
Abstract
Background
Clostridium difficile-associated disease (CDAD) is a serious nosocomial infection, however few studies have assessed CDAD outcome in the intensive care unit (ICU). We evaluated the epidemiology, clinical course and outcome of hospital-acquired CDAD in the critical care setting.
Methods
We performed a historical cohort study on 58 adults with a positive C. difficile cytotoxin assay result occurring in intensive care units.
Results
Sixty-two percent of patients had concurrent infections, 50% of which were bloodstream infections. The most frequently prescribed antimicrobials prior to CDAD were anti-anaerobic agents (60.3%). Septic shock occurred in 32.8% of CDAD patients. The in-hospital mortality was 27.6%. Univariate analysis revealed that SOFA score, at least one organ failure and age were predictors of mortality. Charlson score ≥3, gender, concurrent infection, and number of days with diarrhea before a positive C. difficile toxin assay were not significant predictors of mortality on univariate analysis. Independent predictors for death were SOFA score at infection onset (per 1-point increment, OR 1.40; CI95 1.13–1.75) and age (per 1-year increment, OR 1.10; CI95 1.02–1.19).
Conclusion
In ICU patients with CDAD, advanced age and increased severity of illness at the onset of infection, as measured by the SOFA score, are independent predictors of death.
Similar content being viewed by others

Background
Clostridium difficile is a major cause of antibiotic associated diarrhea and colitis [1]. The incidence of infection with this organism is increasing in hospitals worldwide, consequent to the widespread use of broad-spectrum antibiotics [2].
Hospital-acquired C. difficile disease is associated with not only antimicrobial use, but also advanced age, laxative use, proton pump inhibitors, antineoplastic chemotherapeutic agent use, renal insufficiency, and gastrointestinal surgery or procedures [3, 4].
Over the past several years, numerous reports have been published regarding CDAD in immunocompromised patients (bone marrow transplantation, solid organ transplantation, HIV infected patients and those with neutropenia), [5–9] as well as hospitalized patients in acute care medical wards [10].
The clinical and financial impact of nosocomial CDAD, as measured by the attributable cost and length of stay, is significant [11]. However few studies have assessed CDAD outcome in the intensive care unit (ICU) setting [12].
The purpose of this study was to evaluate the epidemiology, clinical course and outcome of hospital-acquired CDAD in the ICU setting.
Methods
Setting
The Virginia Commonwealth University Medical Center (VCUMC) is an 820-bed tertiary care facility in Richmond, Virginia. The hospital houses 9 intensive care units (ICUs), including pediatric ICUs and a burn unit. Approximately 30,000 patients are admitted annually. The study was approved by the VCUMC Institutional Review Board (IRB).
Study design
All ICU patients with a positive C. difficile toxin at VCU Medical Center from January 2002 to August 2005 were identified retrospectively using the electronic medical microbiology record. This was followed by a retrospective chart review. Each patient was only included once at the time of the first C. difficile result. Patients older than 18 years of age were included in the analysis. At study entry, we recorded patient age, gender, location (medical ICU or surgical ICU), predisposing clinical conditions on admission, and colonoscopy or surgical procedures for CDAD. Data on nosocomial infections were collected for 14 days following the date of the first positive C. difficile toxin result. Additionally, we collected data on the duration of diarrhea before and after diagnosis and treatment of CDAD. Antimicrobial exposure preceding the diagnosis of CDAD and the interruption of antimicrobial treatment due to CDAD were also collected. Colonization status with methicillin-resistant S. aureus (MRSA) and vancomycin-resistant enterococci (VRE) were identified by clinical cultures during the time of study. Adverse outcomes (organ failure and mortality) that occurred during the hospital stay were recorded. The clinical condition of each patient was classified daily according to systemic inflammatory response syndrome (SIRS) criteria [SIRS, sepsis, severe sepsis or septic shock] and SOFA scores from two days prior to the first positive stool C. difficile-toxin assay through 14 days afterwards [13, 14]. The Sequential Organ Failure Assessment (SOFA) score, assesses the incidence and severity of organ dysfunction in critically ill patients [14]. The severity of underlying disease preceding CDAD was classified using the Charlson weighted comorbidity index [15].
