
Abstract
Background
Various cytokines and inflammatory mediators are known to be involved in the pathogenesis of rheumatoid arthritis (RA). We hypothesized that polymorphisms in selected inflammatory response and tissue repair genes contribute to the susceptibility to and severity of RA.
Methods
Polymorphisms in TNFA, IL1B, IL4, IL6, IL8, IL10, PAI1, NOS2a, C1INH, PARP, TLR2 and TLR4 were genotyped in 376 Caucasian RA patients and 463 healthy Caucasian controls using single base extension. Genotype distributions in patients were compared with those in controls. In addition, the association of polymorphisms with the need for anti-TNF-α treatment as a marker of RA severity was assessed.
Results
The IL8 781 CC genotype was associated with early onset of disease. The TNFA -238 G/A polymorphism was differentially distributed between RA patients and controls, but only when not corrected for age and gender. None of the polymorphisms was associated with disease severity.
Conclusions
We here report an association between IL8 781 C/T polymorphism and age of onset of RA. Our findings indicate that there might be a role for variations in genes involved in the immune response and in tissue repair in RA pathogenesis. Nevertheless, additional larger genomic and functional studies are required to further define their role in RA.
Similar content being viewed by others

Background
Rheumatoid arthritis (RA) is a severely disabling chronic inflammatory disease that affects millions of people worldwide. Like in other autoimmune diseases females are affected more often than males. The disease course differs widely between patients. While some have low grade disease which is easily controlled by therapy with one disease-modifying anti-rheumatic drug (DMARD), others suffer from rapidly progressive disease with erosions that is therapy resistant, resulting in the use of many different DMARDs or even the need for therapy with the new biologicals directed against TNF-α. Cytokines and other proteins involved in the inflammatory response play a role in RA. Pro-inflammatory cytokines such as TNF-α and IL-1β are regarded as key players in the pathogenesis of RA [1, 2]. This is further underlined by the development of several anti-cytokine drugs in the treatment of RA, with anti-TNF monoclonal antibodies and soluble TNF-α receptor being the most effective. TNF-α is an important pro-inflammatory cytokine. IL-1β in its turn, stimulates expression of IL-6 and IL-8[2]. Since IL-8 is involved in the initiation and amplification of acute inflammatory responses and in chronic inflammation, genetic variations (indirectly) linked to alterations in expression could be associated to RA susceptibility or severity[3–5]. Antibodies directed against the IL-6 receptor are effective in the treatment of RA [6]. IL-4 and IL-10 on the other hand, have been suggested to ameliorate arthritis [7, 8]. Deficiency of IL-4 is associated with increased severity of arthritis in a mouse model[9]. In addition, the V50 variant in the IL-4 receptor causing unresponsiveness to IL-4, is associated with rapidly erosive RA [10]. In addition to inflammatory tissue destruction, factors involved in tissue repair and necrosis or apoptosis are likely to be involved in erosive disease and may also codetermine disease susceptibility. Plasminogen activator inhibitor 1 (PAI-1) inhibits fibrinolysis and tissue repair [11, 12]. Plasminogen deficiency is associated with decreased susceptibility to and severity of arthritis in mice models for RA [13]. Previously the influence of genetic polymorphisms in inflammatory diseases such as RA has become evident. The association with the HLA DRB1 locus is the best characterized and replicated [14, 15]. Linkage studies in RA families and genome wide screening in case control studies have identified over 30 validated additional genetic loci associated with RA such as HLADRB1, PTPN22, TNFAIP3, TRAF1, STAT4, CCR6, PXK, 10p15,12q13 and 22q13 [14, 16–23]. For a recent overview we refer to the review of Orozco and Barton [24]. We used the classic candidate gene approach, including immune response factors that had previously been shown to be involved in RA pathogenesis, or were likely to be involved. This approach increases the chance that when a SNP is found to be significantly associated with disease, it may actually be the functional SNP. However, the relatively small sample size does limit the chance of finding loci of modest effect size and confirmation in independent cohorts is required. The SNPs in the genes were selected on the basis of either a functional effect, both on transcription (e.g. PAI1, IL6, IL10, IL4, IL1B) and amino acid substitution, resulting in functional differences (e.g. PARP) [25–32]. In addition, polymorphisms, such as in TNFA and IL8, previously associated with RA or other inflammatory diseases were considered relevant as well, even if they were positioned in an intron [3, 33–35].
Therefore, in this study including 376 RA patients and 463 controls, we investigated the possible association of polymorphisms in immune response genes (TNFA, IL1B, IL4, IL6, IL8, IL10, C1INH, TLR2, TLR4) and genes involved in tissue repair and apoptosis (PAI1, 5NOS2a, PARP) in relation to RA susceptibility, and with the use of anti-TNF-α therapy as selected marker of disease severity.
