
Abstract
Background
Ischaemic stroke is a common disorder with genetic and environmental components contributing to overall risk. Atherothromboembolic abnormalities, which play a crucial role in the pathogenesis of ischaemic stroke, are often the end result of dysregulation of lipid metabolism. The ATP Binding Cassette Transporter (ABCA1) is a key gene involved in lipid metabolism. It encodes the cholesterol regulatory efflux protein which mediates the transfer of cellular phospholipids and cholesterol to acceptor apolipoproteins such as apolipoprotein A-I (ApoA-I). Common polymorphisms in this gene affect High Density Lipoprotein Cholesterol (HDL-C) and Apolipoprotein A-I levels and so influence the risk of atherosclerosis. This study has assessed the distribution of ABCA1 polymorphisms and haplotype arrangements in patients with ischaemic stroke and compared them to an appropriate control group. It also examined the relationship of these polymorphisms with serum lipid profiles in cases and controls.
Methods
We studied four common polymorphisms in ABCA1 gene: G/A-L158L, G/A-R219K, G/A-G316G and G/A-R1587K in 400 Caucasian ischaemic stroke patients and 487 controls. Dynamic Allele Specific Hybridisation (DASH) was used as the genotyping assay.
Results
Genotype and allele frequencies of all polymorphisms were similar in cases and controls, except for a modest difference in the ABCA1 R219K allele frequency (P-value = 0.05). Using the PHASE2 program, haplotype frequencies for the four loci (158, 219, 316, and 1587) were estimated in cases and controls. There was no significant difference in overall haplotypes arrangement in patients group compared to controls (p = 0.27). 2211 and 1211 haplotypes (1 = common allele, 2 = rare allele) were more frequent in cases (p = 0.05). Adjusted ORs indicated 40% and 46% excess risk of stroke for these haplotypes respectively. However, none of the adjusted ORs were statistically significant. Individuals who had R219K "22" genotype had a higher LDL level (p = 0.001).
Conclusion
Our study does not support a major role for the ABCA1 gene as a risk factor for ischaemic stroke. Some haplotypes may confer a minor amount of increased risk or protection. Polymorphisms in this gene may influence serum lipid profile.
Similar content being viewed by others

Background
Ischaemic stroke is a complex disorder. Hypertension and dyslipidemia are known to influence atherosclerosis and so predispose to ischaemic stroke. Hypercholesterolemia increases the risk of stroke [1], while lipid lowering therapy significantly reduces risk of stroke [2]. Low HDL has also been reported as a risk factor for ischaemic stroke [3, 4]. Several genes involved in lipid metabolism such as Paraoxonase (PON), Lipoprotein Lipase (LPL) and Fatty Acid-Binding Protein 2 (FABP2) have been examined in the stroke populations [5–8]. ApoE protein is involved in cholesterol transport and some studies suggest ApoE *ε 4 and ApoE *ε 2 alleles are associated with higher risk and lower risk of ischaemic stroke respectively, but this has not been confirmed in all studies [9, 10].
Homozygous mutations including deletions and polymorphisms of the ATP-binding cassette transporter 1 (ABCA1) cause Tangier disease, a rare autosomal recessive disorder with congenital HDL deficiency and increased risk of atherosclerosis. Heterozygous mutants develop familial HDL deficiency in which less severe HDL deficiency is associated with reduced cholesterol efflux, which also predispose to atherosclerosis [11–13]. In the general population, low plasma HDL cholesterol (HDL-C) increases the risk of coronary artery disease (CAD) [14–16]. Variations in ABCA1 gene and alteration in gene expression have been shown to affect the risk of atherosclerosis in animal models [17, 18] and invitro studies show that ABCA1 also modulates LDL oxidation in the artery wall cells [19]. ABCA1 gene expression is upregulated in atherosclerotic plaques, further suggesting an association between ABCA1 and atheroma [20]. Reports have suggested a relationship between individual polymorphisms of ABCA1 gene and lipid profiles [21, 22]. Furthermore, ABCA1 appears to be required in neuronal tissue for cholesterol efflux to ApoA-I and ApoE. ABCA1 deficiency in the brain causes a dramatic fall in neuronal ApoE levels [23, 24]. The only published study in ischaemic stroke on 244 Hungarian patients [25] suggests a protective role for the ABCA1-R219K and V771M polymorphisms. The aim of this study was to assess the distribution of different polymorphisms and haplotype arrangements of the ABCA1 gene, and any association with lipid profile, in a series of well-phenotyped ischaemic stroke patients and unaffected control subjects.