Definitions
We defined a CDAD case as a patient with a positive stool C. difficile cytotoxin assay result and diarrhea. Diarrhea was defined as a change in bowel habit with ≥3 unformed bowel movements per day for ≥2 days [10]. We defined treatment failure as recurrence of diarrhea plus an additional stool specimen positive for C. difficile toxin or a physician order for a second course of treatment for C. difficile. Concurrent infection detected during CDAD was defined according to Centers for Disease Control and Prevention (CDC) criteria [16]. P revious antibiotic treatment was defined as an antibiotic prescribed for at least 48 hours in the 60 days prior to CDAD. The SOFA score was used to assess disease severity [14]. Systemic Inflammatory Response Syndrome (SIRS) was defined as two or more of the following: (1) temperature >38°C or <36°C, (2) heart rate >90 beats per minute, (3) respiratory rate >20 breaths per minute or a PaCO2 <32 mmHg, or (4) white blood cell count >12 × 109/L or <4 × 109/L or the presence of more than 10% immature neutrophils.
The clinical condition of each patient with CDAD was classified daily as SIRS, sepsis, severe sepsis or septic shock using criteria previously published by the American College of Chest Physicians/Society of Critical Care Medicine (ACCP/SCCM) [13]. Sepsis was defined as SIRS associated with C. difficile-associated diarrhea. Sepsis associated with organ dysfunction, hypotension or systemic manifestations of hypoperfusion constituted severe sepsis. Septic shock was defined as sepsis associated with hypotension unresponsive to intravenous fluid challenge or the need for a vasopressor agent. The presence of organ system failure was assessed using the criteria described by Fagon [17]. Nosocomial infection was defined as an infection that occurred >48 hours after hospital admission, an infection that occurred <48 hours after admission to the hospital in patients that had been hospitalized in the 3 weeks prior to the admission, or an infection that occurred <48 hours after admission to the hospital in patients that had been transferred from another hospital or nursing home [16]. Treatment for CDAD was defined as the receipt of metronidazole at a dosage of 250 mg 4 times per day or 500 mg 3 times per day for 10–14 days, or oral vancomycin 125 mg 4 times per day for the same duration.
Statistical analysis
Continuous variables were compared using the Student t test for normally distributed variables and the Mann-Whitney U test for non-normally distributed variables. Differences in proportions were compared using a Chi-square test or Fisher exact test when appropriate. Alpha was set at 0.05 and all tests of significance were two-tailed. Variables significant for predicting mortality in univariate analysis were entered into a logistic regression model. When collinearity was identified between two variables in a correlation matrix, the one with the greatest clinical relevance associated with mortality was included in the final multivariate analysis. The Hosmer and Lemeshow goodness-of-fit statistic was used to assess adequacy of the model fit. Odds ratios with 95% confidence intervals were calculated for independent variables associated with mortality related to CDAD. All statistical analyses were done using the Statistical Package for the Social Sciences software (SPSS version 11.0, Chicago, IL, USA).
Results
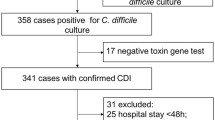
Study population and patient characteristics. From 613 hospitalized patients with CDAD, a total of 70 patients were identified at VCUMC ICUs during the study period. Sixty-three patients (90%) were adults and 7 were pediatric patients (10%). Of the adult patients, 5 (7.9%) had incomplete medical records. The remaining 58 adult ICU patients with CDAD were included in the analysis.
The median age was 55.5 years with an inter-quartile range (IQR) from 43 to 64 years. Twenty-two patients (37.9%) were over 60 years of age. The majority of patients were from surgical ICUs (63.8%). The most frequent admission diagnoses were trauma (22.4%), cardiovascular disease (20.7%), gastrointestinal diseases (17.2%) and solid and haematologic malignancies (12.1%). The mean interval between hospitalization and CDAD infection was 16.8 ± 18.5 days. The median duration of hospitalization was 32.0 days (IQR = 16.7–68.2). The mean duration of diarrhea before CDAD diagnosis was 6.5 ± 7.0 days. The majority of patients (93.1%) were receiving antimicrobial therapy before CDAD (Table 1). The most frequently prescribed antimicrobials prior to CDAD were anti-anaerobic agents considering piperacillin-tazobactam, metronidazole, carbapenems, or clindamycin (60.3%), quinolones (43.1%), and intravenous vancomycin (43.1%). Other prescribed antimicrobials were also cephalosporins (36.2%) and aminoglycosides (15.6%).
Sixty-two percent of patients (36/58) had a concurrent infection; of these 50% (18/36) were bloodstream infections (BSIs), a sizable fraction of which (39.9%, 11/18) were polymicrobial. The most frequent concurrent BSI pathogens BSI were gram-negative bacteria (35.0%), following by coagulase-negative staphylococci (20.0%), and Candida albicans (20.0%). Other isolated pathogens Enterococcus spp (15.0%), Streptococcus viridans (5.0%) and Candida glabrata (5.0%). No vancomycin-resistant enterococci were detected. In approximately thirty-nine percent of BSI patients (7/18), a 24 hours delay in the initiation of appropriate antimicrobial therapy was observed.
