 cancer traits – prostate cancer and breast cancer – in up to 1335 participants from 330 families (54% women, mean entry age 33 years). Multivariable-adjusted residuals, computed using Cox proportional hazards models, were tested for association with qualifying SNPs (70, 987 autosomal SNPs with genotypic call rate ≥80%, minor allele frequency ≥10%, Hardy-Weinberg test p ≥ 0.001) using generalized estimating equations (GEE) models and family based association tests (FBAT).
Results
There were 58 women with breast cancer and 59 men with prostate cancer. No SNP associations attained genome-wide significance. The top SNP associations in GEE models for each trait were as follows: breast cancer, rs2075555, p = 8.0 × 10-8 in COL1A1; and prostate cancer, rs9311171, p = 1.75 × 10-6 in CTDSPL. In analysis of selected candidate cancer susceptibility genes, two MSR1 SNPs (rs9325782, GEE p = 0.008 and rs2410373, FBAT p = 0.021) were associated with prostate cancer and three ERBB4 SNPs (rs905883 GEE p = 0.0002, rs7564590 GEE p = 0.003, rs7558615 GEE p = 0.0078) were associated with breast cancer. The previously reported risk SNP for prostate cancer, rs1447295, was not included on the 100K chip. Results of cancer phenotype-genotype associations for all autosomal SNPs are web posted at http://www.ncbi.nlm.nih.gov/projects/gap/cgi-bin/study.cgi?id=phs000007.
Conclusion
Although no association attained genome-wide significance, several interesting associations emerged for breast and prostate cancer. These findings can serve as a resource for replication in other populations to identify novel biologic pathways contributing to cancer susceptibility.
Similar content being viewed by others

Background
Breast and prostate cancer are the most frequently diagnosed cancers in women and men respectively with over 200,000 cases each of new breast and prostate cancer estimated for 2006 in the United States [1]. Furthermore, prostate cancer is the second leading cause of cancer-related deaths in men and breast cancer is the second leading cause of cancer-related deaths in women. Family history is a well established risk factor for both breast and prostate cancer providing evidence for underlying genetic factors contributing to cancer occurrence. Accumulating research has identified a number of candidate genes and biologic pathways associated with increased susceptibility to cancer. However, even the most penetrant mutations, such as in BRCA1 and BRCA2, account for only 5–10% of cases and are present in <1% of the general population. Genome-wide association studies (GWAS) provide a comprehensive approach to identification of genetic variants associated with cancer risk unconstrained by existing knowledge and may permit detection of common genetic variants each with small associated cancer risk but great public health impact. Reports from two recent GWAS demonstrated the importance of this approach with the discovery of novel loci for breast cancer susceptibility [2, 3]. Four SNPs in the FGFR2 gene were strongly associated with breast cancer and the association was confirmed in a sample of cases and controls derived from three additional studies [3].
We used the Framingham Heart Study (FHS) Affymetrix 100K SNP genotyping resource for GWAS of breast and prostate cancer phenotypes. The FHS offers the advantage of a prospective longitudinal family-based community sample with participants who have been well-characterized throughout adulthood with respect to risk factors and diseases, including cancer. We report results of two complementary strategies to identify genome-wide associations with cancer phenotypes: 1) a simple low p-value SNP ranking strategy; and 2) 100K SNP associations within candidate genes and regions previously reported to be associated with these cancers in humans.
Methods
Study sample
The genotyped study sample comprised 1345 Original cohort (n = 258) and Offspring (n = 1087) participants from the 330 largest FHS families. The Overview [4] provides further details of this sample. There were 250 participants in the sample with cancer (excluding non-melanoma skin cancer) including 58 women with breast cancer, and 59 men with prostate cancer. The Boston University Medical Center Institutional Review Board approved the examination content of Original Cohort and Offspring examinations. All participants provided written informed consent including consent for genetic studies.
Cancer phenotype definitions and residual creation
The 5209 Original Cohort participants have been examined biennially since study inception in 1948 and the 5124 Offspring Cohort participants (children of the Original Cohort and spouses of the children) have been examined approximately every 4 years since enrollment in 1971. Cancer cases were identified at routine examinations or by health-history updates for participants who did not attend an examination. Medical records were reviewed by two independent reviewers (BEK, GLS). The vast majority of cancers were confirmed by pathology reports; <3.4% of cancer cases were based on death certificate or clinical diagnosis alone. The 1976 World Health Organization ICD-O coding was used to classify all primary cancers. Hence, topography, location (subdivision of site), histology or morphology (cell histopathology), behavior (degree of malignancy), and grade (histological grading & differentiation) were recorded along with date of diagnosis. Cancer cases reviewed through December 31, 2005 were included in this study. The proportion of women and men in the study sample with breast (8%) and prostate cancer (9%) respectively was similar to that in the full FHS sample.
Cox proportional hazards models were used to generate martingale residuals using the PHREG procedure in SAS to perform the regression analysis of time from study entry to cancer diagnosis or last contact free of cancer. Breast cancer was examined in women only and models were cohort-specific and adjusted for 1) age at entry and 2) age, parity, and body mass index at study entry. For prostate cancer, in men only, models were cohort-specific and adjusted for age at entry.
