
Abstract
Background
Continued breathing following ventricular fibrillation has here-to-fore not been described.
Methods
We analyzed the spontaneous ventilatory activity during the first several minutes of ventricular fibrillation (VF) in our isoflurane anesthesized swine model of out-of-hospital cardiac arrest. The frequency and type of ventilatory activity was monitored by pneumotachometer and main stream infrared capnometer and analyzed in 61 swine during the first 3 to 6 minutes of untreated VF.
Results
During the first minute of VF, the air flow pattern in all 61 swine was similar to those recorded during regular spontaneous breathing during anesthesia and was clearly different from the patterns of gasping. The average rate of continued breathing during the first minute of untreated VF was 10 breaths per minute. During the second minute of untreated VF, spontaneous breathing activity either stopped or became typical of gasping. During minutes 2 to 5 of untreated VF, most animals exhibited very slow spontaneous ventilatory activity with a pattern typical of gasping; and the pattern of gasping was crescendo-decrescendo, as has been previously reported. In the absence of therapy, all ventilatory activity stopped 6 minutes after VF cardiac arrest.
Conclusion
In our swine model of VF cardiac arrest, we documented that normal breathing continued for the first minute following cardiac arrest.
Similar content being viewed by others

Background
Gasping following cardiac arrest is a well-investigated phenomenon [1–10]. Gasping probably occurs as a response to decreased brain perfusion and/or to hypoxia [11]. It has been observed in all mammals investigated, may be present at birth and at death, and is considered an "auto-resuscitative" phenomenon [12–14]
Gasping is an important phenomenon in humans suffering from cardiac arrest, with a reported occurrence of 55% in patients with witnessed out-of-hospital cardiac arrest [1]. Survival has been reported in 39% of humans with witnessed arrest who gasped while receiving bystander resuscitation efforts but in only 9% of individuals who did not gasp while receiving bystander resuscitation efforts [2].
Spontaneous ventilatory activity consistent with continued breathing during the first minutes of VF cardiac arrest has not been previously described. We observed this phenomenon in swine and performed ventilation recordings to characterize the ventilatory patterns.
Methods
This study was conducted with the approval of the University of Arizona Institutional Animal Care and Use Committee in accordance with the guidelines set forth in the "Position of the American Heart Association on Research Animal Use". This report is an analysis of the respiratory patterns following VF cardiac arrest of a previously reported study comparing two basic resuscitation protocols with regard to 24-hr neurological outcome [15]. Sixty-four swine (28 ± 4 kg) were anesthetized by inhalation of 5% isoflurane in oxygen. An endotracheal tube was placed, and anesthesia was maintained using 1.5 - 3% isoflurane in ambient air. Ventilation was provided by a rate- and volume-regulated ventilator (Narkomed 2A, North American Drager, Telford, PA, USA) and was adjusted to maintain an end-tidal CO2 pressure (EtCO2) of 40 ± 3 mmHg. Vascular introducer sheaths (7F, Cordis Corp., Miami, FL, USA) were placed by sterile cutdown procedures, and solid state pressure transducers (MPC-500, Millar Instruments, Houston, TX, USA) were positioned into the descending aorta and the right atrium. Electrocardiographic leads were placed on the limbs. An infrared capnometer (47210A, Hewlett Packard Co., Palo Alto, CA, USA) and a pneumotachometer (MP45-871, Validyne Engineering Corp., Northridge, CA, USA) were used to measure EtCO2 and air flow, respectively. Defibrillator pads (Quik-Combo, Medtronic, PhysioControl, Redmond, WA, USA) were adhered to the chest. All mentioned parameters were continuously displayed on a recording system (Gould Ponemah Physiology Platform, Model P3 Plus, LDS Life Science, Valley View, OH, USA) and stored on a laptop computer for analysis. After collection of baseline data, VF was induced by alternate current via a pacing electrode temporarily placed in the right ventricle. VF was confirmed by the fall in the arterial blood pressure and the electrocardiographic pattern. Assisted ventilation was discontinued immediately after induction of VF. Two additional control swine were similarly investigated, but rather than assisted ventilation, a period of spontaneous breathing during isoflurane anesthesia was allowed prior to the induction of VF to determine the normal breathing pattern.
Breathing was defined as a ventilatory pattern similar to that recorded during spontaneous ventilation under isoflurane anesthesia. Gasping has been previously defined as an abrupt transient inspiratory effort [16]. To avoid over-interpretation of irrelevant signals or artifacts, due to the high sensitivity of the capnometer, we defined any short inspiratory air flow followed by a rapid decrease of at least 25% of the EtCO2 as a gasp. Data on gasping was available in 61 of the 64 swine. Of those with no data, the capnograph malfunctioned in one animal, and in two others the data files were missing.
Statistical analysis
Data were entered into Microsoft Excel for Windows 2003 (Microsoft Corp, Redmond, WA, USA) and were analyzed using SPSS 16.0 for Windows (SPSS, Inc, Chicago, IL, USA). Continuous variables were presented as mean ± SD and median.
Results
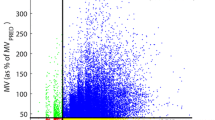
The baseline data are presented in Table 1. All 61 animals exhibited continuous spontaneous ventilatory activity during the first minute following the induction of VF (Figure 1) at an average rate of 10 breaths per minute (Figure 1, Table 2). During minutes 2 to 5, the occurrence of gasping varied between 23% and 82%, and the frequency was less than 3 gasps per minute (Table 2).

