
Abstract
Background
The detection of serum tumor marker becomes a common method for screening tumors. However, this method has not been widely used for routine gastric cancer screening. In this study we aimed to determine whether the combined use of tumor markers may increase the sensitivity for the diagnosis of gastric cancer.
Methods
Serum AFP, CEA, CA125 and CA19-9 levels were measured in 149 patients with gastric cancer, 111 patients with benign gastric diseases and 124 healthy people, who visited the First Affiliated Hospital of Nanchang University from May 2011 to May 2012. Statistical analysis including receiver operating characteristic (ROC) curve, the area under the curve (AUC), and logistic regression analysis was performed to evaluate the diagnostic value of these markers on gastric cancer.
Results
Serum levels of CEA, CA125, and CA19-9 in gastric cancer group were higher than that in the benign gastric disease group and the healthy control group (P <0.005). The sensitivity of AFP, CEA, CA125 and CA19-9 in the diagnosis of gastric cancer was 4.7-20.8% individually, and increased to 40.3% in combination. By using optimal cut-off value, the sensitivity of CEA, CA125, and CA19-9 for the diagnosis of gastric cancer was improved. Especially, the sensitivity of CEA increased to 58.4% and the sensitivity of combined use of four markers increased to 69.1%. The age and gender had no effects on the diagnostic value of these markers.
Conclusions
The determination and application of optimal cut-off values based on ROC curve and logistic regression analysis could improve the diagnosis of gastric cancer based on common tumor markers.
Similar content being viewed by others


Background
It is difficult to differentiate the syndromes of gastric cancer and benign gastric diseases. Up to now, few effective biomarkers for gastric cancer have been applied in the clinic for the diagnosis of gastric cancer [1]. Currently, the diagnosis of gastric cancer mainly depends on invasive examination such as gastroscopy and biopsy. The detection of serum tumor marker is simple and easy and becomes a common clinical method for screening tumor. Tumor markers such as alpha fetoprotein (AFP), carcinoembryonic antigen (CEA), cancer antigen 125 (CA125) and cancer antigen 19–9 (CA19-9) have been widely used for the diagnosis of different types of cancers such as liver cancer, colorectal cancer and pancreatic cancer. However, when these markers are used individually for the diagnosis of gastric cancer, inconsistent results have been obtained [2–6].
A recent study reported that the use of a combination of Ki-67, Galectin-3, and PTTG can distinguish the benign and malignant thyroid tumor [7]. Therefore, we hypothesized that the combined use of tumor markers may avoid the inconsistence and increase the sensitivity for the diagnosis of gastric cancer. In this study we detected the serum levels of tumor markers AFP, CEA, CAl25 and CAl9-9 in 149 patients with gastric cancer, 111 patients with benign gastric diseases and 124 healthy people. Next we performed statistical analysis to compare the diagnostic value of these markers for gastric cancer. Our results showed that the determination of optimal cut-off values of these markers could increase the sensitivity for the diagnosis of gastric cancer.
Methods
Study subjects
Total 384 subjects were enrolled in this study who visited the First Affiliated Hospital of Nanchang University from May 2011 to May 2012, including patients with gastric cancer and benign gastric diseases, and healthy people who underwent physical examination. There were 149 patients in gastric cancer group (115 men, 34 women, age range 28 to 90 years old, average 59.1 years old). Among them, 30 patients had early gastric cancer and 119 patients had advanced gastric cancer. 71 patients had poorly differentiated adenocarcinoma, 72 patients had moderately differentiated adenocarcinoma, and 6 patients had highly differentiated adenocarcinoma. 70 patients had gastric antrum carcinoma, 61 patients had gastric body cancer, 13 patients had gastric cardia - bottom cancer, and 5 patients had multiple site cancer (more than two sites). There were 111 patients in benign gastric disease group (76 men, 35 women, age range 25 to 86 years old, average 52.9 years old). Among them, 24 patients had gastric ulcer, 53 patients had duodenal ulcer, 12 patients had complex ulcer, 17 patients had non-atrophic gastritis, and 5 patients had atrophic gastritis. 124 healthy people were included in the control group (72 men, 52 women, age range 37 to 83 years old, average 53.0 years old). Patients with gastric cancer and benign gastric diseases were diagnosed by endoscopy and confirmed by biopsy.
This study was performed in compliance with the Helsinki Declaration and according to a protocol approved by the Medical Ethics Committee of Nanchang University. All patients were informed about the study and gave their consent.
Serum tumor marker detection
Serum AFP, CEA, CA125 and CA19-9 levels were detected by using Roche electrochemiluminescence instrument at Department of Nuclear Medicine of the First Affiliated Hospital of Nanchang University. The normal reference values were as follows: AFP≤7 ng/mL, CEA≤6.5 ng/mL, CAl25≤ 35 U/mL, CAl9-9≤27 U/mL.