Methods
Participants
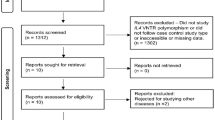
Non related Caucasian patients who met the 1987 ACR criteria for RA and visited the rheumatology outpatient clinic of the Erasmus MC university hospital (n = 76), the Medical Center Rijnmond Zuid (n = 195) or the St. Franciscus Gasthuis Hospital (n = 105), in 2005 were included in the study. Additionally, the patients had to have at least either a positive rheumatoid factor test, or a positive anti-CCP test, or joint erosions. The study was approved by the medical ethical boards of the Erasmus MC and participating hospitals: Medical Center Rijnmond Zuid and the St. Franciscus Gasthuis Hospital. Patients were included after written informed consent. Gender, age at inclusion in the study, age at diagnosis, clinical parameters and current and prior medication were derived from the clinical charts.
Since in The Netherlands treatment of RA is strictly aimed at achieving clinical remission, disease activity itself cannot be used as a marker for disease severity. For that reason it was chosen to use the need for therapy with anti-TNF as an alternative marker for disease severity. This can be done reliably since in the Netherlands the prescription of anti-TNF is strictly regulated and the costs for anti-TNF treatment are only reimbursed by the health insurance companies for RA-patients with therapy-resistant disease. Therapy-resistance is defined as failure of at least two disease-modifying anti-rheumatic drugs (DMARDs) including methotrexate, and still active disease (defined as DAS28 > 3.2) despite therapy with methotrexate 25 mg weekly or with methotrexate at the maximum tolerated dose. Blood was drawn for DNA isolation and routine laboratory analysis. Since the anti-CCP test has only recently been introduced into routine patient care, only for a minority of patients (n = 125) anti CCP status was known.
Caucasian controls representing the general adult population (n = 463) were derived from the Sanquin Blood Bank South West Region.
Experimental procedures
DNA isolation
For RA patients DNA isolation from heparinized whole blood was performed as described previously [36]. DNA from controls was derived from whole blood with column methods using standard protocols (Qiagen, Leusden, The Netherlands).
Genotyping
Single base extension (SBE) analysis was used to determine genotypes of inducible nitric oxide synthase (NOS2A) S608L (rs2297518), poly (ADP-ribose) polymerase (PARP) V762A (rs1136410), complement component inhibitor-1 (C1INH) V480 M (rs4926), PAI1 -675 4G/5G (rs1799889), IL4 C-524T (rs2243250), IL10 G-1082A (rs1800896), IL10 C-819T (rs3021097), IL1B C-31T (rs1143627), TNFA A-863C (rs1800630), TNFA T-857C (rs1799724), TNFA G-376A (rs3093659), TNFA G-308A (rs1800629), TNFA G-238A (rs361525), IL6 G-174C (rs1800795), IL8 C781T intron (rs2227306), TLR4 D299G (rs4986790) and TLR4 T399I (rs4986791) http://www.ncbi.nlm.nih.gov/SNP/, Applied Biosystems, SNaPShot, standard protocol as supplied by the manufacturer, Nieuwerkerk aan den IJssel, The Netherlands). The genomic region of interest was amplified by PCR (Additional file 1: Table S1, S2, and S3). After purification, a single base extension was performed using a primer ending one nucleotide prior to the single nucleotide polymorphism (SNP) location. Both forward and reverse strands were tested. In a multiplex assay one of the primers was used to genotype the SNP of interest. Up to seven SNPs were analysed in one assay. A poly-T-tail attached to the primer combined with the use of a Liz size marker served to distinguish SNPs in the multiplex analysis (Additional file 1: Table S4). A subset of PCR samples was sequenced to confirm genotypes. All genotypes were annotated independently by two investigators who were blinded for the clinical data.
Statistical analysis
Statistical analysis was performed using SPSS 11.5. Haplotype analysis was carried out with Thesias version 2 [37, 38]. Genotype frequencies were compared between patients with RA and controls using the Cochrane-Armitage trend test for additive effects. The median number of different drugs used per year since the moment of diagnosis was assessed. Additionally, genotype distributions between patients who received anti-TNF-α medication were compared with those who did not. Binomial variables were analysed using Pearson's chi-square test (2df) or Fisher's exact test when appropriate. For continuous variables Student's T test or Mann-Whitney U test were used when appropriate. Verification of Hardy Weinberg equilibrium (HWE) of genotypes was performed using Chi-square test (1df). Probability (P) values < 0.05 were considered to be statistically significant. Significant probability values obtained were corrected for multiple testing using Bonferroni for the number SNPs tested (n = 17) and the number of tests performed (n = 3). Power calculations using Quanto revealed a power of 0.8 to detect an OR of 1.5 comparing patients and controls given an allele frequency of 0.1 and α of 0.05 [39].