Genotyping
Affymetrix 100K SNP GeneChip genotyping and the Marshfield STR genotyping performed by the Mammalian Genotyping Service http://research.marshfieldclinic.org/genetics are described in the Overview [4]. SNPs were excluded if minor allele frequency <0.10 (n = 38062); genotypic call rate <0.80 (n = 2346); Hardy Weinberg equilibrium test p < 0.001 (n = 1595). There were 70,987 autosomal SNPs available for analysis after the exclusions.
Statistical Analysis
The statistical methods for genome-wide association analyses are described in detail in the Overview [4]. While there are various suggested methods for interpretation of genome-wide significance, we chose to use a conservative (p < 0.05/10-6 = 5 × 10-8) threshold to define genome-wide significance for this report.
Association
All cancer residual traits listed in Table 1 were computed using Cox proportional hazards models. The full set of FHS participants with the phenotype were used to create the residuals. The residuals were used to test for association between the genotyped subset of participants and the SNPs using family-based association test (FBAT) and generalized estimating equation (GEE) models. FBAT analyses were restricted to at least 10 informative families. The GEE tests tended to give an excess of very small p-values over what would be expected (see Overview [4]).
SNP prioritization
We used several strategies to prioritize SNPs associated with cancer traits. First, we used an untargeted approach whereby SNP associations were ranked according to the strength of the p-value for each trait. Next we identified candidate genes reported to be associated with each cancer trait from review of the literature. Candidate genes were selected by searching PubMed (using susceptibility, gene, cancer and (breast or prostate) as keywords, last accessed 08-15-06), and the Entrez Gene and Online Mendelian Inheritance in Man resources, as well as recent text books. All available 100K SNPs in or near the a priori selected candidate genes were investigated for association with cancer traits. Finally for prostate cancer, we also examined SNP associations in the region on chromosome 8 (8q24) previously reported to be associated with prostate cancer in Icelandic families and confirmed in three case-control series [5] and African American men [6]. Further, for prostate cancer we examined the overlap in SNP associations in our study and the top 500 ranked SNPs from the Cancer Genetics Markers of Susceptibility (CGEMS) project sponsored by the National Cancer Institute. Because CGEMS used an Illumina platform for genotyping and the genotyping used in this study was performed with an Affymetrix platform, the gene_symbol from the UCSC annotation was used to link with CGEMS top 500 SNP list. Using this method, 1487 SNPs in FHS 100K (including SNPs with MAF < 0.1) correlated with the CGEMS top 500 SNPs related to a known gene.
SNPs were annotated with the UCSC genome browser tables using the May 2004 assembly http://genome.ucsc.edu/[7, 8]. All genes within 60 kb of the top ranked SNPs were identified. The physical location of the SNPs was based on Build 35 of Genome for this report; however, the 100K web browser was based on Build 36.
Results
The cancer phenotypes available in the FHS 100K SNP resource, including details of the sample size, number of cancer events, and covariate adjustment for each trait are listed in Table 1. In this report, we consider only two phenotypes: breast cancer in women (multivariable-adjusted) and prostate cancer in men. Among participants in the 100K sample the mean age at breast cancer diagnosis was 59 years (range 35 to 83 years) in Offspring Cohort women and 70 years (range 35 to 97 years) in Original Cohort women; the mean age at prostate cancer diagnosis was 66 years (range 43 to 85 years) in Offspring Cohort men and 76 years (range 53 to 95 years) in Original Cohort men.
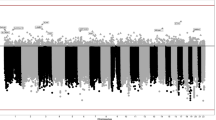
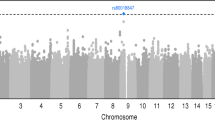
For each of the cancer phenotypes, Table 2 provides the top 15 SNPs ranked in order by lowest p-value for the GEE models and for the FBAT models (all SNP associations can be viewed on the web) [9]. None of the SNP associations achieved genome-wide significance (p < 5 × 10-8) [4]. However, for prostate cancer, the top SNP in GEE models, rs9311171, is in CTDSPL (CTD {carboxy-terminal domain, RNA polymerase II, polypeptide A} small phosphatase-like), a gene that may play a role in tumor suppression [10].
There were several additional associations not listed in Table 2 that were of interest. For prostate cancer, in GEE models rs906304 (rank 27, p = 0.000067), is in NCOR2 also known as SMRT. SMRT levels have been reported to be elevated in prostate cancer cells, and result in suppression of anti-proliferative target gene actions for the vitamin D receptor [11, 12]. In FBAT models, for prostate cancer SNP rs255561 (rank 17, p = 0.00039), is near XRCC4, a gene that plays a role in DNA repair and rs1897676 (rank 50, p = 0.0012), is in PTPRD. Protein tyrosine phosphatases are signaling molecules involved in the regulation of a variety of cellular processes including cell growth, differentiation, mitotic cycle, and oncogenic transformation [13]. For breast cancer in GEE models rs4146372 (rank 31, p = 0.00007), is near RAB21, SNP rs9307561 (rank 40, p = 0.0001), is near FAT4, and rs10512849 (rank 46, p = 0.00014), is in FGF10. These genes appear to play biologic roles in a variety of processes including tumor growth and suppression [13, 14]. In FBAT models, for breast cancer rs2836391 (rank 46, p = 0.0012), is in ERG, an oncogene important in the development of prostate cancer [15, 16].