Statistical analysis
The data were expressed as mean ± standard deviation. The area under curve (AUC) of receiver operating characteristic (ROC) curve was used to evaluate the diagnostic value of serum tumor markers. Multivariate logistic regression analysis was used to establish the diagnostic mathematical model. On the basis of this model, the prediction value was calculated followed by ROC curve analysis. The statistical analysis was performed using SPSS17.0 statistical software (SPSS Inc., Chicago, IL, USA).
Results
The serum levels of CEA, CA125, CA19-9 and AFP in the study subjects
The demographic data such as age and gender and the test results of four serum tumor markers in gastric cancer group, benign gastric disease group and healthy control group were shown in Table 1. The average serum level and the positive rate of AFP, CEA, CA125 and CA19-9 in gastric cancer group were higher than that in the benign gastric disease group and the healthy control group.
Positive rates of serum tumor markers in gastric cancer of different clinicopathological features
According to the stage, location and histological differentiation of gastric cancer, we subdivided gastric cancer group and calculated positive rates of 4 serum tumor markers with qualitative combined detection. The results showed that the positive rate of serum tumor markers in the advanced gastric cancer was higher than that in the early gastric cancer. The positive rate of AFP, CEA and CA19-9 with combined detection in the cardia cancer was higher than that in the other parts. However, there were no significant differences in the positive rate of serum tumor markers among gastric cancer with different differentiation (Table 2).
The association of serum tumor marker levels with the risk of gastric cancer
To evaluate the significance of serum tumor marker levels for the diagnosis of gastric cancer, we analyzed the association of serum tumor marker levels with gastric cancer in gastric cancer group. We got crude odds ratio (OR) after logistic regression analysis (Table 3). To exclude the possible effects of age and gender, we got adjusted odds ratio (ORa) after the adjustment of gender and age, and the results showed that CEA, CA125 and CA19-9 levels were positively correlated with the risk of gastric cancer (Table 3).
Use of normal cut-off values of serum tumor markers for the diagnosis of gastric cancer
We took the normal value of tumor marker serum level as cut-off value to determine the negative or positive of gastric cancer. The results showed that the use of single serum tumor marker had good specificity (96.2%-99.1%) but poor sensitivity (4.7%-20.8%) for the diagnosis of gastric cancer (Table 4). The sensitivity was improved with the combined use of serum tumor markers, but was still low (Table 4).
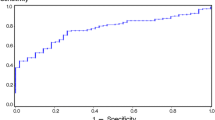
Use of optimum cut-off values of serum tumor markers for the diagnosis of gastric cancer
Since the sensitivity in gastric cancer diagnosis with the use of normal cut-off values of four serum tumor markers was low, the potential in clinical application would be limited. Therefore, we analyzed the serum markers to obtain AUC of ROC curve, determined optimum diagnostic cut-off values, and then calculated their diagnostic values on gastric cancer. The results showed that the use of optimum boundary values could significantly improve the sensitivity in gastric cancer diagnosis with CEA and combination (58.4% and 47.7%, respectively) (Table 5).
Discussion
In this study we analyzed the diagnostic value of four common clinical serum tumor markers AFP, CEA, CA125 and CA19-9 for gastric cancer. We compared the serum levels of these four markers in the gastric cancer group, benign gastric disease group and healthy control group, and found that the serum levels of all four markers were higher in gastric cancer group than in the benign gastric disease group and the healthy control group. Especially, the serum levels of CEA, CA125 and CA19-9 were significantly higher than in the benign gastric disease group and the healthy control group (P <0.005). In contrast, the serum levels of these four markers were not significantly different between the benign disease group and healthy control group (P = 0.581-0.844). These data suggest that these markers have diagnostic value for gastric cancer.
When we took the normal values of four markers as cut-off value to determine the negative or positive of the clinical specimens, we found that the specificity of four markers in the diagnosis of gastric cancer was more than 95%, when used individually, but the sensitivity was very low, ranging from 4.7% to 20.8%, and AUC was no more than 0.6. Thus single marker for clinical gastric cancer diagnosis is very limited [8]. When the four markers were combined, the sensitivity of the diagnosis of gastric cancer reached 40.3%, but was still not ideal.
To improve the sensitivity of gastric cancer diagnosis, we performed logistic regression analysis and used ROC curve to determine the optimum cut-off values. With the use of optimum cut-off values, for CEA the sensitivity was increased from 17.4% to 58.4% (the specificity was decreased from 99.1% to 83.4%), and AUC reached 0.767. These results are consistent with earlier studies performed in Chinese population [5, 9].
Furthermore, we investigated the relationship between serum levels of tumor markers and clinicopathological features of gastric cancer. We found that the positive rates of CEA, CA19-9, and combined use of four markers were higher in the advanced gastric cancer than in the early gastric cancer. The positive rates of CA19-9 and combined use of four markers were higher in the cardia cancer than in the other parts of the gastric cancer. Our results are in agreement with previous reports that the stage and sites of gastric cancer would affect serum marker levels [10–12]. However, the positive rates of markers among the gastric cancer with different differentiation were not statistically significant, suggesting that the differentiation has little impact on gastric carcinoma marker level as reported previously [13].
