
Abstract
Background
Ambulatory consolidation chemotherapy for acute myeloid leukemia (AML) is frequently associated with bloodstream infections but the spectrum of bacterial pathogens in this setting has not been well-described.
Methods
We evaluated the emergence of bacteremias and their respective antibiotic susceptibility patterns in AML patients receiving ambulatory-based consolidation therapy. Following achievement of complete remission, 207 patients received the first cycle (C1), and 195 the second cycle (C2), of consolidation on an ambulatory basis. Antimicrobial prophylaxis consisted of ciprofloxacin, amoxicillin and fluconazole.
Results
There were significantly more positive blood cultures for E. coli in C2 as compared to C1 (10 vs. 1, p=0.0045); all E. coli strains for which susceptibility testing was performed demonstrated resistance to ciprofloxacin. In patients under age 60 there was a significantly higher rate of Streptococccus spp. bacteremia in C2 vs. C1; despite amoxicillin prophylaxis all Streptococcus isolates in C2 were sensitive to penicillin. Patients with Staphylococcus bacteremia in C1 had significantly higher rates of Staphylococcus bacteremia in C2 (p=0.009, OR=8.6).
Conclusions
For AML patients undergoing outpatient-based intensive consolidation chemotherapy with antibiotic prophylaxis, the second cycle is associated with higher rates of ciprofloxacin resistant E. coli, penicillin-sensitive Streptococcus bacteremias and recurrent Staphylococcus infections.
Similar content being viewed by others

Background
Intensive treatment for acute myeloid leukemia (AML) typically includes induction followed by 2–4 cycles of consolidation chemotherapy [1]. In recent years there has been a shift to outpatient-based AML consolidation therapy with a number of studies confirming the safety of this approach for selected patients [2–9].
In most centers ambulatory chemotherapy programs rely on the use of antimicrobial prophylaxis as a means of reducing infections. Recent Infectious Disease Society of America (IDSA) guidelines endorse the use of ciprofloxacin prophylaxis to reduce bacterial infections in high risk cancer patients receiving chemotherapy [10]. Despite prophylactic antibiotics 30-90% of ambulatory patients experience a fever and 20-90% of consolidation cycles are associated with hospitalizations [2, 4–6]. However, there are limited data on the characteristics of infectious complications in this setting. We have previously shown that infectious complications increase in the second cycle of ambulatory AML consolidation therapy resulting in greater need for intensive care unit (ICU) support and increased mortality [11]. As these findings may relate to breakthrough infections caused by the development of antibiotic resistant microbes despite prophylactic antibiotic use, we conducted a retrospective analysis evaluating the spectrum of microbiological isolates and their antibiotic resistance patterns in AML patients undergoing ambulatory-based consolidation chemotherapy.
Methods
Patients
All newly diagnosed AML patients at the Princess Margaret Hospital (PMH) who had achieved complete remission with frontline induction chemotherapy and proceeding to ambulatory-based consolidation chemotherapy from October 2002 - February 2008 were included in the analysis. Eligibility requirements were as previously described [11]. Patients received the second consolidation cycle following peripheral count recovery from the first cycle and resolution of any previous bacterial infections. Prior approval for the study was obtained from the Cancer Registry Data Access Committee and Research Ethics Board of the University Health Network, Toronto, Ontario.
Chemotherapy regimens and supportive care
Ambulatory chemotherapy, subsequent monitoring and supportive care were provided as previously described [11] either in the ambulatory care area of the PMH or a local community hospital/clinic. Patients under age 60 (younger cohort) received two cycles of consolidation therapy (C1 and C2), each consisting of high dose cytarabine (HiDAC) 3 grams/m2 IV q12 hours × 6 doses on days 1, 3, and 5, plus daunorubicn 45 mg/m2 IV daily on days 1 and 2. For patients over age 60 (older cohort), C1 consisted of daunorubicin 60 mg/m2 IV daily × 3 plus cytarabine 100 mg/m2 as a 7-day continuous infusion via ambulatory infusion pump and C2 consisted of mitoxantrone 10 mg/m2 IV plus etoposide 100 mg/m2 IV, each given once daily from days 1–5.