Spontaneous ventilatory activity during the first 6 minutes of untreated ventricular fibrillation (VF) plotted as mean ± standard error of the mean (SEM) for each minute after induction of VF.
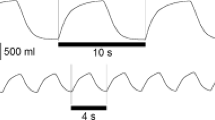
The air flow pattern during the initial minute after induction of VF appeared to be very similar to the flow pattern of normal spontaneous ventilation during anesthesia and was distinctly different from gasping (Figure 2). This spontaneous ventilation pattern was characterized by an initial increase in inspiratory flow reaching a plateau followed by high flow expiration (Figure 2A, B). This pattern is different from that observed during gasping (Figure 2C). The air flow pattern of typical gasps consists of a rapid increase in inspiratory flow, which immediately changes after reaching peak values, to a peak expiratory flow and a subsequent pause (Figure 3). The airflow pattern of breathing was also different from that of mechanical assisted ventilation (Figure 3 and 4). In contrast, the air flow pattern of typical gasps consists of a rapid increase in inspiratory flow, which immediately changes to a peak expiratory flow and a subsequent pause after reaching peak values (Figure 2C).

Graphic recording of aortic pressure (AoP), air flow signal, and end-tidal CO 2 (EtCO 2 ) curves in anesthetized swine during: A) Spontaneous breathing during normal sinus rhythm, B) Spontaneous breathing following the induction of ventricular fibrillation (VF), and C) Gasping during untreated VF. Note the relative plateau in the inspiratory air flow of the spontaneous breaths compared with the sharp "peak" in the air flow of the gasps.

Graphic recording showing the aortic pressure (AoP), air flow signal and end-tidal CO 2 (EtCO 2 ) curves in anesthetized swine during: A) Spontaneous breathing during normal sinus rhythm. B) Mechanical ventilation.