Results
Patient characteristics
376 patients, mean age (sd) 59.3 years (13.7) and 463 controls mean age (sd) 39.1 years (8.5), were included in the study (p < 0.001). In the patient and control cohort 277 (73.7%) and 230 (49.7%) individuals were female, respectively (p < 0.001). All patients were included when comparing RA patients with healthy controls. For 6 patients records regarding medication use were incomplete due to (multiple) transfers of patients from other hospitals. For this reason the 370 patients for whom medication data was complete were included in the analysis regarding disease severity (Table 1).
Genotypes and disease susceptibility
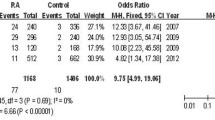
In controls, genotype distribution of all SNPs except the IL10 G-819A polymorphism reached Hardy Weinberg Equilibrium (HWE). To rule out a technical problem, an initial set of individuals was typed using both the reverse and forward primer in the single base extension reaction. Results for both strands were identical. Sequencing of a subset of 13 random controls showed identical genotypes excluding technical errors (data not shown). When Bonferroni correction is applied, none of the SNPs was significantly associated with RA susceptibility, adjusted for age and gender. Using the Cochrane-Armitage trend test for additive effects an association was observed for the TNFA -238 G/A polymorphisms (Bonferroni corrected p values 0.04). The TNFA-238 G/G genotype were overrepresented in RA patients when compared to controls (crude OR (95% CI) 2.48 (1.38-4.46) for TNFA G/G vs G/A; Table 2). Analysis of TNFA haplotypes yielded similar results as for the individual SNPs (data not shown). Since RA patients were significantly older than healthy controls and controls are by definition still 'at risk' to develop RA at a later age, the difference observed may also result from a difference in susceptibility to develop RA at a younger age. For this reason the relation of all SNPs with the age at diagnosis was analysed. The IL8 781 C/C genotype was associated with younger age at RA diagnosis compared to both the IL8 781 C/T and T/T genotype (mean age (SD): IL8 781 T/T 52.2 (14) years, T/C 50.0 (14) years and C/C 44.2 (13) years, respectively, p < 0.01, after Bonferroni correction; Table 3).
Genetic polymorphisms and severity of disease
The use of TNF-α modifying therapy was considered to be an indicator of severe disease in the Dutch situation as explained in the methods section. Anti-TNF-α drugs were administered to 120 of 370 patients. The mean age (sd) of patients who used anti-TNF-α was 55.7 (12.8) years compared with 60.8 (13.9) years in the group that did not receive anti-TNF-α (p = 0.001). Presence of anti CCP antibodies, RF or disease duration was not different between the two groups. In contrast, the presence of erosions, and the numbers of DMARDs used was differentially distributed between patients requiring anti-TNF treatment to obtain acceptable disease activity and those who did not (Table 1). Only a trend was observed for the TNFA -308 G/A polymorphism using the Cochrane-Armitage trend test for additive effects (p = 0.04, without Bonferroni correction). After adjustment for age and multiple testing, none of the polymorphisms was significantly associated with disease severity (Table 4).
Discussion
In our study the IL8 781 C/C genotype was associated with a younger age at RA diagnosis. Increased IL-8 expression was associated with RA when compared with osteoarthritis [40]. The IL8 C/T polymorphism was previously associated with viral infection, but no data are available on the effect of this intronic polymorphism on IL-8 expression. Recently a group in Taiwan published the IL-8 3'-UTR 2767AA genotype to be associated with younger age at onset [41]. The IL8 781C, IL8 276A and the IL8 -251T alleles appear to be in linkage disequilibrium [3]. The IL8 -251 T allele has previously been associated with respiratory syncytial virus infection in children, in whom also higher serum IL-8 levels were observed [3]. Given the role of IL-8 in promoting the pro-inflammatory response this could explain the association of IL8 polymorphisms with early onset of RA.