Our second strategy was to identify from the literature candidate genes implicated in breast and prostate cancer susceptibility (see Additional data file 1). For prostate cancer, we identified 63 candidate genes. Twenty of these candidate genes had from 1 to 20 SNPs on the 100K chip whereas the remaining genes had no SNP coverage on the chip. For breast cancer, 75 potential candidate genes were identified, 28 of these genes had between 1 and 35 SNPs on the 100K chip and the remaining candidate genes were not covered on the chip. Two SNPs in MSR1 (rs9325782, GEE p = 0.008 and rs2410373, FBAT p = 0.021) were associated with prostate cancer and three SNPs in ERBB4 (rs905883 GEE p = 0.0002, rs7564590 GEE p = 0.003, rs7558615 GEE p = 0.0078) were associated with breast cancer (Table 3). For prostate cancer, a region on chromosome 8q24 was recently reported to be associated with prostate cancer risk in Icelandic men and confirmed in three case-control series of men of European ancestry and African American men [5, 6]. There were a total of 64 SNPs on the 100K chip in this 8q24 region (128 to 129.3 Mb interval). However, the reported risk SNP, rs1447295, was not included on the 100K chip and none of the 64 available SNPs were in linkage disequilibrium with the risk SNP. Five other SNPs in this region were associated with prostate cancer with a GEE or FBAT p-value < 0.01 (Table 4).
The National Cancer Institute commenced the CGEMS [17] initiative to conduct genome-wide association studies to identify genetic factors related to prostate and breast cancer. We examined overlap between the top 500 ranked SNPs for prostate cancer in CGEMS phase 1a [18] and the results of the FHS 100K GWAS analysis for prostate cancer. The physical position of the SNP was used to detect overlapping associations and the results are shown in Table 5. Of note, many of the associations in Table 5 are in SNPs with very low minor allele frequencies and the results are presented according to minor allele frequency. WWOX gene, a tumor suppressor gene, that has been reported to play a role in prostate cancer [19], showed evidence of association (rs3751832, p = 0.0009) in our study sample.
Discussion
Breast and prostate cancer are the two most frequently diagnosed cancers in the United States and result in substantial morbidity and mortality [1]. A number of breast and prostate cancer susceptibility genes and chromosomal regions have been identified [2, 3, 5, 20–34]. However, currently known genes account for only a fraction of the familial aggregation of breast cancer [25] and few prostate cancer susceptibility genes have even been identified. Risk for these cancers is likely mediated through variation in many genes, each conferring a relatively small risk for the disease. Genome-wide association studies provide an opportunity to discover novel genes and pathways that play a causal role in cancer occurrence and in turn may lead to new therapies for the prevention and treatment of cancer. Finding genetic associations with breast and prostate cancer risk that are robust across multiple studies may facilitate the identification of high risk individuals who can be targeted for early screening and preventive interventions.
We report GWAS results for breast cancer and prostate cancer phenotypes in a community-based sample of adults from two generations of the same families. Although none of the SNP associations achieved genome-wide significance in GEE or FBAT models, this resource has the potential to detect novel cancer susceptibility genes and to explore the relevance of promising candidate gene associations to human cancer. Our results can be compared to those from other genome-wide association studies such as the National Cancer Institute's CGEMS [17]. Although the two studies used different genotyping platforms limiting overlap in the SNPs examined, we were able to determine the physical position of the SNPs. Using this strategy, SNPs in the ERRB4 gene (CGEMS DSSNP_ID rs2371438 and FHS 100K SNP rs10497958) were associated with prostate cancer. ErbB proteins are widely expressed in prostate cells [35] and may play a role in tumor development, growth and progression in human prostate cancer [36, 37]. We also examined the 8q24 region previously associated with prostate cancer risk. CGEMS investigators recently reported a second independent risk SNP (rs6983267) within the 8q24 strongly associated with prostate cancer [34]. The Affymetrix 100K GeneChip did not include either of the previously reported risk SNPs; however, we did identify five other SNPs in this region associated with prostate cancer. The underlying biologic mechanism mediating prostate cancer risk associated with the SNPs and chromosomal region remains unknown. A two-stage approach, genome-wide association followed by selective genotyping of SNPs with suggestive evidence of association, may provide an efficient strategy for pursuing initial genome-wide results [2, 38, 39].