Nearly all patients (98.3%) with CDAD received metronidazole as the initial antimicrobial treatment. Five patients failed the first course of antimicrobial therapy (8.6%); of these, two were treated with a second course of metronidazole, one was treated with vancomycin and two patients received both drugs (Table 1). The majority of patients (84.5%) with CDAD received concurrent antimicrobial therapy; in 13 (22.4%) of these patients there was no evidence of another infection. Two patients (3.4%) underwent colonoscopy for CDAD, but no patients required operative management. Almost one-third of CDAD patients were colonized with MRSA or VRE (31.0%).
Clinical course
Septic shock occurred in 32.8% (19/58) of CDAD patients. The maximal SIR (severe sepsis, septic shock or death) occurred in 43.1% (25/58) during the 14 days following the first positive C. difficile toxin assay. No significant difference was observed in maximal SIR score between patients with CDAD only and those with concurrent nosocomial infection (31.8% vs. 50.0%, p = 0.17). A statistically significant difference in SOFA scores was observed between the survivors and non-survivors. The 14-day mortality was 17.2% (10/58) and the in-hospital mortality was 27.6% (16/58).
Univariate analysis revealed that SOFA score, septic shock, at least one organ failure (respiratory, cardiovascular, renal, hematologic and hepatic) and age were significant predictors of mortality (table 2). Charlson score ≥3, gender, other concurrent nosocomial infections, and days from start of diarrhea to start of treatment for CDAD were not significant predictors of mortality on univariate analysis. Variables significant for predicting mortality in univariate analysis (age, SOFA score and at least one organ failure) were entered into a logistic regression model (p < 0.05). Using this model, the following variables were independent predictors for death (table 3): SOFA score at CDAD infection onset (per 1-point increment; OR 1.40, CI95 1.13–1.75) and age (per year; OR 1.10, CI95 1.02–1.19).
Discussion
To better understand the epidemiology of CDAD infection in critically ill patients, we investigated its clinical course and outcome in the intensive care units of a tertiary care, academic medical center. Of the 58 ICU patients with C. difficile colitis in our cohort study, a significant proportion of these patients had concurrent infection (62.1%). The majority of the pathogens associated with nosocomial infections in our study cohort were gastrointestinal flora. This finding coupled with the relatively high proportion of bloodstream infections that were polymicrobial suggest that the inflammation and disruption of the colonic mucosa by CDAD provided a source of entry for organisms into the bloodstream. Of note, 60% of these patients had recently been treated with antimicrobials with significant activity against anaerobes, suggesting an important protective role that anaerobes may play in the intestinal flora. Similarly, disruption of the anaerobic gut flora has been shown to be a risk factor for VRE colonization [18], an epidemiologic finding that has been experimentally validated in an animal model [19].
As more than a half of our C. difficile patients were co-infected, findings predictably showed that a high proportion of ICU CDAD patients had a maximal SIR (severe sepsis, septic shock or death) during 14 days of follow-up. However, no statistically difference was observed in maximal SIR between patients with CDAD only those with CDAD and another infection (p = 0.17). One potential explanation for this observation may have been the delay in the introduction of specific antimicrobial therapy (metronidazole or oral vancomycin) for patients with CDAD. In our study, ICU patients were symptomatic with diarrhea on average for 6.5 days prior to microbiologic confirmation of the CDAD diagnosis and initiation of therapy. In our study cohort, no patients required surgical procedures as a result of CDAD. This is similar to another report in which 2.5% of patients required emergency colectomy [20].
Some studies have shown that treatment of CDAD with metronidazole may lead to poor outcomes [21, 22]. In our study it was not our purpose to determine the efficacy of metronidazole since we had multiple confounders such as a high rate of co-infection, and some patients died before completing metronidazole treatment. Almost one-fifth of our patients received antibiotics in the absence of evidence to suggest a concurrent infection. This observation is particularly important as prior reports suggest that unnecessary antibiotic use makes treatment of CDAD more difficult and potentially less efficacious [2, 3].