During induction therapy patients received antimicrobial prophylaxis with fluconazole 400 mg PO daily whereas during consolidation they received ciprofloxacin 500 mg PO q12 hours, amoxicillin 500 mg PO q8 hours and fluconazole 400 mg PO daily, starting on Day 8 of the chemotherapy cycle and continuing until absolute neutrophil count (ANC) > 0.5 × 109/L. All chemotherapy, transfusions and IV antibiotics were administered via central venous catheters (CVC), usually double lumen Hickman lines placed prior to the start of induction chemotherapy.
Patients presenting with fever or clinical features of an infection had blood cultures drawn from all CVC ports, a peripheral vein and any other accessible sites suspected of being infected. As per institutional policy, empiric antibiotics for febrile neutropenia most commonly consisted of pipracillin/tazobactam 4.5 grams IV q8 hours plus tobramycin 5 mg/kg IV q24 hours. Febrile patients with suspected CVC involvement i.e. those with erythema, pain or purulent drainage at the insertion site, were started on vancomycin 1 gram IV q12 hours. Empiric therapy was adjusted based upon the results of culture and sensitivity testing. Antimicrobials were continued until microbiological and clinical evidence of infection had resolved and the ANC was > 0.5 × 109/L. Hematopoietic growth factors were not routinely used but were administered at the physician’s discretion from day 16–18 until neutrophil recovery. Patients with blood cultures positive for coagulase negative staphylococci (CNST) usually retained their CVC whereas patients with candidemia, tunnel infections or those with persistently positive cultures beyond 72 hours had their CVC replaced.
Cultures were processed using standard microbiological methods. Antibiotic susceptibilities were performed and reported by the Department of Microbiology of the Mount Sinai Hospital/University Health Network (Toronto, Ontario) or the local community hospital (if the site of the patient’s initial presentation) using predefined criteria. Antibiotic sensitivity data were not available in some cases where patients presented to local community hospitals.
Definitions
Blood cultures were considered positive if one or more culture bottles showed growth, regardless of the organism, with symptoms compatible with an infection. Bacteremias related to common contaminants such as CNST, Micrococcus., Propionibacterium or Bacillus spp. were treated with a full course of antibiotics; thus no distinction was made between contaminants and true pathogens. Cultures were considered polymicrobial if at least two different organisms were isolated. Repeated cultures in persistently febrile patients yielding the same organism with the same antibiotic susceptibility profile were considered as one isolate unless separated by one or more negative blood cultures.
Statistical analysis
Descriptive statistics were used to describe patient characteristics and outcome recordings. Categorical variables were expressed as count and proportions whereas continuous variables were expressed as means. Pearson Chi-square or Fisher’s exact test, when applicable, were used when comparing rates of infection and readmission. Results were considered significant if two-tailed P was < 0.05. Statistical Analysis Software (SAS, version 9.2; SAS Institute Inc., Cary NC) was used for statistical analysis.
Results
Patient characteristics
The characteristics of the patients receiving ambulatory-based consolidation chemotherapy have been previously described [11], and are summarized in Table 1. There was no significant difference in the median age of patients between C1 and C2; 54.6% of patients in C1 and 52.3% in C2 were male and the proportion of patients age ≥ 60 was 30% in C1 and 33% in C2 (p=NS).
Bacteremia during ambulatory chemotherapy
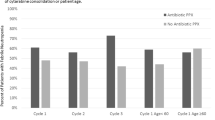
Microbiologically documented episodes of bacteremia are shown in Table 1. As we previously reported, the ambulatory cohort in C2 had significantly higher rates of positive blood cultures and bloodstream infection relative to C1 [11]. Most patients had only a single positive blood culture (86% in C1 and 90% in C2) with greater than 90% of cultures in each cycle being monomicrobial. In each consolidation cycle significantly more patients had a gram-positive bacterial infection as compared to gram-negative infections. The proportion of gram positive vs. gram negative isolates was not significantly different in C1 as compared to C2. Approximately 30% of patients presented to local community hospitals, where the source of the positive blood culture (CVC vs. peripheral) was not identified; we were therefore unable to determine the extent of CVC related bacteremias in these cases.