Several important limitations merit comment. First, this study used cancer cases identified through surveillance of a multigenerational community-based sample. The enrollment and examination of Original Cohort and Offspring Cohort participants began years before DNA collection occurred. Thus, a survival bias may have been introduced. Our cases may be comprised of early-staged and less lethal cancers. To address this potential bias, we adjusted for covariates using the full Framingham sample, and used the residual traits for the subset of individuals genotyped using the 100K Affymetrix GeneChip to test for association with the SNPs in linear regression models. Residual traits from Cox models typically are not ideally distributed for linear regression models, but our adjustment method using the full Framingham sample precludes the testing of SNP associations with cancer traits using Cox models. Second, we had a small number of cancer events (250 all cancer cases, 58 breast cancer cases and 59 prostate cancer cases) limiting our ability to detect SNP associations. In a recent small GWAS of age-related macular degeneration that included 96 cases and 50 controls, an association with the CFH gene was identified [40] and confirmed in larger studies [41–43]. However, in that report, individuals homozygous for the CFH risk allele had a sevenfold increased likelihood of age-related macular degeneration [40]. It is very unlikely that common genetic variants for cancer phenotypes will confer a risk for cancer susceptibility of that magnitude. For example, the odds ratio associated with the risk marker identified for prostate cancer in region 8q24 was 1.72 in the combined Icelandic sample [5]. Furthermore, the associations between prostate cancer and the SNPs with low minor allele frequency (Table 5) are likely to be false positive associations given the small number of prostate cancer cases in our sample. Third, the 100K Affymetrix GeneChip provides limited coverage of the genome; many of our a priori candidate genes did not have any SNP coverage on the chip and coverage of some candidate genes that were present on the chip was suboptimal. Importantly, the replicated risk SNP, rs1447295, for prostate cancer [5] was not included on the chip. NHLBI has committed funds for a 550 K genome-wide scan on all FHS participants. This will enable us to confirm our initial 100K SNP associations in a larger sample with a greater number of cancer cases and with denser coverage of the genome. We did not examine epistasis or gene-environment interactions which may modify the associations noted in this study. Lastly, most of our associations are likely to be due to chance. Replication studies are needed to determine if any of the results we report are indicative of true associations. It is important that our data be used in conjunction with data from other samples given the high probability of false positive associations.
Conclusion
In summary, the untargeted genome-wide approach to detect genetic associations for cancer traits provides an opportunity to identify novel biologic pathways related to cancer occurrence and to direct future study of candidate genes that hold the most promise for relevance to cancer risk in humans. Enhancing our understanding of the mechanisms responsible for cancer susceptibility may in turn identify novel strategies for early detection, prevention, and treatment of breast and prostate cancers. These data serve as a resource for replication in other population-based samples.
Abbreviations
- CGEMS:
-
cancer genetics markers of susceptibility
- FBAT:
-
family-based association test
- FHS:
-
Framingham Heart Study
- GEE:
-
generalized estimating equations
- GWAS:
-
genome-wide association study
- ICD-O:
-
international classification of diseases for oncology
- MAF:
-
minor allele frequency
- SNP:
-
single nucleotide polymorphism.
References
American Cancer Society: Cancer Facts and Figures 2006. 2006, Atlanta: American Cancer Society
Easton DF, Pooley KA, Dunning AM, Pharoah PD, Thompson D, Ballinger DG, Struewing JP, Morrison J, Field H, Luben R, Wareham N, Ahmed S, Healey CS, Bowman R, Luccarini C, Conroy D, Shah M, Munday H, Jordan C, Perkins B, West J, Redman K, Meyer KB, Haiman CA, Kolonel LK, Henderson BE, Le Marchand L, Brennan P, Sangrajrang S, Gaborieau V, Odefrey F, Shen CY, Wu PE, Wang HC, Eccles D, Evans DG, Peto J, Fletcher O, Johnson N, Seal S, Stratton MR, Rahman N, Chenevix-Trench G, Bojesen SE, Nordestgaard BG, Axelsson CK, Garcia-Closas M, Brinton L, Chanock S, Lissowska J, Peplonska B, Nevanlinna H, Fagerholm R, Eerola H, Kang D, Yoo KY, Noh DY, Ahn SH, Hunter DJ, Hankinson SE, Cox DG, Hall P, Wedren S, Liu J, Low YL, Bogdanova N, Schurmann P, Dork T, Tollenaar RA, Jacobi CE, Devilee P, Klijn JG, Sigurdson AJ, Doody MM, Alexander BH, Zhang J, Cox A, Brock IW, Macpherson G, Reed MW, Couch FJ, Goode EL, Olson JE, Meijers-Heijboer H, van den OA, Uitterlinden A, Rivadeneira F, Milne RL, Ribas G, Gonzalez-Neira A, Benitez J, Hopper JL, McCredie M, Southey M, Giles GG, Schroen C, Justenhoven C, Brauch H, Hamann U, Ko YD, Spurdle AB, Beesley J, Chen X, Aghmesheh M, Amor D, Andrews L, Antill Y, Armes J, Armitage S, Arnold L, Balleine R, Begley G, Beilby J, Bennett I, Bennett B, Berry G, Blackburn A, Brennan M, Brown M, Buckley M, Burke J, Butow P, Byron K, Callen D, Campbell I, Chenevix-Trench G, Clarke C, Colley A, Cotton D, Cui J, Culling B, Cummings M, Dawson SJ, Dixon J, Dobrovic A, Dudding T, Edkins T, Eisenbruch M, Farshid G, Fawcett S, Field M, Firgaira F, Fleming J, Forbes J, Friedlander M, Gaff C, Gardner M, Gattas M, George P, Giles G, Gill G, Goldblatt J, Greening S, Grist S, Haan E, Harris M, Hart S, Hayward N, Hopper J, Humphrey E, Jenkins M, Jones A, Kefford R, Kirk J, Kollias J, Kovalenko S, Lakhani S, Leary J, Lim J, Lindeman G, Lipton L, Lobb L, Maclurcan M, Mann G, Marsh D, McCredie M, McKay M, Anne MS, Meiser B, Milne R, Mitchell G, Newman B, O'loughlin I, Osborne R, Peters L, Phillips K, Price M, Reeve J, Reeve T, Richards R, Rinehart G, Robinson B, Rudzki B, Salisbury E, Sambrook J, Saunders C, Scott C, Scott E, Scott R, Seshadri R, Shelling A, Southey M, Spurdle A, Suthers G, Taylor D, Tennant C, Thorne H, Townshend S, Tucker K, Tyler J, Venter D, Visvader J, Walpole I, Ward R, Waring P, Warner B, Warren G, Watson E, Williams R, Wilson J, Winship I, Young MA, Bowtell D, Green A, Defazio A, Chenevix-Trench G, Gertig D, Webb P, Mannermaa A, Kosma VM, Kataja V, Hartikainen J, Day NE, Cox DR, Ponder BA: Genome-wide association study identifies novel breast cancer susceptibility loci. Nature. 2007.