Methods
Subjects
After ethical committee approval and informed consent, 400 Caucasian patients admitted to a regional hospital with a CT confirmed diagnosis of ischemic stroke were recruited over a period of 3 years. Four hundred and eighty seven Caucasian individuals from the same region, without any clinical cerebrovascular disease were used as controls. All were volunteers, 194 were part of a birth cohort (Aberdeen Birth Cohort) born in 1921. The others were recruited through general practices, so that overall controls were roughly age matched to cases. For a subgroup of controls (n = 181) detailed lipid parameters including total cholesterol, VLDL-Cholesterol, VLDL-Triglyceride, IDL, LDL, HDL2, HDL3 were available for comparison with ABCA1 genotypes.
Classification of stroke patients
On the basis of clinical, laboratory and radiological parameters, all cases were assessed by an experienced stroke physician according to Trial of Org 10172 in Acute Stroke Treatment (TOAST) criteria [26] to determine stroke subtype (Table 2). Haemorrhagic stroke cases were not included. For most patients lipid levels were checked either at admission or the following morning. No patients included in this analysis were known to be on statin on admission.
Genotyping method and markers
DNA was extracted using Nucleon® DNA extraction kits. 5–10ng DNA was amplified through Hot Start PCR protocol using Immolase Taq DNA polymerase®. We used different sets of primers for each SNP as follows:
1- ABCA1 -rs2230805 (G/A; L158L); designated as [ ABCA1 -6]
ABCA1-2230805F: 5'-biotin-TAGACTTTGGGAGAGAGAGGTTGT-3'
ABCA1-2230805R: 5'-AATGAAACCTTCTCTGGGTTCC-3'
2- ABCA1 -rs2234884 (G1051A; R219K); designated as [ ABCA1 -3]
ABCA1-2234884F: 5'-biotin-AATTTCTGAGCTTTGTGGACTA-3'
ABCA1-2234884R: 5'-GCTCTGCTGCAGTCATTTTCTC-3'
3- ABCA1 -rs2246841 (G888A; G316G); designated as [ ABCA1 -5]
ABCA1-2246841F: 5'-biotin-TACCAGTTGAGAGACTTGATCTTC-3'
ABCA1-2246841R: 5'-TCTCGTATTGTCTGTGGGCATC-3'
4- ABCA1 -rs1997618 (c/t, T1555I)
ABCA1-1997618F: 5'-biotin-CCGAGTCAAGAAGTTAATGATGC-3'
ABCA1-1997618R: 5'-GCTTTAGGTGTTTCTTCATTTGTTT-3'
5- ABCA1 -rs2234886 (G5155A; R1587K); designated as [ ABCA1 -4]
ABCA1-2234886F: 5'-biotin-CAGCGGTTTACCTTGACATTATT-3'
ABCA1-2234886R: 5'-GAAGATTTATGACAGGACTGGACAC-3'
6- ABCA1 -rs1883024 (c/t, P1648L)
ABCA1-1883024F: 5'-biotin-TATACAGACACAGCCACACTTA-3'
ABCA1-1883024R: 5'-ATCTCACCAAGCAGCAGTTCTC-3'
Of the six ABCA1 SNPs, only four SNPs (G/A-L158L, G/A-R219K, G/A-G316G and G/A-R1587K) were polymorphic in the Scottish population. All had genotype frequencies in Hardy Weinberg equilibrium. Genotyping assays for determining different alleles were based on the Dynamic Allele Specific Hybridisation (DASH) technique as described by the developers [27]. Genotype scoring in this method is based on the melting temperature curves of the amplified DNA strand containing the polymorphic site and its complementary specific probe in presence of a dye.
Data analysis
Association between markers and disease phenotype was tested with Pearson χ2 test. To explore distribution of categorical data, hypertension and gender, between cases and controls, chi-square test was used. Lipid parameters were log transformed before analysis. Numerical covariates, age, total cholesterol, HDL, LDL, total triglyceride and glucose, were compared between cases and controls by t-test. Smoking status was incomplete for a subgroup of controls and therefore not included in analysis. A univariate logistic regression method was carried out in order to identify factors potentially associated with risk of stroke. To control for the effect of confounding factors and covariates, multiple logistic regression with SPSS version 14 (Statistical Package for Social Science) was used for statistical analysis. A p-value of less than or equal to 0.05 was considered statistically significant.