As shown in Table 1, CNST were the most common gram positive isolates during both cycles. Streptococci constituted 17% (9/53) of the total isolates in C1 and 23.9% (17/71) of the total isolates in C2 (p=0.35). Younger patients had a significantly higher incidence of streptococcal bacteremia in C2 relative to C1 (11.2% vs. 4.3%, p=0.033), and in these patients streptococci represented a greater proportion of the total isolates in C2 (34%, 15/44 isolates) relative to C1 (15%, 6/40 isolates, p=0.044).
Gram negative organisms were identified in 5.6% of patients in C1 vs. 10.7% of those in C2 (p=0.07). The frequency of E. coli isolates was significantly higher in C2 relative to C1 (5.4% vs. 0.5%, p=0.005) with E. coli constituting 14.1% (10/71) of all isolates in C2 and 1.9% (1/53) of those in C1 (p=0.023). This trend was observed in both the younger (0 in C1 vs. 4 in C2) and older (1 in C1 vs. 6 in C2) cohorts. In addition, there was no difference in the incidence of E. coli bacteremia in younger versus older patients within C1 (p=0.827) or C2 (p=0.8). The proportion of patients with non-E. coli gram negative isolates did not differ between C1 and C2 (5.1% vs. 5.3%, p=0.91).
Antibiotic resistance patterns
Table 2 highlights the antibiotic resistance patterns for selected organisms. Only one of the CNST with antibiotic sensitivity data was resistant to vancomycin while virtually all isolates were resistant to cloxacillin. All Streptococcus spp. isolates with susceptibility data exhibited sensitivity to penicillin. Among the non- E. coli gram-negative isolates, there was no difference in rates of ciprofloxacin resistance between C1 and C2 (1/9 vs. 0/7, p=1.0). In contrast, all E. coli isolates (8/8) from patients in C2 for which susceptibilities were available were ciprofloxacin resistant.
As shown in Table 2, most gram negative isolates in C1 and C2 were sensitive to the commonly used empiric antibiotics for febrile neutropenia in our institution, piperacillin/tazobactam and aminoglycosides. However, tobramycin resistance was noted in 67% (4/6) of the E. coli isolates, including 3/5 isolates from patients in C2.
Infection-related mortality
Overall, 9 patients died due to infectious complications while receiving ambulatory chemotherapy, one patient during C1 and 8 during C2. CNST were isolated from one such patient during C2 whereas Streptococcus spp. was isolated from two patients who died (one each in C1 and C2). The single Streptococcus isolate with available antibiotic susceptibility information was sensitive to penicillin and vancomycin. Gram negative organisms were isolated in 6 of the 8 patient deaths in C2: Klebsiella spp. (3 cases), E. coli (2) and Pseudomonas spp. (1, urine isolate). Both E. coli isolates were resistant to ciprofloxacin and tobramycin and displayed sensitivity only to piperacillin/tazobactam. Mortality amongst patients with ciprofloxacin resistant gram-negative bacteremias was 20% (2/10) versus 13.3% (2/15) for those with ciprofloxacin sensitive strains (p=1.0).
Effect of previous positive cultures/hospitalization
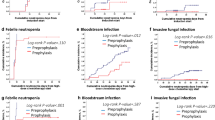
Approximately 51% of patients with a positive blood culture in C1 had a subsequent positive culture in C2 while only 27% of those with negative blood cultures in C1 had a positive culture in C2 (OR=2.8, p=0.005). This trend was significant for gram-positive organisms (OR=3.25, p=0.004) but not for gram-negative organisms (OR=2.1, p=0.31). An infection with Staphylococcal isolates in C1 was associated with the highest recurrence rates in C2 but only for patients age <60 (OR=8.6, p=0.009). No such association was seen for Streptococcal isolates or in the older cohort.
Discussion
Recent data suggest that ambulatory chemotherapy for AML patients can reduce the incidence of septicemia [7]. However, published data on the characteristics of microbiological isolates from patients receiving ambulatory chemotherapy remains limited [2–7, 9]. Our study, focusing on bacterial bloodstream infections, represents the largest reported series on AML patients receiving ambulatory-based intensive consolidation chemotherapy. We have previously shown that the rate of positive blood cultures increases following the second consolidation cycle [11] and the current study highlights potential explanations for the observed increase.