Hunter DJ, Kraft P, Jacobs KB, Cox DG, Yeager M, Hankinson SE, Wacholder S, Wang Z, Welch R, Hutchinson A, Wang J, Yu K, Chatterjee N, Orr N, Willett WC, Colditz GA, Ziegler RG, Berg CD, Buys SS, McCarty CA, Feigelson HS, Calle EE, Thun MJ, Hayes RB, Tucker M, Gerhard DS, Fraumeni JF, Hoover RN, Thomas G, Chanock SJ: A genome-wide association study identifies alleles in FGFR2 associated with risk of sporadic postmenopausal breast cancer. Nat Genet. 2007.
Cupples LA, Arruda H, Benjamin EJ, D'Agostino RB, Demissie S, DeStefano AL, Dupuis J, Falls K, Fox CS, Gottlieb D, Govindaraju DR, Guo CY, Heard-Costa N, Hwang SJ, Katherisan S, Kiel D, Laramie JM, Larson MG, Levy D, Liu CY, Lunetta KL, Mailman M, Manning AK, Meigs JB, Murabito JM, Newton-Cheh C, O'Connor GT, O'Donnell CJ, Pandey MA, Seshadri S, Vasan RS, Wang ZY, Wilk JB, Wolf PA, Yang Q, Atwood LD: The Framingham Heart Study 100K SNP genome-wide association study resource: Overview of 17 phenotype working group reports. BMC Med Genet. 2007, 8 (Suppl 1): S1-
Amundadottir LT, Sulem P, Gudmundsson J, Helgason A, Baker A, Agnarsson BA, Sigurdsson A, Benediktsdottir KR, Cazier JB, Sainz J, Jakobsdottir M, Kostic J, Magnusdottir DN, Ghosh S, Agnarsson K, Birgisdottir B, Le Roux L, Olafsdottir A, Blondal T, Andresdottir M, Gretarsdottir OS, Bergthorsson JT, Gudbjartsson D, Gylfason A, Thorleifsson G, Manolescu A, Kristjansson K, Geirsson G, Isaksson H, Douglas J, Johansson JE, Balter K, Wiklund F, Montie JE, Yu X, Suarez BK, Ober C, Cooney KA, Gronberg H, Catalona WJ, Einarsson GV, Barkardottir RB, Gulcher JR, Kong A, Thorsteinsdottir U, Stefansson K: A common variant associated with prostate cancer in European and African populations. Nat Genet. 2006, 38: 652-658. 10.1038/ng1808.
Freedman ML, Haiman CA, Patterson N, McDonald GJ, Tandon A, Waliszewska A, Penney K, Steen RG, Ardlie K, John EM, Oakley-Girvan I, Whittemore AS, Cooney KA, Ingles SA, Altshuler D, Henderson BE, Reich D: Admixture mapping identifies 8q24 as a prostate cancer risk locus in African-American men. Proc Natl Acad Sci USA. 2006, 103: 14068-14073. 10.1073/pnas.0605832103.
Karolchik D, Baertsch R, Diekhans M, Furey TS, Hinrichs A, Lu YT, Roskin KM, Schwartz M, Sugnet CW, Thomas DJ, Weber RJ, Haussler D, Kent WJ: The UCSC Genome Browser Database. Nucleic Acids Res. 2003, 31: 51-54. 10.1093/nar/gkg129.
Kent WJ, Sugnet CW, Furey TS, Roskin KM, Pringle TH, Zahler AM, Haussler D: The human genome browser at UCSC. Genome Res. 2002, 12: 996-1006. 10.1101/gr.229102. Article published online before print in May 2002.
2007, [http://www.ncbi.nlm.nih.gov/projects/gap/cgi-bin/study.cgi?id=phs000007]
Kashuba VI, Li J, Wang F, Senchenko VN, Protopopov A, Malyukova A, Kutsenko AS, Kadyrova E, Zabarovska VI, Muravenko OV, Zelenin AV, Kisselev LL, Kuzmin I, Minna JD, Winberg G, Ernberg I, Braga E, Lerman MI, Klein G, Zabarovsky ER: RBSP3 (HYA22) is a tumor suppressor gene implicated in major epithelial malignancies. Proc Natl Acad Sci USA. 2004, 101: 4906-4911. 10.1073/pnas.0401238101.