ANOVA was used for comparing the effect of different genotypes on lipid profiles. Independent samples T-test was also used to compare means of different groups based on quartiles or carrier status. Haplotype frequencies for the four loci (G/A-L158L, G/A-R219K, G/A-G316G and G/A-R1587K) were estimated for cases and controls, using PHASE Ver.2.11 [28].
Results
Demographic parameters and serology results are shown in Table 1.
Allelic distributions and genotype frequencies
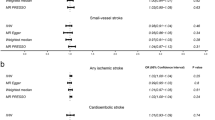
ABCA1-6 (G/A; L158L) "G" allele frequency (L variant) in cases and controls was 69.7% and 72.3% respectively (p = 0.25; OR = 0.88, 95%CI: 0.71–1.09). ABCA1-3 (G1051A; R219K) "G" allele frequency (R variant) was 68.2% in cases and 73.2% in controls (p = 0.05; OR = 0.79, 95%CI: 0.62–1.00), ABCA1-5 (G/A; G316G) "G" allele frequency (G variant) was 88% in cases and 86.7% in controls (p = 0.42; OR = 1.13, 95%CI: 0.84–1.52); ABCA1-4 (G5155A; R1587K) "G" allele frequency (R variant) was 77.4% in cases and 75.9% in controls (p = 0.47; OR = 1.09, 95%CI: 0.86–1.37). After adjusting for confounding factors and covariates, minor changes in the risk were not statistically significant.
In addition to a trend to lower ABCA1-3 (G1051A; R219K) "G" allele frequency in all cases (p = 0.05), especially in males (p = 0.04), the "22" genotype was higher in LVD cases (p = 0.04) and also in patients over 65 years (p = 0.01), compared to controls. ABCA1-5 (G/A; G316G) "11" genotype was also commoner in cases than in controls (p = 0.04). However after adjusting OR for confounders the difference did not remain significant.
There were no significant differences in allele frequencies between cases and controls in each gender group, or between stroke TOAST subgroups for the other SNPs tested.
Effects of genotypes on lipid profile
We also studied the effects of different ABCA1 genotypes on lipid profile in all cases and controls. Cases with ABCA1-3 (G1051A; R219K) "22" genotype had a higher LDL level compared to controls which remained significant after Bonferroni correction (p = 0.003). In 181 of the controls who had a more detailed lipid profile, no differences were found in VLDL-Cholesterol, IDL, LDL, HDL2, HDL3, total cholesterol and triglyceride levels in females or males between different genotypes of ABCA1. However, in this subgroup, females with ABCA1-3 (G1051A; R219K) "11" and ABCA1-4 (G5155A; R1587K) "22" genotypes had a higher level of IDL (p = 0.01 and p = 0.02) respectively.
Effects of alleles on lipid profile
Comparing the lipid profiles in carriers of different ABCA1 alleles revealed that individuals who were the ABCA1-R219K carrier (K allele) had a lower TG level than non carriers (p = 0.005). This trend was observed in cases (p = 0.017) but not in controls (p = 0.8). The lipid profile of the population in the presence of different ABCA1 gene alleles has been summarised in tables 3.
Haplotypes
Haplotype analysis was performed using PHASE version 2.11. The PHASE program [28], resulted in reconstruction of 16 different haplotypes in cases and controls. Overall haplotype frequencies in cases and controls were not reported significantly different by the program (p = 0.27), although there were differences in specific haplotypes between the groups. Adjusted ORs indicated 40%, 27% and 46% excess risk of stroke for haplotypes 2211, 2212 and 1211 respectively. However, none of these risks were statistically significant (Table 4). The haplotypes arrangements did not influence the lipid profile of cases or controls.
Discussion
The ABCA1 gene is known to have a crucial role in lipid metabolism [29, 30]. Mutations or polymorphisms in this gene are known to cause dyslipidemia such as low HDL-C and thus predispose to atherosclerosis [31, 32]. Several polymorphisms of the ABCA1 gene have been investigated for their association with CAD [33–35]. Other works have reported that CAD patients who are carriers of R219K allele had less severe atherosclerosis [31] and overall lower risk of CAD [36]. Andrikovics et al recently reported a higher frequency of R219K in controls than in Hungarian stroke patients and suggested a protective role for this polymorphism [25]. By contrast, our control group had a higher "R219" allele frequency, while the stroke population had a higher "219K" allele frequency. The "219K" allele frequency is similar to that reported in other studies of Irish and other Scottish populations [36]. Two SNPs, P1648L and T1555I, were not polymorphic in our population.