Despite the isolation of ciprofloxacin resistant E. coli in febrile neutropenic patients receiving fluoroquinolone prophylaxis [7, 12, 13] their use in high risk patients receiving chemotherapy has been supported by large randomized clinical trials and meta-analysis [14–17]. Within our cohort we observed an increased incidence of gram-negative bacteremia and ciprofloxacin resistance as patients transitioned from C1 to C2. Ciprofloxacin resistance was observed in 100% of the E. coli strains in C2, was rarely seen in Pseudomonas spp (1/4 in C1) and was not observed in the remaining Enterobacteriaceae (0/5 in C1 and 0/7 in C2). The preferential development of resistance among E. coli strains has been previously reported [18–20]. Cometta et al. noted that, among a cohort of patients receiving prophylactic fluoroquinolones, 28% of the E. Coli isolates were fluoroquinolone resistant while > 90% of the P. aeruginosa and K. pneumoniae isolates remained fluoroquinolone sensitive [18]. Kern et al. postulated the decreased virulence of fluoroquinolone resistant P. aeruginosa as one explanation for this phenomenon [20]. Prolonged exposure to subtherapeutic concentrations of antibiotics has been associated with the development of antibiotic resistance [21, 22]. It is possible that decreased absorption of fluoroquinolones in the setting of chemotherapy-induced mucositis, may have prevented reaching the mutant prevention concentration [23, 24] for E. coli in our cohort. We were unable to determine whether there was an emergence of resistance to other antibiotics, although the frequency of E. coli aminoglycoside resistance in C2 (4/6 cases) is concerning.
The effects of discontinuing prophylactic fluoroquinolones have been investigated in a number of studies. Reuter et al. prematurely stopped a trial of levofloxacin discontinuation due to a significant increase in infection-related mortality [25] and Kern et al. noted increased rates of bacteremia and a trend toward increased mortality during a period in which fluoroquinolone prophylaxis was discontinued [12]. A similar increase in bloodstream infections with fluoroquinolone susceptible isolates was seen when fluoroquinolone prophylaxis was discontinued by two Japanese groups although no effects on mortality were noted [26, 27]. Thus, although the emergence of ciprofloxacin resistance organisms calls into question the value of ciprofloxacin prophylaxis, current evidence and IDSA guidelines support its use in high-risk patients with prolonged (≥ 7 days) and profound neutropenia (≤100 cells/mm3) [10].
The increased use of fluoroquinolone prophylaxis and indwelling CVC’s has led to gram-positive organisms as the main cause of bacteremia in immunocompromised patients [4, 6, 7, 28]. In our cohort gram-positive organisms constituted 79% of the isolates during C1 and 70% in C2. As some of our patients were followed in community hospitals, we were unable to accurately determine which isolates were CVC related although we speculate that most CNST were of CVC origin. Consistent with previous reports [2, 6, 7, 28, 29], CNST and Streptococcus spp. were the most common gram positive organisms. The rate of CNST isolates was not statistically different between C1 and C2, however, Streptococcus isolates, particularly S. viridans, increased from C1 to C2 within the younger cohort, likely reflecting the cumulative effects of HiDAC chemotherapy [11, 28, 30–32].
As a high frequency of S. viridans infections is a well-documented effect associated with ciprofloxacin prophylaxis [12], patients within our cohort were administered amoxicillin during the neutropenic period. Surprisingly, however, all Streptococcus isolates with susceptibility data were found to be penicillin sensitive. Poor compliance with amoxicillin dosing or prior CVC colonization may provide a potential explanation for this observation. Although current IDSA guidelines recommend against the addition of gram-positive coverage to fluoroquinolone prophylaxis, studies have suggested that it may be beneficial in patients at high risk of streptococcal infections including those with severe neutropenia, oral mucositis, bone marrow transplantation and those receiving HiDAC-based chemotherapy [33]. From our data, it is unclear if the addition of amoxicillin alone resulted in any substantial benefit; delineation of this would require a prospective randomized study.