Only the TNFA -238 polymorphism was differentially distributed between RA patients and controls, even after Bonferroni correction. However, after adjustment for age and gender none remained significant. Using anti-TNF requirement as marker for severity a trend was observed for the TNFA -238 polymorphism. The findings for the TNFA-238 polymorphism match those reported for both a Mexican and a Colombian cohort [33, 35]. Additionally, in the Mexican cohort, the -308 A allele was associated with more severe disease, while it is also reported to be associated with erosion in RA patients [35, 42]. Moreover, carriage of the TNFA -308A allele, related to higher TNF-α production, was previously reported to be associated with non-response to anti-TNF-α in patients with different autoimmune diseases among which RA [43–45]. In the past numerous studies have been performed to investigate the association of TNFA promoter polymorphisms and TNF-α levels in different inflammatory and infectious diseases, reporting contradictory results [46]. TNF-α expression is probably not determined by one but by a combination of polymorphisms in TNFA and -associated genes. In our study, and in contrast to those described above, only the TNFA -238A allele showed a trend towards more severe disease (Table 3). It must however be noted that the allele frequency is very low and a slight difference in genotype distribution would markedly alter the results. Moreover, it is not unlikely that the observations for the TNFA polymorphisms result at least in part from linkage disequilibrium with the HLADRB1 locus, which was previously associated with RA [14, 15, 19].
No association of polymorphisms with disease severity was observed after correction for multiple testing. Many would argue that functional studies are preferred over genetic association studies. However, interpretation of RNA expression analyses is difficult due to the intra and inter-patient variation [47]. Careful sampling may overcome this problem and reduce the finding of false positive differentially expressed genes. With the exception of those studies assessing cytokine expression only in patients without DMARDs at diagnosis, results are likely to be influenced by the use of these DMARDs and disease progression. For this reason comparison of the results of different studies is limited. One can question whether therapy with anti-TNF is an appropriate marker for disease severity. In the modern era of aggressive treatment of RA medication is intensified till the goal of low disease activity or even remission is achieved. That disease activity was low is underscored by the low geometric mean ESR level in our cohort of RA-patients (16.2; 95% CI 14.7-17.7 mm/hr), that was not different (p = 0.17) between patients on conventional DMARDs (15.4; 95% CI 13.8-17.3 mm/hr) or those on biologicals (17.6; 95% CI 15.1-20.5 mm/hr). It was therefore decided not to use disease activity as marker of disease severity, but whether low disease activity could be achieved by conventional DMARDs or by use of biologicals directed against TNF. That therapy with a biological against TNF could be used as a marker of disease severity in this study is also due to the fact that its use is strictly regulated in the Netherlands; therapy with biologicals against TNF is available for all RA-patients that failed on two DMARDs and still have active disease (DAS28 > 3.2) despite therapy with methotrexate 25 mg weekly or at the maximal tolerated dose.
No association was observed for the IL10 polymorphisms with RA susceptibility or severity. Previously, contrasting results were reported for the role of IL10 polymorphisms in RA [48–50]. A recent study demonstrated a significant association between having RA and the IL10 1082 G allele (p = 0.008; OR = 1.44, 95% CI 1.11-1.86) [50]. Recently, a substantial improvement of RA upon treatment with anti-IL-6 receptor antibody [6]. The IL6 G/G genotype is associated with increased IL-6 levels compared to the C/C genotype, contributing to the complex regulation of IL-6 production [26, 51–53]. Furthermore, IL-6 expression in synovial tissue is higher in end-stage RA than in chronic active RA [54]. IL-6 expression is influenced by TNF-α, and interaction of polymorphisms in these and other genes may co-determine the disease phenotype. This interaction in combination with the limited sample size may have prohibited finding an association of the IL6 polymorphism with RA.
Although a polymorphism in TLR4 has previously been associated with rapid response to treatment in RA no association with RA was observed for the TLR4 polymorphisms in our study [55].
Recent GWAS studies on RA susceptibility included thousands of patients. We used a candidate gene approach in the SNP selection because this is a moderately sized population. Despite having a larger a priori chance of finding a true association if SNPs are associated with disease, this may have resulted in both false positive and false negative findings. The recent studies observed no larger effect size than an OR of approximately 1.3. This implies that our study is probably underpowered to detect loci with a modest effect, and that larger patient numbers are needed to gain further insight into the possible role of these genes in RA pathogenesis. Additionally, apart from the TNFA region, the identified genomic regions of interest in these GWAS study do not correspond to the location of the genes we selected. Nevertheless, although validation of our results in an independent cohort is required, the data presented here do remain valuable for meta-analysis.
Conclusions
In summary we here report an association between IL8 781 C/T polymorphism and a younger age of onset of RA. After correction for age (and gender), and multiple testing, none of the polymorphisms was associated with RA susceptibility or severity. This illustrates the need for additional larger studies to elucidate the contributing factor of polymorphisms in the susceptibility to and severity of RA. Carefully designed functional studies regarding expression of mRNA and protein levels in combination with genetic analyses are warranted to elucidate the contribution of polymorphisms to disease severity and will contribute to improving our knowledge on RA pathogenesis.