In this study, the age and gender ratio of study subjects in the three groups were statistically significant. To avoid the possible bias caused by these factors, we analyzed the effects of age and gender on serum levels of the four markers in the diagnosis of gastric cancer. We performed multivariate logistic regression analysis and got ORa adjusted for age and gender. The results showed that the differences in age and gender could not change the diagnostic value of markers for gastric cancer.
Conclusions
While the four common tumor markers when used individually has little clinical value in the diagnosis of gastric cancer, with the help of the ROC curve analysis and logistic regression analysis, we could determine the optimal cut-off values of the markers and improve the diagnosis of gastric cancer based on these markers. These results suggest that the optimal application of these common tumor markers could promote the clinical screening and diagnosis of gastric cancer.
References
Jackson C, Cunningham D, Oliveira J: Gastric cancer: ESMO clinical recommendations for diagnosis, treatment and follow-up. Ann Oncol. 2009, 20 (Suppl 4): 34-36.
Haglund C, Kuusela P, Roberts P, Jalanko H: Tumour marker CA 125 in patients with digestive tract malignancies. Scand J Clin Lab Invest. 1991, 51 (3): 265-270. 10.3109/00365519109091613.
Ychou M, Duffour J, Kramar A: Clinical significance and prognostic Value of CA72-4 compared with CEA and CA19-9 in patients with gastric cancer. Dis Markers. 2000, 16 (3–4): 105-110.
Li Y, Yang Y, Lu M: Predictive value of serum CEA, CA19-9 and CA72.4 in early diagnosis of recurrence after radical resection of gastric cancer. Hepatogastroenterology. 2011, 58 (112): 2166-2170.
Bornschein J, Selgrad M, Wex T, Kuester D, Malfertheiner P: Serological assessment of gastric mucosal atrophy in gastric cancer. BMC Gastroenterol. 2012, 12: 10-10.1186/1471-230X-12-10.
Zur B, Holdenrieder S, Walgenbach-Brünagel G, Albers E, Stoffel-Wagner B: Method comparison for determination of the tumor markers AFP, CEA, PSA and free PSA between Immulite 2000 XPI and Dimension Vista 1500. Clin Lab. 2012, 58 (1–2): 97-105.
Cui W, Lu X, Zheng S, Ma Y, Liu X, Zhang W: The use of a combination of Ki-67, Galectin-3, and PTTG can distinguish the benign and malignant thyroid tumor. Clin Lab. 2012, 58 (5–6): 419-426.
Lai IR, Lee WJ, Huang MT: Comparison of serum CA72-4, CEA, TPA, CA19-9 and CA125 levels in gastric cancer patients and correlation with recurrence. Hepatogastroenterol. 2002, 49: 1157-1160.
Chen XZ, Zhang WK, Kun Y: Correlation between serum CA724 and gastric cancer: multiple analyses based on Chinese population. Mol Biol Rep. 2012, 39: 9031-9039. 10.1007/s11033-012-1774-x.
Duraker N, Celik AN: The prognostic significance of preoperative serum CA 19–9 in patients with resectable gastric carcinoma: comparison with CEA. J Surg Oncol. 2001, 76 (4): 266-271. 10.1002/jso.1044.
Fan B, Xiong B: Investigation of serum tumor markers in the diagnosis of gastric cancer. Hepatogastroenterology. 2011, 58 (105): 239-245.
Mihmanli M, Dilege E, Demir U: The use of tumor markers as predictors of prognosis in gastric cancer. Hepatogastroenterology. 2004, 51 (59): 1544-1547.
Wobbes T, Thomas CM, Segers MF: Evaluation of seven tumor markers (CA 50, CA 19–9, CA 19–9 TruQuant, CA 72–4, CA 195, carcinoembryonic antigen, and tissue polypeptide antigen) in the pretreatment sera of patients with gastric carcinoma. Cancer. 1992, 69 (8): 2036-2041. 10.1002/1097-0142(19920415)69:8<2036::AID-CNCR2820690805>3.0.CO;2-M.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-230X/13/87/prepub
Acknowledgment
We would like to thank Dr. Yingqun Wang for his critical discussion and editing of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declared that they have no competing interest.
Authors’ contributions
KHZ, CZH and NHL designed the study; CZH, QL and XHL collected the samples; CZH and YH detected serum marker levels; KHZ and CZH performed statistical analysis; CZ H and KHZ drafted the manuscript. All authors read and approved the final manuscript.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
He, CZ., Zhang, KH., Li, Q. et al. Combined use of AFP, CEA, CA125 and CAl9-9 improves the sensitivity for the diagnosis of gastric cancer. BMC Gastroenterol 13, 87 (2013). https://doi.org/10.1186/1471-230X-13-87
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-230X-13-87