An important finding in our study, not previously described, is the increased rate of positive blood cultures in C2 in patients with previous positive cultures in C1. This effect was restricted to Staphylococcus spp. in younger patients and may reflect the prolonged use of indwelling catheters. The inadequate activity of ciprofloxacin and amoxicillin against these organisms likely further contributed to their increased pathogenicity [14, 29]. It is possible that CVC replacement between consolidation cycles in patients previously positive for Staphylococcus spp. could reduce their recurrence rates, but this requires further study.
Our data have several limitations. This was a retrospective analysis conducted at a single tertiary care cancer center and it is unclear whether results are generalizable to other centers or with different regimens. Second, our rates of gram-positive bacteremia may have been overestimated as we could not always accurately differentiate whether isolates represented true bacteremia, CVC colonization or contamination. However, given the context of fever in high-risk neutropenic patients, all of whom were treated empirically with IV antibiotics, infection is more likely. Furthermore, as some patients were treated in community hospitals, we had incomplete information regarding antibiotic sensitivities.
Conclusions
In summary, our findings emphasize the limitations of antibacterial prophylaxis of AML patients post-chemotherapy in the ambulatory setting, particularly in later cycles following prolonged use of fluoroquinolones and indwelling central venous catheters. Clinicians should be cognizant of the resulting increased predilection to fluoroquinolone-resistant E. coli, streptococcal spp. and recurrent CNST infections, and additional prophylactic measures should be considered in these patients.
References
Tallman MS: New strategies for the treatment of acute myeloid leukemia including antibodies and other novel agents. Hematology Am Soc Hematol Educ Program. 2005, 143-150.
Girmenia C, Alimena G, Latagliata R, Morano SG, Celesti F, Coppola L, Spadea A, Tosti S, Mecarocci S, D'Elia GM, et al: Out-patient management of acute myeloid leukemia after consolidation chemotherapy. Role of a hematologic emergency unit. Haematologica. 1999, 84 (9): 814-819.
Gillis S, Dann EJ, Rund D: Selective discharge of patients with acute myeloid leukemia during chemotherapy-induced neutropenia. Am J Hematol. 1996, 51 (1): 26-31. 10.1002/(SICI)1096-8652(199601)51:1<26::AID-AJH5>3.0.CO;2-9.
Eisele L, Gunther F, Ebeling P, Nabring J, Duhrsen U, Durig J: Outpatient management of acute myeloid leukemia after intensive consolidation chemotherapy is feasible and reduces hospital treatment costs. Onkologie. 2010, 33 (12): 658-664. 10.1159/000322209.
Savoie ML, Nevil TJ, Song KW, Forrest DL, Hogge DE, Nantel SH, Shepherd JD, Smith CA, Sutherland HJ, Toze CL, et al: Shifting to outpatient management of acute myeloid leukemia: a prospective experience. Ann Oncol. 2006, 17 (5): 763-768. 10.1093/annonc/mdl011.
Moller T, Nielsen OJ, Welinder P, Dunweber A, Hjerming M, Moser C, Kjeldsen L: Safe and feasible outpatient treatment following induction and consolidation chemotherapy for patients with acute leukaemia. Eur J Haematol. 2010, 84 (4): 316-322. 10.1111/j.1600-0609.2009.01397.x.
Halim TY, Song KW, Barnett MJ, Forrest DL, Hogge DE, Nantel SH, Nevill TJ, Shepherd JD, Smith CA, Sutherland HJ, et al: Positive impact of selective outpatient management of high-risk acute myelogenous leukemia on the incidence of septicemia. Ann Oncol. 2007, 18 (7): 1246-1252. 10.1093/annonc/mdm112.
Allan DS, Buckstein R, Imrie KR: Outpatient supportive care following chemotherapy for acute myeloblastic leukemia. Leuk Lymphoma. 2001, 42 (3): 339-346. 10.3109/10428190109064590.
Ruiz-Arguelles GJ, Apreza-Molina MG, Aleman-Hoey DD, Gomez-Almaguer D, Marin-Lopez A, Mercado-Diaz L: Outpatient supportive therapy after induction to remission therapy in adult acute myelogenous leukaemia (AML) is feasible: a multicentre study. Eur J Haematol. 1995, 54 (1): 18-20.
Freifeld AG, Bow EJ, Sepkowitz KA, Boeckh MJ, Ito JI, Mullen CA, Raad II, Rolston KV, Young JA, Wingard JR, et al: Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 Update by the Infectious Diseases Society of America. Clin Infect Dis. 2011, 52 (4): 427-431. 10.1093/cid/ciq147.