While the R219K -G1051A- (A or "K" variant) has been associated with decreased TG, increased HDL and subsequently a lower risk for atherosclerotic progression, in contrast the R allele has been associated with vascular disease [31]. This has not been confirmed in our study, although in our stroke population those with R219K "22" genotype (AA) had a higher level of LDL and the "K allele" carriers had a lower TG. Clee et al also reported lower TG in the carriers of 219K variant and this finding was replicated in our population (p = 0.006). The HDL level showed no significant difference among different R219K genotypes.
It is also of interest that a protective role for the 219K allele has not been confirmed by all studies. Ethnic background or other environmental factors may weaken the link with HDL-C levels. However, in three other European populations in contrast to a Japanese one, R219 has been constantly the wild type allele [37].
Haplotype analysis can provide additional power in association studies in complex diseases [38]. Results using different programs are usually consistent, but sometimes there are minor variations [6, 39]. We performed haplotype analysis in the remaining four SNPs, and only the 2211 and 1211 haplotypes were more frequent in cases (p = 0.05). Only a small proportion of individuals carried these haplotypes, thus the result should be interpreted with caution.
We found an association between LDL levels and ABCA1 genotype, but not with HDL. Epidemiological studies of ABCA1 polymorphisms and HDL levels suggest that only 10% of HDL level variation maybe explained by this gene [40] and thus our study may not have been large enough to detect this. Other studies have shown an association between the R219K polymorphism and MI, but no association between haplotype arrangements and MI. Polymorphisms in the promoter region (C-564T) and in the coding region (R1587K) have shown an association with ApoA-I levels but these have not been associated with vascular disease. Another study has suggested that rare alleles with major phenotypic effects contribute significantly to low plasma HDL [41]. Although lipid measurements were made early after admission, possible confounders include the acute lipid changes that occur after acute stroke. The lipid levels reported in our study are similar to those values on the morning after admission reported by Dyker, Weir and Lees in patients after acute stroke [42]. The changes in lipids post stroke remain controversial, but further studies of changes in lipid profile will be difficult because of the early introduction of statin therapy on the basis of studies such as SPARCL [43].
Conclusion
In conclusion ABCA1 was not associated with ischaemic stroke in our population. Among the studied ABCA1 gene polymorphisms, R219K has the greatest impact on lipid profile especially LDL and TG. Large scale epidemiological studies may be necessary to definitively confirm an association of this gene with specific vascular diseases.
References
Ebrahim S, Sung J, Song YM, Ferrer RL, Lawlor DA, Smith GD: Serum cholesterol, haemorrhagic stroke, ischaemic stroke, and myocardial infarction: Korean national health system prospective cohort study. BMJ. 2006, 333: 22-10.1136/bmj.38855.610324.80.
Collins R, Armitage J, Parish S, Sleigh P, Peto R, Group HPSC: MRC/BHF Heart Protection Study of cholesterol-lowering with simvastatin in 5963 people with diabetes: a randomised placebo-controlled trial. Lancet. 2003, 361: 2005-2016. 10.1016/S0140-6736(03)12475-0.
Albucher JF, Ferrieres J, Ruidavets JB, Guiraud-Chaumeil B, Perret BP, Chollet F: Serum lipids in young patients with ischaemic stroke: a case-control study. J Neurol Neurosurg Psychiatry. 2000, 69: 29-33. 10.1136/jnnp.69.1.29.
Ohira T, Shahar E, Chambless LE, Rosamond WD, Mosley TH, Folsom AR: Risk Factors for Ischemic Stroke Subtypes: The Atherosclerosis Risk in Communities Study. Stroke. 2006, 37: 2493-2498. 10.1161/01.STR.0000239694.19359.88.
Ranade K, Kirchgessner TG, Iakoubova OA, Devlin JJ, DelMonte T, Vishnupad P, Hui L, Tsuchihashi Z, Sacks FM, Sabatine MS, Braunwald E, White TJ, Shaw PM, Dracopoli NC: Evaluation of the Paraoxonases as Candidate Genes for Stroke: Gln192Arg Polymorphism in the Paraoxonase 1 Gene Is Associated With Increased Risk of Stroke. Stroke. 2005, 36: 2346-2350. 10.1161/01.STR.0000185703.88944.7d.