Khanim FL, Gommersall LM, Wood VH, Smith KL, Montalvo L, O'Neill LP, Xu Y, Peehl DM, Stewart PM, Turner BM, Campbell MJ: Altered SMRT levels disrupt vitamin D3 receptor signalling in prostate cancer cells. Oncogene. 2004, 23: 6712-6725. 10.1038/sj.onc.1207772.
Abedin SA, Banwell CM, Colston KW, Carlberg C, Campbell MJ: Epigenetic corruption of VDR signalling in malignancy. Anticancer Res. 2006, 26: 2557-2566.
2006, [http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=gene&cmd]
Theodorou V, Boer M, Weigelt B, Jonkers J, van d V, Hilkens J: Fgf10 is an oncogene activated by MMTV insertional mutagenesis in mouse mammary tumors and overexpressed in a subset of human breast carcinomas. Oncogene. 2004, 23: 6047-6055. 10.1038/sj.onc.1207816.
Tomlins SA, Rhodes DR, Perner S, Dhanasekaran SM, Mehra R, Sun XW, Varambally S, Cao X, Tchinda J, Kuefer R, Lee C, Montie JE, Shah RB, Pienta KJ, Rubin MA, Chinnaiyan AM: Recurrent fusion of TMPRSS2 and ETS transcription factor genes in prostate cancer. Science. 2005, 310: 644-648. 10.1126/science.1117679.
Liu W, Chang B, Sauvageot J, Dimitrov L, Gielzak M, Li T, Yan G, Sun J, Sun J, Adams TS, Turner AR, Kim JW, Meyers DA, Zheng SL, Isaacs WB, Xu J: Comprehensive assessment of DNA copy number alterations in human prostate cancers using Affymetrix 100K SNP mapping array. Genes Chromosomes Cancer. 2006, 45: 1018-1032. 10.1002/gcc.20369.
Qin HR, Iliopoulos D, Semba S, Fabbri M, Druck T, Volinia S, Croce CM, Morrison CD, Klein RD, Huebner K: A role for the WWOX gene in prostate cancer. Cancer Res. 2006, 66: 6477-6481. 10.1158/0008-5472.CAN-06-0956.
Xu J, Dimitrov L, Chang BL, Adams TS, Turner AR, Meyers DA, Eeles RA, Easton DF, Foulkes WD, Simard J, Giles GG, Hopper JL, Mahle L, Moller P, Bishop T, Evans C, Edwards S, Meitz J, Bullock S, Hope Q, Hsieh CL, Halpern J, Balise RN, Oakley-Girvan I, Whittemore AS, Ewing CM, Gielzak M, Isaacs SD, Walsh PC, Wiley KE, Isaacs WB, Thibodeau SN, McDonnell SK, Cunningham JM, Zarfas KE, Hebbring S, Schaid DJ, Friedrichsen DM, Deutsch K, Kolb S, Badzioch M, Jarvik GP, Janer M, Hood L, Ostrander EA, Stanford JL, Lange EM, Beebe-Dimmer JL, Mohai CE, Cooney KA, Ikonen T, Baffoe-Bonnie A, Fredriksson H, Matikainen MP, Tammela TL, Bailey-Wilson J, Schleutker J, Maier C, Herkommer K, Hoegel JJ, Vogel W, Paiss T, Wiklund F, Emanuelsson M, Stenman E, Jonsson BA, Gronberg H, Camp NJ, Farnham J, Cannon-Albright LA, Seminara D: A combined genomewide linkage scan of 1,233 families for prostate cancer-susceptibility genes conducted by the international consortium for prostate cancer genetics. Am J Hum Genet. 2005, 77: 219-229. 10.1086/432377.
Kammerer S, Roth RB, Reneland R, Marnellos G, Hoyal CR, Markward NJ, Ebner F, Kiechle M, Schwarz-Boeger U, Griffiths LR, Ulbrich C, Chrobok K, Forster G, Praetorius GM, Meyer P, Rehbock J, Cantor CR, Nelson MR, Braun A: Large-scale association study identifies ICAM gene region as breast and prostate cancer susceptibility locus. Cancer Res. 2004, 64: 8906-8910. 10.1158/0008-5472.CAN-04-1788.
Xu J, Zheng SL, Hawkins GA, Faith DA, Kelly B, Isaacs SD, Wiley KE, Chang B, Ewing CM, Bujnovszky P, Carpten JD, Bleecker ER, Walsh PC, Trent JM, Meyers DA, Isaacs WB: Linkage and association studies of prostate cancer susceptibility: evidence for linkage at 8p22–23. Am J Hum Genet. 2001, 69: 341-350. 10.1086/321967.
Kraft P, Pharoah P, Chanock SJ, Albanes D, Kolonel LN, Hayes RB, Altshuler D, Andriole G, Berg C, Boeing H, Burtt NP, Bueno-de-Mesquita B, Calle EE, Cann H, Canzian F, Chen YC, Crawford DE, Dunning AM, Feigelson HS, Freedman ML, Gaziano JM, Giovannucci E, Gonzalez CA, Haiman CA, Hallmans G, Henderson BE, Hirschhorn JN, Hunter DJ, Kaaks R, Key T, Le Marchand L, Ma J, Overvad K, Palli D, Pike MC, Riboli E, Rodriguez C, Setiawan WV, Stampfer MJ, Stram DO, Thomas G, Thun MJ, Travis R, Trichopoulou A, Virtamo J, Wacholder S: Genetic variation in the HSD17B1 gene and risk of prostate cancer. PLoS Genet. 2005, 1: e68-10.1371/journal.pgen.0010068.