Saini L, Minden MD, Schuh AC, Yee KW, Schimmer AD, Gupta V, Atenafu EG, Murray C, Nixon S, Brandwein JM: Feasibility of outpatient consolidation chemotherapy in older versus younger patients with acute myeloid leukemia. Am J Hematol. 2012, 87 (3): 323-326. 10.1002/ajh.22268.
Kern WV, Klose K, Jellen-Ritter AS, Oethinger M, Bohnert J, Kern P, Reuter S, von Baum H, Marre R: Fluoroquinolone resistance of Escherichia coli at a cancer center: epidemiologic evolution and effects of discontinuing prophylactic fluoroquinolone use in neutropenic patients with leukemia. Eur J Clin Microbiol Infect Dis. 2005, 24 (2): 111-118. 10.1007/s10096-005-1278-x.
van Belkum A, Goessens W, van der Schee C, Lemmens-den Toom N, Vos MC, Cornelissen J, Lugtenburg E, de Marie S, Verbrugh H, Lowenberg B, et al: Rapid emergence of ciprofloxacin-resistant enterobacteriaceae containing multiple gentamicin resistance-associated integrons in a Dutch hospital. Emerg Infect Dis. 2001, 7 (5): 862-871.
Bucaneve G, Micozzi A, Menichetti F, Martino P, Dionisi MS, Martinelli G, Allione B, D'Antonio D, Buelli M, Nosari AM, et al: Levofloxacin to prevent bacterial infection in patients with cancer and neutropenia. N Engl J Med. 2005, 353 (10): 977-987. 10.1056/NEJMoa044097.
Cullen M, Steven N, Billingham L, Gaunt C, Hastings M, Simmonds P, Stuart N, Rea D, Bower M, Fernando I, et al: Antibacterial prophylaxis after chemotherapy for solid tumors and lymphomas. N Engl J Med. 2005, 353 (10): 988-998. 10.1056/NEJMoa050078.
Leibovici L, Paul M, Cullen M, Bucaneve G, Gafter-Gvili A, Fraser A, Kern WV: Antibiotic prophylaxis in neutropenic patients: new evidence, practical decisions. Cancer. 2006, 107 (8): 1743-1751. 10.1002/cncr.22205.
Gafter-Gvili A, Fraser A, Paul M, Leibovici L: Meta-analysis: antibiotic prophylaxis reduces mortality in neutropenic patients. Ann Intern Med. 2005, 142 (12 Pt 1): 979-995.
Cometta A, Calandra T, Bille J, Glauser MP: Escherichia coli resistant to fluoroquinolones in patients with cancer and neutropenia. N Engl J Med. 1994, 330 (17): 1240-1241. 10.1056/NEJM199404283301717.
Cattaneo C, Quaresmini G, Casari S, Capucci MA, Micheletti M, Borlenghi E, Signorini L, Re A, Carosi G, Rossi G: Recent changes in bacterial epidemiology and the emergence of fluoroquinolone-resistant Escherichia coli among patients with haematological malignancies: results of a prospective study on 823 patients at a single institution. J Antimicrob Chemother. 2008, 61 (3): 721-728. 10.1093/jac/dkm514.
Kern WV, Steib-Bauert M, de With K, Reuter S, Bertz H, Frank U, von Baum H: Fluoroquinolone consumption and resistance in haematology-oncology patients: ecological analysis in two university hospitals 1999–2002. J Antimicrob Chemother. 2005, 55 (1): 57-60.
Brown NM, White LO, Blundell EL, Chown SR, Slade RR, MacGowan AP, Reeves DS: Absorption of oral ofloxacin after cytotoxic chemotherapy for haematological malignancy. J Antimicrob Chemother. 1993, 32 (1): 117-122. 10.1093/jac/32.1.117.
Johnson EJ, MacGowan AP, Potter MN, Stockley RJ, White LO, Slade RR, Reeves DS: Reduced absorption of oral ciprofloxacin after chemotherapy for haematological malignancy. J Antimicrob Chemother. 1990, 25 (5): 837-842. 10.1093/jac/25.5.837.