Pasdar A, Ross-Adams H, Cumming A, Cheung J, Whalley L, St Clair D, MacLeod MJ: Paraoxonase gene polymorphisms and haplotype analysis in a stroke population. BMC Medical Genetics. 2006, 7: 28-10.1186/1471-2350-7-28.
Carlsson M, Orho-Melander M, Hedenbro J, Almgren P, Groop LC: The T 54 Allele of the Intestinal Fatty Acid-Binding Protein 2 Is Associated with a Parental History of Stroke. J Clin Endocrinol Metab. 2000, 85: 2801-2804. 10.1210/jc.85.8.2801.
Morrison AC, Ballantyne CM, Bray M, Chambless LE, Sharrett AR, Boerwinkle E: LPL polymorphism predicts stroke risk in men. Genet Epidemiol. 2002, 22: 233-242. 10.1002/gepi.0191.
Kessler C, Spitzer C, Stauske D, Mende S, Stadlmuller J, Walther R, Rettig R: The Apolipoprotein E and beta-fibrinogen G/A-455 Gene Polymorphisms Are Associated With Ischemic Stroke Involving Large-Vessel Disease. Arterioscler Thromb Vasc Biol. 1997, 17: 2880-
MacLeod MJ, De Lange RP, Breen G, Meiklejohn D, Lemmon H, Clair DS: Lack of association between apolipoprotein E genoype and ischaemic stroke in a Scottish population. Eur J Clin Invest. 2001, 31: 570-573. 10.1046/j.1365-2362.2001.00851.x.
Brooks-Wilson A, Marcil M, Clee SM, Zhang LH, Roomp K, van Dam M, Yu L, Brewer C, Collins JA, Molhuizen HO, Loubser O, Ouelette BF, Fichter K, Ashbourne-Excoffon KJ, Sensen CW, Scherer S, Mott S, Denis M, Martindale D, Frohlich J, Morgan K, Koop B, Pimstone S, Kastelein JJ, Hayden MR: Mutations in ABC1 in Tangier disease and familial high-density lipoprotein deficiency. Nat Genet. 1999, 22: 336-345. 10.1038/11905.
Oram JF, Vaughan AM: ABCA1-mediated transport of cellular cholesterol and phospholipids to HDL apolipoproteins. Current Opinion in Lipidology. 2000, 11: 253-260. 10.1097/00041433-200006000-00005.
Brousseau ME, Schaefer EJ, Dupuis J, Eustace B, Van Eerdewegh P, Goldkamp AL, Thurston LM, FitzGerald MG, Yasek-McKenna D, O'Neill G, Eberhart GP, Weiffenbach B, Ordovas JM, Freeman MW, Brown RH, Gu JZ: Novel mutations in the gene encoding ATP-binding cassette 1 in four Tangier disease kindreds. Journal of Lipid Research. 2000, 41: 433-441.
Wilson PW, Abbott RD, Castelli WP: High density lipoprotein cholesterol and mortality. The Framingham Heart Study. Arterioscler Thromb Vasc Biol. 1988, 8: 737-741.
Goldbourt U, Yaari S, Medalie JH: Isolated Low HDL Cholesterol As a Risk Factor for Coronary Heart Disease Mortality: A 21-Year Follow-up of 8000 Men. Arterioscler Thromb Vasc Biol. 1997, 17: 107-113.
Miller GJ, Miller NE: Plasma-high-density-lipoprotein concentration and development of ischaemic heart-disease. Lancet. 1975, 1: 16-19. 10.1016/S0140-6736(75)92376-4.
Aiello RJ, Brees D, Francone OL: ABCA1-Deficient Mice: Insights Into the Role of Monocyte Lipid Efflux in HDL Formation and Inflammation. Arterioscler Thromb Vasc Biol. 2003, 23: 972-10.1161/01.ATV.0000054661.21499.FB.
Joyce C, Freeman L, Brewer HB, Santamarina-Fojo S: Study of ABCA1 Function in Transgenic Mice. Arterioscler Thromb Vasc Biol. 2003, 23: 965-10.1161/01.ATV.0000055194.85073.FF.