Breast Cancer Association Consortium: Commonly studied single-nucleotide polymorphisms and breast cancer: results from the Breast Cancer Association Consortium. J Natl Cancer Inst. 2006, 98: 1382-1396.
Antoniou AC, Easton DF: Models of genetic susceptibility to breast cancer. Oncogene. 2006, 25: 5898-5905. 10.1038/sj.onc.1209879.
Smith P, McGuffog L, Easton DF, Mann GJ, Pupo GM, Newman B, Chenevix-Trench G, Szabo C, Southey M, Renard H, Odefrey F, Lynch H, Stoppa-Lyonnet D, Couch F, Hopper JL, Giles GG, McCredie MR, Buys S, Andrulis I, Senie R, Goldgar DE, Oldenburg R, Kroeze-Jansema K, Kraan J, Meijers-Heijboer H, Klijn JG, van Asperen C, van L I, Vasen HF, Cornelisse CJ, Devilee P, Baskcomb L, Seal S, Barfoot R, Mangion J, Hall A, Edkins S, Rapley E, Wooster R, Chang-Claude J, Eccles D, Evans DG, Futreal PA, Nathanson KL, Weber BL, Rahman N, Stratton MR: A genome wide linkage search for breast cancer susceptibility genes. Genes Chromosomes Cancer. 2006, 45: 646-655. 10.1002/gcc.20354.
Walsh T, Casadei S, Coats KH, Swisher E, Stray SM, Higgins J, Roach KC, Mandell J, Lee MK, Ciernikova S, Foretova L, Soucek P, King MC: Spectrum of mutations in BRCA1, BRCA2, CHEK2, and TP53 in families at high risk of breast cancer. JAMA. 2006, 295: 1379-1388. 10.1001/jama.295.12.1379.
Berndt SI, Chatterjee N, Huang WY, Chanock SJ, Welch R, Crawford ED, Hayes RB: Variant in sex hormone-binding globulin gene and the risk of prostate cancer. Cancer Epidemiol Biomarkers Prev. 2007, 16: 165-168. 10.1158/1055-9965.EPI-06-0689.
Bergman A, Karlsson P, Berggren J, Martinsson T, Bjorck K, Nilsson S, Wahlstrom J, Wallgren A, Nordling M: Genome-wide linkage scan for breast cancer susceptibility loci in Swedish hereditary non-BRCA1/2 families: suggestive linkage to 10q23.32–q25.3. Genes Chromosomes Cancer. 2007, 46: 302-309. 10.1002/gcc.20405.
Rahman N, Seal S, Thompson D, Kelly P, Renwick A, Elliott A, Reid S, Spanova K, Barfoot R, Chagtai T, Jayatilake H, McGuffog L, Hanks S, Evans DG, Eccles D, Easton DF, Stratton MR: PALB2, which encodes a BRCA2-interacting protein, is a breast cancer susceptibility gene. Nat Genet. 2007, 39: 165-167. 10.1038/ng1959.
Cox A, Dunning AM, Garcia-Closas M, Balasubramanian S, Reed MW, Pooley KA, Scollen S, Baynes C, Ponder BA, Chanock S, Lissowska J, Brinton L, Peplonska B, Southey MC, Hopper JL, McCredie MR, Giles GG, Fletcher O, Johnson N, Dos SSI, Gibson L, Bojesen SE, Nordestgaard BG, Axelsson CK, Torres D, Hamann U, Justenhoven C, Brauch H, Chang-Claude J, Kropp S, Risch A, Wang-Gohrke S, Schurmann P, Bogdanova N, Dork T, Fagerholm R, Aaltonen K, Blomqvist C, Nevanlinna H, Seal S, Renwick A, Stratton MR, Rahman N, Sangrajrang S, Hughes D, Odefrey F, Brennan P, Spurdle AB, Chenevix-Trench G, Beesley J, Mannermaa A, Hartikainen J, Kataja V, Kosma VM, Couch FJ, Olson JE, Goode EL, Broeks A, Schmidt MK, Hogervorst FB, Veer LJ, Kang D, Yoo KY, Noh DY, Ahn SH, Wedren S, Hall P, Low YL, Liu J, Milne RL, Ribas G, Gonzalez-Neira A, Benitez J, Sigurdson AJ, Stredrick DL, Alexander BH, Struewing JP, Pharoah PD, Easton DF: A common coding variant in CASP8 is associated with breast cancer risk. Nat Genet. 2007, 39: 352-358. 10.1038/ng1981.
Camp NJ, Farnham JM, Cannon-Albright LA: Localization of a prostate cancer predisposition gene to an 880-kb region on chromosome 22q12.3 in Utah high-risk pedigrees. Cancer Res. 2006, 66: 10205-10212. 10.1158/0008-5472.CAN-06-1233.
Lange EM, Ho LA, Beebe-Dimmer JL, Wang Y, Gillanders EM, Trent JM, Lange LA, Wood DP, Cooney KA: Genome-wide linkage scan for prostate cancer susceptibility genes in men with aggressive disease: significant evidence for linkage at chromosome 15q12. Hum Genet. 2006, 119: 400-407. 10.1007/s00439-006-0149-6.