References
van den Berg WB: Arguments for interleukin 1 as a target in chronic arthritis. Ann Rheum Dis. 2000, 59 (Suppl 1): i81-84. 10.1136/ard.59.suppl_1.i81.
Zwerina J, Redlich K, Schett G, Smolen JS: Pathogenesis of rheumatoid arthritis: targeting cytokines. Ann N Y Acad Sci. 2005, 1051: 716-729. 10.1196/annals.1361.116.
Heinzmann A, Ahlert I, Kurz T, Berner R, Deichmann KA: Association study suggests opposite effects of polymorphisms within IL8 on bronchial asthma and respiratory syncytial virus bronchiolitis. J Allergy Clin Immunol. 2004, 114: 671-676. 10.1016/j.jaci.2004.06.038.
Rodenburg RJ, van Den Hoogen FH, Barrera P, van Venrooij WJ, van De Putte LB: Superinduction of interleukin 8 mRNA in activated monocyte derived macrophages from rheumatoid arthritis patients. Ann Rheum Dis. 1999, 58: 648-652. 10.1136/ard.58.10.648.
Harada A, Sekido N, Akahoshi T, Wada T, Mukaida N, Matsushima K: Essential involvement of interleukin-8 (IL-8) in acute inflammation. J Leukoc Biol. 1994, 56: 559-564.
Maini RN, Taylor PC, Szechinski J, Pavelka K, Broll J, Balint G, Emery P, Raemen F, Petersen J, Smolen J, et al: Double-blind randomized controlled clinical trial of the interleukin-6 receptor antagonist, tocilizumab, in European patients with rheumatoid arthritis who had an incomplete response to methotrexate. Arthritis Rheum. 2006, 54: 2817-2829. 10.1002/art.22033.
Joosten LA, Lubberts E, Helsen MM, Saxne T, Coenen-de Roo CJ, Heinegard D, van den Berg WB: Protection against cartilage and bone destruction by systemic interleukin-4 treatment in established murine type II collagen-induced arthritis. Arthritis Res. 1999, 1: 81-91. 10.1186/ar14.
Keystone E, Wherry J, Grint P: IL-10 as a therapeutic strategy in the treatment of rheumatoid arthritis. Rheum Dis Clin North Am. 1998, 24: 629-639. 10.1016/S0889-857X(05)70030-2.
Finnegan A, Grusby MJ, Kaplan CD, O'Neill SK, Eibel H, Koreny T, Czipri M, Mikecz K, Zhang J: IL-4 and IL-12 regulate proteoglycan-induced arthritis through Stat-dependent mechanisms. J Immunol. 2002, 169: 3345-3352.
Prots I, Skapenko A, Wendler J, Mattyasovszky S, Yone CL, Spriewald B, Burkhardt H, Rau R, Kalden JR, Lipsky PE, Schulze-Koops H: Association of the IL4R single-nucleotide polymorphism I50V with rapidly erosive rheumatoid arthritis. Arthritis Rheum. 2006, 54: 1491-1500. 10.1002/art.21832.
Kjoller L, Kanse SM, Kirkegaard T, Rodenburg KW, Ronne E, Goodman SL, Preissner KT, Ossowski L, Andreasen PA: Plasminogen activator inhibitor-1 represses integrin- and vitronectin-mediated cell migration independently of its function as an inhibitor of plasminogen activation. Exp Cell Res. 1997, 232: 420-429. 10.1006/excr.1997.3540.
Stefansson S, Lawrence DA: The serpin PAI-1 inhibits cell migration by blocking integrin alpha V beta 3 binding to vitronectin. Nature. 1996, 383: 441-443. 10.1038/383441a0.
Li J, Guo Y, Holmdahl R, Ny T: Contrasting roles of plasminogen deficiency in different rheumatoid arthritis models. Arthritis Rheum. 2005, 52: 2541-2548. 10.1002/art.21229.
Criswell LA, Gregersen PK: Current understanding of the genetic aetiology of rheumatoid arthritis and likely future developments. Rheumatology (Oxford). 2005, 44 (Suppl 4): iv9-iv13. 10.1093/rheumatology/kei054.
Gibert M, Balandraud N, Touinssi M, Mercier P, Roudier J, Reviron D: Functional categorization of HLA-DRB1 alleles in rheumatoid arthritis: the protective effect. Hum Immunol. 2003, 64: 930-935. 10.1016/S0198-8859(03)00186-1.