Reddy ST, Hama S, Ng C, Grijalva V, Navab M, Fogelman AM: ATP-Binding Cassette Transporter 1 Participates in LDL Oxidation by Artery Wall Cells. Arterioscler Thromb Vasc Biol. 2002, 22: 1877-1883. 10.1161/01.ATV.0000035700.82829.2A.
Albrecht C, Soumian S, Amey JS, Sardini A, Higgins CF, Davies AH, Gibbs RGJ: ABCA1 Expression in Carotid Atherosclerotic Plaques. Stroke. 2004, 35: 2801-2806. 10.1161/01.STR.0000147036.07307.93.
Ho Hong S, Rhyne J, Miller M: Novel Polypyrimidine Variation (IVS46: del T -39...-46) in ABCA1 Causes Exon Skipping and Contributes to HDL Cholesterol Deficiency in a Family With Premature Coronary Disease. Circ Res. 2003, 93: 1006-1012. 10.1161/01.RES.0000102957.84247.8F.
Hodoglugil U, Williamson DW, Huang Y, Mahley RW: Common polymorphisms of ATP binding cassette transporter A1, including a functional promoter polymorphism, associated with plasma high density lipoprotein cholesterol levels in Turks. Atherosclerosis. 2005, 183: 199-212. 10.1016/j.atherosclerosis.2005.03.004.
Hirsch-Reinshagen V, Zhou S, Burgess BL, Bernier L, McIsaac SA, Chan JY, Tansley GH, Cohn JS, Hayden MR, Wellington CL: Deficiency of ABCA1 Impairs Apolipoprotein E Metabolism in Brain. J Biol Chem. 2004, 279: 41197-41207. 10.1074/jbc.M407962200.
Wahrle SE, Jiang H, Parsadanian M, Legleiter J, Han X, Fryer JD, Kowalewski T, Holtzman DM: ABCA1 Is Required for Normal Central Nervous System ApoE Levels and for Lipidation of Astrocyte-secreted apoE. J Biol Chem. 2004, 279: 40987-40993. 10.1074/jbc.M407963200.
Andrikovics H, Pongrbcz E, Kalina , Szilvbsi A, Aslanidis C, Schmitz G, Tordai A: Decreased Frequencies of ABCA1 Polymorphisms R219K and V771M in Hungarian Patients with Cerebrovascular and Cardiovascular Diseases. Cerebrovascular Diseases. 2006, 21: 254-259. 10.1159/000091223.
Adams HP, Bendixen BH, Kappelle LJ, Biller J, Love BB, Gordon DL, Marsh EE: Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke. 1993, 24: 35-41.
Prince JA, Feuk L, Howell WM, Jobs M, Emahazion T, Blennow K, Brookes AJ: Robust and Accurate Single Nucleotide Polymorphism Genotyping by Dynamic Allele-Specific Hybridization (DASH): Design Criteria and Assay Validation. Genome Res. 2001, 11: 152-162. 10.1101/gr.150201.
Stephens M, Smith NJ, Donnelly P: A new statistical method for haplotype reconstruction from population data. Am J Hum Genet. 2001, 68: 978-989. 10.1086/319501.
Attie AD, Kastelein JP, Hayden MR: Pivotal role of ABCA1 in reverse cholesterol transport influencing HDL levels and susceptibility to atherosclerosis. Journal of Lipid Research. 2001, 42: 1717-1726.
Iida A, Saito S, Sekine A, Kitamura Y, Kondo K, Mishima C, Osawa S, Harigae S, Nakamura Y: High-density single-nucleotide polymorphism (SNP) map of the 150-kb region corresponding to the human ATP-binding cassette transporter A1 (ABCA1) gene. J Hum Genet. 2001, 46: 522-528. 10.1007/s100380170034.
Clee SM, Zwinderman AH, Engert JC, Zwarts KY, Molhuizen HOF, Roomp K, Jukema JW, van Wijland M, van Dam M, Hudson TJ, Brooks-Wilson A, Genest J, Kastelein JJP, Hayden MR: Common Genetic Variation in ABCA1 Is Associated With Altered Lipoprotein Levels and a Modified Risk for Coronary Artery Disease. Circulation. 2001, 103: 1198-1205.
Fredrickson DS: The inheritance of high density lipoprotein deficiency (Tangier Disease). J Clin Invest. 1964, 43:228-36.: 228-236.