The crude mortality rate associated with C. difficile diarrhea in our ICU population was high (27.6%). Similarly, a prospective study at 12 Quebec hospitals of 1,073 patients with CDAD found a 30-day crude mortality rate of 24.8% independent of being ICU or non-ICU patients [23]. In this study, Loo et al. found that the age-specific incidence of CDAD increased markedly after the age of 50 years and the attributable mortality rate increased after the age of 60 years [23]. Pepin et al. have also found that advanced age (≥65 years) is a risk factor for recurrence of CDAD following treatment with metronidazole. By multivariate analysis, we demonstrated that for ICU patients with CDAD, advanced age and a high SOFA score were independent predictors of mortality. Prior studies have identified advanced age as a risk factor for CDAD [11, 24]. To our knowledge, no other studies have reported SOFA score as a predictor for mortality in ICU patients with CDAD.
The limitations of our study should be acknowledged. First, we performed a retrospective cohort study; second, we only evaluated patients during hospitalization. Thus, we cannot comment on long term follow-up, including relapse of diarrhea and mortality. Third, these findings were specific for an ICU population in a tertiary care medical center and thus may not be generalizable to a non-ICU population. Fourth, as this study lacked controls, we did not investigate risk factors for the development of CDAD in our ICU population. Lastly, the study had a small sample size thereby potentially resulting in a type II error at the time of univariate and multivariate analysis.
Conclusion
CDAD is a serious nosocomial infection in ICU patients. It is associated with a high mortality and a high rate of nosocomial co-infection. As such, the management of these infections remains challenging. In ICU patients with CDAD, advanced age and increased severity of illness at the onset of infection, as measured by the SOFA score, are independent predictors of death.
Key messages
CDAD is not an infrequent infection with an usually late diagnosis and therapy, and high potential comorbidity and mortality. Almost one-fifth of our patients received antibiotics in the absence of evidence to suggest a concurrent infection. Antibiotics are used in a indiscriminate way in ICU. This observation is particularly important as prior reports suggest that unnecessary antibiotic use makes treatment of CDAD more difficult and potentially less efficacious.
References
Kelly CP, Pothoulakis C, LaMont JT: Clostridium difficile colitis. N Engl J Med. 1994, 330: 257-262. 10.1056/NEJM199401273300406.
Gorbach SL: Antibiotics and Clostridium difficile. N Engl J Med. 1999, 341: 1690-1691. 10.1056/NEJM199911253412211.
Gerding DN, Johnson S, Peterson LR, Mulligan ME, Silva J: Clostridium difficile-associated diarrhea and colitis. Infect Control Hosp Epidemiol. 1995, 16: 459-477.
Al-Tureihi FI, Hassoun A, Wolf-Klein G, Isenberg H: Albumin, length of stay, and proton pump inhibitors: key factors in Clostridium difficile-associated disease in nursing home patients. J Am Med Dir Assoc. 2005, 6: 105-108. 10.1016/j.jamda.2005.01.003.
Chakrabarti S, Lees A, Jones SG, Milligan DW: Clostridium difficile infection in allogeneic stem cell transplant recipients is associated with severe graft-versus-host disease and non-relapse mortality. Bone Marrow Transplant. 2000, 26: 871-876. 10.1038/sj.bmt.1702627.
Bilgrami S, Feingold JM, Dorsky D, Edwards RL, Bona RD, Khan AM, Rodriguez-Pinero F, Clive J, Tutschka PJ: Incidence and outcome of Clostridium difficile infection following autologous peripheral blood stem cell transplantation. Bone Marrow Transplant. 1999, 23: 1039-1042. 10.1038/sj.bmt.1701773.
Keven K, Basu A, Re L, Tan H, Marcos A, Fung JJ, Starzl TE, Simmons RL, Shapiro R: Clostridium difficile colitis in patients after kidney and pancreas-kidney transplantation. Transpl Infect Dis. 2004, 6: 10-14. 10.1111/j.1399-3062.2004.00040.x.
Gorschluter M, Glasmacher A, Hahn C, Schakowski F, Ziske C, Molitor E, Marklein G, Sauerbruch T, Schmidt-Wolf IG: Clostridium difficile infection in patients with neutropenia. Clin Infect Dis. 2001, 33: 786-791. 10.1086/322616.
Pulvirenti JJ, Mehra T, Hafiz I, DeMarais P, Marsh D, Kocka F, Meyer PM, Fischer SA, Goodman L, Gerding DN, Weinstein RA: Epidemiology and outcome of Clostridium difficile infection and diarrhea in HIV infected inpatients. Diagn Microbiol Infect Dis. 2002, 44: 325-330. 10.1016/S0732-8893(02)00462-5.