Tamiya G, Shinya M, Imanishi T, Ikuta T, Makino S, Okamoto K, Furugaki K, Matsumoto T, Mano S, Ando S, et al: Whole genome association study of rheumatoid arthritis using 27 039 microsatellites. Hum Mol Genet. 2005, 14: 2305-2321. 10.1093/hmg/ddi234.
Barton A, Thomson W, Ke X, Eyre S, Hinks A, Bowes J, Gibbons L, Plant D, Wilson AG, Marinou I, et al: Re-evaluation of putative rheumatoid arthritis susceptibility genes in the post-genome wide association study era and hypothesis of a key pathway underlying susceptibility. Hum Mol Genet. 2008, 17: 2274-2279. 10.1093/hmg/ddn128.
Barton A, Thomson W, Ke X, Eyre S, Hinks A, Bowes J, Plant D, Gibbons LJ, Wilson AG, Bax DE, et al: Rheumatoid arthritis susceptibility loci at chromosomes 10p15, 12q13 and 22q13. Nat Genet. 2008, 40: 1156-1159. 10.1038/ng.218.
Gregersen PK, Silver J, Winchester RJ: The shared epitope hypothesis. An approach to understanding the molecular genetics of susceptibility to rheumatoid arthritis. Arthritis Rheum. 1987, 30: 1205-1213. 10.1002/art.1780301102.
Hinks A, Worthington J, Thomson W: The association of PTPN22 with rheumatoid arthritis and juvenile idiopathic arthritis. Rheumatology (Oxford). 2006, 45: 365-368. 10.1093/rheumatology/kel005.
Orozco G, Hinks A, Eyre S, Ke X, Gibbons LJ, Bowes J, Flynn E, Martin P, Wilson AG, Bax DE, et al: Combined effects of three independent SNPs greatly increase the risk estimate for RA at 6q23. Hum Mol Genet. 2009, 18: 2693-2699. 10.1093/hmg/ddp193.
Stahl EA, Raychaudhuri S, Remmers EF, Xie G, Eyre S, Thomson BP, Li Y, Kurreeman FA, Zhernakova A, Hinks A, et al: Genome-wide association study meta-analysis identifies seven new rheumatoid arthritis risk loci. Nat Genet. 2010, 42: 508-514. 10.1038/ng.582.
Thomson W, Barton A, Ke X, Eyre S, Hinks A, Bowes J, Donn R, Symmons D, Hider S, Bruce IN, et al: Rheumatoid arthritis association at 6q23. Nat Genet. 2007, 39: 1431-1433. 10.1038/ng.2007.32.
Orozco G, Barton A: Update on the genetic risk factors for rheumatoid arthritis. Expert Rev Clin Immunol. 2010, 6: 61-75. 10.1586/eci.09.72.
Nakashima H, Miyake K, Inoue Y, Shimizu S, Akahoshi M, Tanaka Y, Otsuka T, Harada M: Association between IL-4 genotype and IL-4 production in the Japanese population. Genes Immun. 2002, 3: 107-109. 10.1038/sj.gene.6363830.
Fishman D, Faulds G, Jeffery R, Mohamed-Ali V, Yudkin JS, Humphries S, Woo P: The effect of novel polymorphisms in the interleukin-6 (IL-6) gene on IL-6 transcription and plasma IL-6 levels, and an association with systemic-onset juvenile chronic arthritis. J Clin Invest. 1998, 102: 1369-1376. 10.1172/JCI2629.
Dawson SJ, Wiman B, Hamsten A, Green F, Humphries S, Henney AM: The two allele sequences of a common polymorphism in the promoter of the plasminogen activator inhibitor-1 (PAI-1) gene respond differently to interleukin-1 in HepG2 cells. J Biol Chem. 1993, 268: 10739-10745.
Lockett KL, Hall MC, Xu J, Zheng SL, Berwick M, Chuang SC, Clark PE, Cramer SD, Lohman K, Hu JJ: The ADPRT V762A genetic variant contributes to prostate cancer susceptibility and deficient enzyme function. Cancer Res. 2004, 64: 6344-6348. 10.1158/0008-5472.CAN-04-0338.
Turner DM, Williams DM, Sankaran D, Lazarus M, Sinnott PJ, Hutchinson IV: An investigation of polymorphism in the interleukin-10 gene promoter. Eur J Immunogenet. 1997, 24: 1-8. 10.1111/j.1365-2370.1997.tb00001.x.
Chen H, Wilkins LM, Aziz N, Cannings C, Wyllie DH, Bingle C, Rogus J, Beck JD, Offenbacher S, Cork MJ, et al: Single nucleotide polymorphisms in the human interleukin-1B gene affect transcription according to haplotype context. Hum Mol Genet. 2006, 15: 519-529. 10.1093/hmg/ddi469.