Cenarro A, Artieda M, Castillo S, Mozas P, Reyes G, Tejedor D, Alonso R, Mata P, Pocovi M, Civeira F: A common variant in the ABCA1 gene is associated with a lower risk for premature coronary heart disease in familial hypercholesterolaemia. J Med Genet. 2003, 40: 163-168. 10.1136/jmg.40.3.163.
Evans D, Beil FU: The association of the R219K polymorphism in the ATP-binding cassette transporter 1 (ABCA1) gene with coronary heart disease and hyperlipidaemia. Journal of Molecular Medicine. 2003, 81: 264-270. 10.1007/s00109-003-0465-4.
Frikke-Schmidt R, Nordestgaard BG, Schnohr P, Steffensen R, Tybjaerg-Hansen A: Mutation in ABCA1 Predicted Risk of Ischemic Heart Disease in the Copenhagen City Heart Study Population. Journal of the American College of Cardiology. 2005, 46: 1516-1520. 10.1016/j.jacc.2005.06.066.
Tregouet DA, Ricard S, Nicaud V, Arnould I, Soubigou S, Rosier M, Duverger N, Poirier O, Mace S, Kee F, Morrison C, Denefle P, Tiret L, Evans A, Deleuze JF, Cambien F: In-Depth Haplotype Analysis of ABCA1 Gene Polymorphisms in Relation to Plasma ApoA1 Levels and Myocardial Infarction. Arterioscler Thromb Vasc Biol. 2004, 24: 775-781. 10.1161/01.ATV.0000121573.29550.1a.
Singaraja RR, Brunham LR, Visscher H, Kastelein JJP, Hayden MR: Efflux and Atherosclerosis: The Clinical and Biochemical Impact of Variations in the ABCA1 Gene. Arterioscler Thromb Vasc Biol. 2003, 23: 1322-1332. 10.1161/01.ATV.0000078520.89539.77.
Yagil Y, Yagil C: Candidate genes, association studies and haplotype analysis in the search for the genetic basis of hypertension. J Hypertens. 2004, 22: 1255-1258. 10.1097/01.hjh.0000125426.50839.4e.
Zhang S, Pakstis AJ, Kidd KK, Zhao H: Comparisons of two methods for haplotype reconstruction and haplotype frequency estimation from population data. Am J Hum Genet. 2001, 69: 906-914. 10.1086/323622.
Knoblauch H, Bauerfeind A, Toliat MR, Becker C, Luganskaja T, Gunther UP, Rohde K, Schuster H, Junghans C, Luft FC, Nurnberg P, Reich JG: Haplotypes and SNPs in 13 lipid-relevant genes explain most of the genetic variance in high-density lipoprotein and low-density lipoprotein cholesterol. Hum Mol Genet. 2004, 13: 993-1004. 10.1093/hmg/ddh119.
Cohen JC, Kiss RS, Pertsemlidis A, Marcel YL, McPherson R, Hobbs HH: Multiple rare alleles contribute to low plasma levels of HDL cholesterol. Science. 2004, 305: 869-872. 10.1126/science.1099870.
Dyker AG, Weir CJ, Lees KR: Influence of cholesterol on survival after stroke: retrospective study. BMJ. 1997, 314: 1584-
The Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) Investigators: High-Dose Atorvastatin after Stroke or Transient Ischemic Attack. N Engl J Med. 2006, 355: 549-559. 10.1056/NEJMoa061894.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2350/8/30/prepub
Acknowledgements
We would like to thank Mashad University of Medical Sciences, Mashad, Iran and the Iranian Ministry of Health for their financial support. Lawrence Whalley holds a career development award from the Wellcome Trust who supported collection of control subject data.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The author(s) declare that they have no competing interests.
Authors' contributions
AP participated in study design, carried out the genotyping and the statistical analyses and drafted the manuscript. GY reviewed and reanalysed the data and commented on statistics. AC helped with study design and commented on the manuscript. LW and DS contributed to the study design, sample collection and helped draft the manuscript. MJM contributed to study design, coordinated recruitment and drafted the manuscript. Authors read and approved the final manuscript.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Pasdar, A., Yadegarfar, G., Cumming, A. et al. The effect of ABCA1gene polymorphisms on ischaemic stroke risk and relationship with lipid profile. BMC Med Genet 8, 30 (2007). https://doi.org/10.1186/1471-2350-8-30
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2350-8-30