Epstein BJ, Gums JG, Drlica K: The changing face of antibiotic prescribing: the mutant selection window. Ann Pharmacother. 2004, 38 (10): 1675-1682. 10.1345/aph.1E041.
Rybak MJ: Pharmacodynamics: relation to antimicrobial resistance. Am J Med. 2006, 119 (6 Suppl 1): S37-44. discussion S62-70
Reuter S, Kern WV, Sigge A, Dohner H, Marre R, Kern P, von Baum H: Impact of fluoroquinolone prophylaxis on reduced infection-related mortality among patients with neutropenia and hematologic malignancies. Clin Infect Dis. 2005, 40 (8): 1087-1093. 10.1086/428732.
Saito T, Yoshioka S, Iinuma Y, Takakura S, Fujihara N, Ichinohe T, Ishikawa T, Uchiyama T, Ichiyama S: Effects on spectrum and susceptibility patterns of isolates causing bloodstream infection by restriction of fluoroquinolone prophylaxis in a hematology-oncology unit. Eur J Clin Microbiol Infect Dis. 2008, 27 (3): 209-216. 10.1007/s10096-007-0428-8.
Chong Y, Yakushiji H, Ito Y, Kamimura T: Clinical impact of fluoroquinolone prophylaxis in neutropenic patients with hematological malignancies. International journal of infectious diseases: IJID: official publication of the International Society for Infectious Diseases. 2011, 15 (4): e277-281. 10.1016/j.ijid.2010.12.010.
Cannas G, Pautas C, Raffoux E, Quesnel B, Botton SD, Revel TD, Reman O, Gardin C, Elhamri M, Boissel N, et al: Infectious complications in adult acute myeloid leukemia: analysis of the Acute Leukemia French Association-9802 prospective multicenter clinical trial. Leuk Lymphoma. 2012, 53 (6): 1068-1076. 10.3109/10428194.2011.636812.
Madani TA: Clinical infections and bloodstream isolates associated with fever in patients undergoing chemotherapy for acute myeloid leukemia. Infection. 2000, 28 (6): 367-373. 10.1007/s150100070007.
Bakhshi S, Singh P, Swaroop C: Outpatient consolidation chemotherapy in pediatric acute myeloid leukemia: a retrospective analysis. Hematology. 2009, 14 (5): 255-260. 10.1179/102453309X446144.
Engelhard D, Elishoov H, Or R, Naparstek E, Nagler A, Strauss N, Cividalli G, Aker M, Ramu N, Simhon A, et al: Cytosine arabinoside as a major risk factor for Streptococcus viridans septicemia following bone marrow transplantation: a 5-year prospective study. Bone Marrow Transplant. 1995, 16 (4): 565-570.
Okamoto Y, Ribeiro RC, Srivastava DK, Shenep JL, Pui CH, Razzouk BI: Viridans streptococcal sepsis: clinical features and complications in childhood acute myeloid leukemia. J Pediatr Hematol Oncol. 2003, 25 (9): 696-703. 10.1097/00043426-200309000-00005.
Cruciani M, Malena M, Bosco O, Nardi S, Serpelloni G, Mengoli C: Reappraisal with meta-analysis of the addition of Gram-positive prophylaxis to fluoroquinolone in neutropenic patients. J Clin Oncol. 2003, 21 (22): 4127-4137. 10.1200/JCO.2003.01.234.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2334/13/284/prepub
Acknowledgements
We gratefully acknowledge the support of the various nurses and physicians involved in the care of the AML patients both at the PMH and the various local hospitals in and around the greater Toronto area.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
All authors declare that they have no competing interests.
Authors’ contributions
LS performed the research and drafted the manuscript. CR revised the manuscript. EGA performed the statistical analysis. JMB participated in the study deign and revised the manuscript. All authors read and approved the final manuscript.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Saini, L., Rostein, C., Atenafu, E.G. et al. Ambulatory consolidation chemotherapy for acute myeloid leukemia with antibacterial prophylaxis is associated with frequent bacteremia and the emergence of fluoroquinolone resistant E. Coli. BMC Infect Dis 13, 284 (2013). https://doi.org/10.1186/1471-2334-13-284
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2334-13-284