Wen AQ, Wang J, Feng K, Zhu PF, Wang ZG, Jiang JX: Effects of haplotypes in the interleukin 1beta promoter on lipopolysaccharide-induced interleukin 1beta expression. Shock. 2006, 26: 25-30. 10.1097/01.shk.0000223125.56888.c7.
Hermans PW, Hibberd ML, Booy R, Daramola O, Hazelzet JA, de Groot R, Levin M: 4G/5G promoter polymorphism in the plasminogen-activator-inhibitor-1 gene and outcome of meningococcal disease. Meningococcal Research Group. Lancet. 1999, 354: 556-560. 10.1016/S0140-6736(99)02220-5.
Correa PA, Gomez LM, Cadena J, Anaya JM: Autoimmunity and tuberculosis. Opposite association with TNF polymorphism. J Rheumatol. 2005, 32: 219-224.
Hull J, Ackerman H, Isles K, Usen S, Pinder M, Thomson A, Kwiatkowski D: Unusual haplotypic structure of IL8, a susceptibility locus for a common respiratory virus. Am J Hum Genet. 2001, 69: 413-419. 10.1086/321291.
Rodriguez-Carreon AA, Zuniga J, Hernandez-Pacheco G, Rodriguez-Perez JM, Perez-Hernandez N, Montes de Oca JV, Cardiel MH, Granados J, Vargas-Alarcon G: Tumor necrosis factor-alpha -308 promoter polymorphism contributes independently to HLA alleles in the severity of rheumatoid arthritis in Mexicans. J Autoimmun. 2005, 24: 63-68. 10.1016/j.jaut.2004.11.002.
van de Geijn FE, Roos A, de Man YA, Laman JD, de Groot CJ, Daha MR, Hazes JM, Dolhain RJ: Mannose-binding lectin levels during pregnancy: a longitudinal study. Hum Reprod. 2007, 22: 362-371. 10.1093/humrep/del392.
Tregouet DA, Escolano S, Tiret L, Mallet A, Golmard JL: A new algorithm for haplotype-based association analysis: the Stochastic-EM algorithm. Ann Hum Genet. 2004, 68: 165-177. 10.1046/j.1529-8817.2003.00085.x.
Schaid DJ, Rowland CM, Tines DE, Jacobson RM, Poland GA: Score tests for association between traits and haplotypes when linkage phase is ambiguous. Am J Hum Genet. 2002, 70: 425-434. 10.1086/338688.
QUANTO 1.1: A computer program for power and sample size calculations for genetic-epidemiology studies. [http://hydra.usc.edu/gxe]
Klimiuk PA, Sierakowski S, Latosiewicz R, Skowronski J, Cylwik JP, Cylwik B, Chwiecko J: Histological patterns of synovitis and serum chemokines in patients with rheumatoid arthritis. J Rheumatol. 2005, 32: 1666-1672.
Lo SF, Huang CM, Lin HC, Chen WC, Tsai CH, Tsai FJ: Cytokine (IL-6) and chemokine (IL-8) gene polymorphisms among rheumatoid arthritis patients in Taiwan. Clin Exp Rheumatol. 2008, 26: 632-637.
Khanna D, Wu H, Park G, Gersuk V, Gold RH, Nepom GT, Wong WK, Sharp JT, Reed EF, Paulus HE, Tsao BP: Association of tumor necrosis factor alpha polymorphism, but not the shared epitope, with increased radiographic progression in a seropositive rheumatoid arthritis inception cohort. Arthritis Rheum. 2006, 54: 1105-1116. 10.1002/art.21750.
Balog A, Klausz G, Gal J, Molnar T, Nagy F, Ocsovszky I, Gyulai Z, Mandi Y: Investigation of the prognostic value of TNF-alpha gene polymorphism among patients treated with infliximab, and the effects of infliximab therapy on TNF-alpha production and apoptosis. Pathobiology. 2004, 71: 274-280. 10.1159/000080062.
Seitz M, Wirthmuller U, Moller B, Villiger PM: The -308 tumour necrosis factor-alpha gene polymorphism predicts therapeutic response to TNFalpha-blockers in rheumatoid arthritis and spondyloarthritis patients. Rheumatology (Oxford). 2006
Mugnier B, Balandraud N, Darque A, Roudier C, Roudier J, Reviron D: Polymorphism at position -308 of the tumor necrosis factor alpha gene influences outcome of infliximab therapy in rheumatoid arthritis. Arthritis Rheum. 2003, 48: 1849-1852. 10.1002/art.11168.