Kyne L, Warny M, Qamar A, Kelly CP: Asymptomatic carriage of Clostridium difficile and serum levels of IgG antibody against toxin A. N Engl J Med. 2000, 342: 390-397. 10.1056/NEJM200002103420604.
Kyne L, Hamel MB, Polavaram R, Kelly CP: Health care costs and mortality associated with nosocomial diarrhea due to Clostridium difficile. Clin Infect Dis. 2002, 34: 346-353. 10.1086/338260.
Rotimi VO, Mokaddas EM, Jamal WY, Verghese TL, el-Din K, Junaid TA: Hospital-acquired Clostridium difficile infection amongst ICU and burn patients in Kuwait. Med Princ Pract. 2002, 11: 23-28. 10.1159/000048656.
American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference: Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Crit Care Med. 1992, 20: 864-874.
Vincent JL, de Mendonça A, Cantraine F, Moreno R, Takala J, Suter PM, Sprung CL, Colardyn F, Blecher S: Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: results of a multicenter, prospective study. Working group on "sepsis-related problems" of the European Society of Intensive Care Medicine. Crit Care Med. 1998, 26: 1793-800.
Charlson ME, Pompei P, Ales KL, MacKenzie CR: A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987, 40: 373-383. 10.1016/0021-9681(87)90171-8.
Garner JS, Jarvis WR, Emori TG, Horan TC, Hughes JM: CDC definitions for nosocomial infections. Am J Infect Control. 1988, 6: 128-140. 10.1016/0196-6553(88)90053-3.
Fagon JY, Chastre J, Novara A, Medioni P, Gibert C: Characterization of intensive care unit patients using a model based on the presence or absence of organ dysfunctions and/or infection: the ODIN model. Intensive Care Med. 1993, 19: 137-144. 10.1007/BF01720528.
Edmond MB, Ober JF, Weinbaum DL, Pfaller MA, Hwang T, Sanford MD, Wenzel RP: Vancomycin-resistant Enterococcus faecium bacteremia: risk factors for infection. Clin Infect Dis. 1995, 20: 1126-1133.
Pultz NJ, Stiefel U, Subramanyan S, Helfand MS, Donskey CJ: Mechanisms by which anaerobic microbiota inhibit the establishment in mice of intestinal colonization by vancomycin-resistant Enterococcus. J Infect Dis. 2005, 191: 949-956. 10.1086/428090.
Pépin J, Valiquette L, Cossette B: Mortality attributable to nosocomial Clostridium difficile-associated disease during an epidemic caused by a hypervirulent strain in Quebec. CMAJ. 2005, 173: 1037-1042.
Musher DM, Aslam S, Logan N, Nallacheru S, Bhaila I, Borchert F, Hamill RJ: Relatively poor outcome after treatment of Clostridium difficile colitis with metronidazole. Clin Infect Dis. 2005, 40: 1586-1590. 10.1086/430311.
Pepin J, Alary ME, Valiquette L, Raiche E, Ruel J, Fulop K, Godin D, Bourassa C: Increasing risk of relapse after treatment of Clostridium difficile colitis in Quebec, Canada. Clin Infect Dis. 2005, 40: 1591-1597. 10.1086/430315.
Loo VG, Poirier L, Miller MA, Oughton M, Libman MD, Michaud S, Bourgault AM, Nguyen T, Frenette C, Kelly M, Vibien A, Brassard P, Fenn S, Dewar K, Hudson TJ, Horn R, Rene P, Monczak Y, Dascal A: A predomantly clonal multi-institutional outbreak of Clostridium difficile-associated diarrhea with high morbidity and mortality. N Engl J Med. 2005, 353: 2442-2449. 10.1056/NEJMoa051639.
Andrews CN, Raboud J, Kassen BO, Enns R: Clostridium difficile-associated diarrhea: predictors of severity in patients presenting to the emergency department. Can J Gastroenterol. 2003, 17: 369-373.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2334/7/42/prepub
Acknowledgements
This work was supported by CAPES – Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (Brasília, Brazil).
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The author(s) declare that they have no competing interests.
Authors' contributions
ARM participated in the design of the study, collected the data and performed the statistical analysis. GMLB participated in the design of the study and performed the statistical analysis. RPW participated in the design of the study and coordination. MBE conceived of the study, and participated in its design and coordination. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Marra, A.R., Edmond, M.B., Wenzel, R.P. et al. Hospital-acquired Clostridium difficile-associateddisease in the intensive care unit setting: epidemiology, clinical course and outcome. BMC Infect Dis 7, 42 (2007). https://doi.org/10.1186/1471-2334-7-42
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2334-7-42