Yeager M, Orr N, Hayes RB, Jacobs KB, Kraft P, Wacholder S, Minichiello MJ, Fearnhead P, Yu K, Chatterjee N, Wang Z, Welch R, Staats BJ, Calle EE, Feigelson HS, Thun MJ, Rodriguez C, Albanes D, Virtamo J, Weinstein S, Schumacher FR, Giovannucci E, Willett WC, Cancel-Tassin G, Cussenot O, Valeri A, Andriole GL, Gelmann EP, Tucker M, Gerhard DS, Fraumeni JF, Hoover R, Hunter DJ, Chanock SJ, Thomas G: Genome-wide association study of prostate cancer identifies a second risk locus at 8q24. Nat Genet. 2007, 39: 645-649. 10.1038/ng2022.
Nasu K, Tanji N, Nishioka R, Wang J, Yanagihara Y, Ozawa A, Yokoyama M, Sakayama K: EXpression of ErbB proteins in human prostate. Arch Androl. 2006, 52: 185-190. 10.1080/01485010500316238.
Soung YH, Lee JW, Kim SY, Wang YP, Jo KH, Moon SW, Park WS, Nam SW, Lee JY, Yoo NJ, Lee SH: Somatic mutations of the ERBB4 kinase domain in human cancers. Int J Cancer. 2006, 118: 1426-1429. 10.1002/ijc.21507.
Gallo RM, Bryant I, Fry R, Williams EE, Riese DJ: Phosphorylation of ErbB4 on Tyr1056 is critical for inhibition of colony formation by prostate tumor cell lines. Biochem Biophys Res Commun. 2006, 349: 372-382. 10.1016/j.bbrc.2006.08.055.
Skol AD, Scott LJ, Abecasis GR, Boehnke M: Joint analysis is more efficient than replication-based analysis for two-stage genome-wide association studies. Nat Genet. 2006, 38: 209-213. 10.1038/ng1706.
Wang H, Thomas DC, Pe'er I, Stram DO: Optimal two-stage genotyping designs for genome-wide association scans. Genet Epidemiol. 2006, 30: 356-368. 10.1002/gepi.20150.
Klein RJ, Zeiss C, Chew EY, Tsai JY, Sackler RS, Haynes C, Henning AK, SanGiovanni JP, Mane SM, Mayne ST, Bracken MB, Ferris FL, Ott J, Barnss C, Hoh J: Complement factor H polymorphism in age-related macular degeneration. Science. 2005, 308: 385-389. 10.1126/science.1109557.
Despriet DD, Klaver CC, Witteman JC, Bergen AA, Kardys I, de Maat MP, Boekhoorn SS, Vingerling JR, Hofman A, Oostra BA, Uitterlinden AG, Stijnen T, van Duijn CM, de Jong PT: Complement factor H polymorphism, complement activators, and risk of age-related macular degeneration. JAMA. 2006, 296: 301-309. 10.1001/jama.296.3.301.
Edwards AO, Ritter R, Abel KJ, Manning A, Panhuysen C, Farrer LA: Complement factor H polymorphism and age-related macular degeneration. Science. 2005, 308: 421-424. 10.1126/science.1110189.
Schaumberg DA, Christen WG, Kozlowski P, Miller DT, Ridker PM, Zee RY: A prospective assessment of the Y402H variant in complement factor H, genetic variants in C-reactive protein, and risk of age-related macular degeneration. Invest Ophthalmol Vis Sci. 2006, 47: 2336-2340. 10.1167/iovs.05-1456.
Acknowledgements
We thank Drs Emelia J. Benjamin and Martin G. Larson for their participation in the Framingham Heart Study Cancer Phenotype Working Group and for their contribution to the conception, design and interpretation of the data and comments on the drafting of the manuscript.
We thank the FHS participants for their ongoing participation and dedication to the study making this work possible.
NHLBI's Framingham Heart Study is supported by contract number N01-HC-25195. FHS 100K analyses were conducted using the Boston University. Linux Cluster for Genetic Analysis (LinGA) funded by the NIH NCRR (National Center for Research Resources) Shared Instrumentation grant 1S10RR163736-01A1 http://www.bu.edu/dbin/sph/departments/biostatistics/linga_publications.php.
This article has been published as part of BMC Medical Genetics Volume 8 Supplement 1, 2007: The Framingham Heart Study 100,000 single nucleotide polymorphisms resource. The full contents of the supplement are available online at http://www.biomedcentral.com/1471-2350/8?issue=S1.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
All authors have made substantial contributions to conception and design or acquisition of phenotypic data. JMM, SJW, DF, DL, CLR contributed to the analysis and interpretation of data. JMM, CLR, DL, DF, and SJW have been involved in drafting the manuscript or revising it critically for important intellectual content and all authors have read and approved the final manuscript.
Electronic supplementary material
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an open access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Murabito, J.M., Rosenberg, C.L., Finger, D. et al. A genome-wide association study of breast and prostate cancer in the NHLBI's Framingham Heart Study. BMC Med Genet 8 (Suppl 1), S6 (2007). https://doi.org/10.1186/1471-2350-8-S1-S6
Published:
DOI: https://doi.org/10.1186/1471-2350-8-S1-S6