Bayley JP, Ottenhoff TH, Verweij CL: Is there a future for TNF promoter polymorphisms?. Genes Immun. 2004, 5: 315-329. 10.1038/sj.gene.6364055.
Lindberg J, Af Klint E, Ulfgren AK, Stark A, Andersson T, Nilsson P, Klareskog L, Lundeberg J: Variability in synovial inflammation in rheumatoid arthritis investigated by microarray technology. Arthritis Res Ther. 2006, 8: R47-10.1186/ar1903.
Martinez A, Pascual M, Pascual-Salcedo D, Balsa A, Martin J, de la Concha EG: Genetic polymorphisms in Spanish rheumatoid arthritis patients: an association and linkage study. Genes Immun. 2003, 4: 117-121. 10.1038/sj.gene.6363931.
Riyazi N, Kurreeman FA, Huizinga TW, Dekker FW, Stoeken-Rijsbergen G, Kloppenburg M: The role of interleukin 10 promoter polymorphisms in the susceptibility of distal interphalangeal osteoarthritis. J Rheumatol. 2005, 32: 1571-1575.
Ates O, Hatemi G, Hamuryudan V, Topal-Sarikaya A: Tumor necrosis factor-alpha and interleukin-10 gene promoter polymorphisms in Turkish rheumatoid arthritis patients. Clin Rheumatol. 2008, 27: 1243-1248. 10.1007/s10067-008-0893-1.
Schluter B, Raufhake C, Erren M, Schotte H, Kipp F, Rust S, Van AH, Assmann G, Berendes E: Effect of the interleukin-6 promoter polymorphism (-174 G/C) on the incidence and outcome of sepsis. Crit Care Med. 2002, 30: 32-37. 10.1097/00003246-200201000-00005.
Terry CF, Loukaci V, Green FR: Cooperative influence of genetic polymorphisms on interleukin 6 transcriptional regulation. J Biol Chem. 2000, 275: 18138-18144. 10.1074/jbc.M000379200.
Hegedus CM, Skibola CF, Bracci P, Holly EA, Smith MT: Screening the human serum proteome for genotype-phenotype associations: an analysis of the IL6 - 174G > C polymorphism. Proteomics. 2007, 7: 548-557. 10.1002/pmic.200600366.
Smeets TJ, Barg EC, Kraan MC, Smith MD, Breedveld FC, Tak PP: Analysis of the cell infiltrate and expression of proinflammatory cytokines and matrix metalloproteinases in arthroscopic synovial biopsies: comparison with synovial samples from patients with end stage, destructive rheumatoid arthritis. Ann Rheum Dis. 2003, 62: 635-638. 10.1136/ard.62.7.635.
Kuuliala K, Orpana A, Leirisalo-Repo M, Kautiainen H, Hurme M, Hannonen P, Korpela M, Mottonen T, Paimela L, Puolakka K, et al: Polymorphism at position +896 of the toll-like receptor 4 gene interferes with rapid response to treatment in rheumatoid arthritis. Ann Rheum Dis. 2006, 65: 1241-1243. 10.1136/ard.2006.055137.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2350/12/36/prepub
Acknowledgements
The Sanquin Blood Bank South West Region provided samples of healthy blood donors. We thank Peter Hermans PhD and Ronald de Groot PhD MD, Department of Pediatrics, Radboud University Nijmegen Medical Centre, Nijmegen, for critically reading the manuscript.
M. Emonts was funded by the Erasmus MC Revolving Fund Foundation (RF 2001/24). The funding body had no influence in study design; in the collection, analysis, and interpretation of data; in the writing of the manuscript; and in the decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
ME and RD designed the study, got medical ethical approval, were responsible for database management and wrote the manuscript; JH and JL participated in the study design; ME and JH-D performed the statistical analyses. LV isolated the DNA; CG-J performed the genotyping analysis; KH, JW and RD included patients and collected clinical data. All authors read and approved the final manuscript.
Electronic supplementary material
12881_2010_770_MOESM1_ESM.PDF
Additional file 1: Supplemental tables S1, S2, S3 and S4. Supplemental table S1. PCR primer sequences. Supplemental table S2. PCR conditions using 384 Tetrad PCR machine. Supplemental table S3. Touchdown protocols for PCR. Supplemental table S4. Primer sequences for SBE reactions. (PDF 15 KB)
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Emonts, M., Hazes, M.J., Houwing-Duistermaat, J.J. et al. Polymorphisms in genes controlling inflammation and tissue repair in rheumatoid arthritis: a case control study. BMC Med Genet 12, 36 (2011). https://doi.org/10.1186/1471-2350-12-36
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2350-12-36