Graphic recording showing the aortic pressure (AoP), air flow signal and end-tidal CO 2 (EtCO 2 ) curves in anesthetized swine during the first 90 seconds of VF cardiac arrest. The asterisk (*) indicates the time point when the endotracheal tube was disconnected from the mechanical ventilator.
Discussion
In this swine model of out-of-hospital cardiac arrest, our group observed that following the induction of VF, all animals continued breathing for about one minute at a mean frequency of 10 breaths per minute (Figure 1). The continued breathing was then followed by the crescendo-decrescendo pattern of gasping that has previously been described [8] (Figure 1). The recorded air flow pattern during the first minutes following the onset of ventricular fibrillation was similar to that of regular spontaneous breathing of an anesthetized animal and was different from the air flow pattern typical for gasping or agonal ventilation that occurred during minutes 2 to 5 (Figure 2). This continued breathing pattern was also clearly different from the pattern of assisted mechanical ventilation (Figure 3). The finding of continued breathing for the first minute following VF cardiac arrest, if confirmed in humans, is of clinical relevance. The failure to recognize spontaneous breathing and gasping following cardiac arrest potentially delays the recognition of the arrest and, thus, the early initiation of resuscitation efforts.
The explanation for the observation of continued breathing during the first minute following VF cardiac arrest might well be related to carotid artery and cerebral blood flow patterns immediately following untreated VF cardiac arrest. Frenneaux and Steen [17, 18] reported that carotid artery blood flow was relatively well maintained for the first minute following untreated VF cardiac arrest, before rapidly and markedly decreasing during the second minute and remaining marginal but still present for up to four minutes. Ristagno and colleagues [8] also found that there was substantial cerebral cortical microvascular flow after the onset of VF that rapidly decreased during the first three minutes of untreated VF cardiac arrest in swine. Cerebral blood flow differs from coronary artery blood flow, which ceases almost immediately after VF cardiac arrest [18].
Our observation of normal breathing during the first minute of VF was followed by a slower rate of spontaneous ventilation during minutes 2 to 5, which was typical of gasping or agonal respiration. As shown in Figure 2, gasping has a ventilatory flow pattern distinctly different from normal breathing or mechanical ventilation and typically exhibits a crescendo-decrescendo frequency pattern. After the fifth minute of untreated VF, gasping was not observed.
Gasping following cardiac arrest has been previously reported in human [1–3] as well as in animal models. In 1988 study in rats, von Planta and colleagues [19] reported that "gasping typically began 1 min after the induction of VF". In a swine model of VF cardiac arrest, Srinivasan [9] found that the time to the first gasp was 1.5 ± 0.5 min and that gasping ended on average 4.7 min after the onset of VF cardiac arrest. Ristagno and colleagues [8] also reported on the frequency of gasping during minutes 2 to 5 after onset of VF cardiac arrest. In their swine model, Frenneaux and Steen [18] found that gasping typically began weakly, increased to a maximum and generally ceased entirely by about 5 minutes post VF induction. These reports do not comment on spontaneous ventilatory activity during the first minute of VF cardiac arrest.
Menegazzi et al. [20] reported in a study of 12 swine that were sedated with ketamine/xylazine, and anesthetized with alpha-chloralose that all had agonal respirations through the first 2 minutes of arrest. The number of swine presenting spontaneous respiratory activity decreased to 11 (92%) at minute 3, five (42%) at minute 4, and two (17%) at minute 7. Mean respiratory rates ranged from 6 to 11 breaths/min. This report did not analyze the air the air flow pattern or the wave form of the end-tidal CO2 curves and invariably refers to post arrest ventilations as agonal respirations, whereas our findings suggest two different types of agonal respirations; initially continued breathing followed by typical agonal or gasping ventilations.
We believe that this is the first published report showing two different spontaneous air flow patterns during the early phase following VF cardiac arrest. However, based upon the references cited we wonder whether this has been a present but unrecognized phenomenon.
The pattern of continued spontaneous breathing for the first minute of VF cardiac arrest may be explained by continued perfusion through the carotid artery (and presumably continued cerebral blood flow), as reported by Frenneaux and Steen [18] following the induction of VF. Breathing no doubt stops in response to inadequate cerebral blood flow. Gasping, produced by a more primitive ventilatory center located in the brain stem is then activated [11–14]. Gasping is initiated during the second minute of VF cardiac arrest and increases during the third minute, but as the gasping center in the brain stem becomes more ischemic, the frequency of gasping decreases and eventually stops. This is a plausible explanation for the classically described crescendo-decrescendo pattern of gasping following untreated cardiac arrest [18].
There are limitations to this study that must be considered. This study is observational only and was not designed to determine the mechanisms of spontaneous breathing and gasping. Gasping is markedly more pronounced in immature animals [11–13]. Although the young swine used in this study were not immature, they might have exhibited a higher relative frequency of gasping compared with aged animals. The phenomenon of gasping is also related to the type and duration of anesthesia the animals are subjected to before the induction VF and the presence or absence of paralysis. The swine in this study were not paralyzed and were maintained on a relatively low concentration of isoflurane, which is less likely to suppress gasping relative to some other commonly used anesthetics, but might reduce the respiratory stimulation due to increasing pCO2 [21]. In our experience, high doses of isoflurane will also suppress gasping.
Conclusions
In this swine model of VF cardiac arrest, spontaneous ventilatory activity was observed in all 61 animals during the first minute after cardiac arrest. The airflow pattern of ventilations during the first minute was the same as that exhibited during spontaneous breathing in anesthetized swine. Thereafter, the airflow pattern changed to that typical of gasping. This pattern change is suggestive of a shift in the "respiratory center" from the breathing center located in the medullo-pontine area caudally to a gasping center located in the medulla oblongata. Gasping was not present after 5 minutes of untreated VF.
Spontaneous ventilatory activity following VF cardiac arrest is a potentially important phenomenon. The observation of continued breathing following VF cardiac arrest is reported to encourage others to determine whether this phenomenon also occurs in man. If so, these phenomena may well have important clinical implications for the early recognition of cardiac arrest.
Key messages
-
In swine undergoing VF cardiac arrest, normal spontaneous breathing occurred during the first minute.
-
Gasping was observed in swine between minutes 2 and 5, but never after minute 5, of untreated VF cardiac arrest.
-
If found to occur in man, spontaneous ventilatory activity following VF cardiac arrest may have important implications for the early recognition of cardiac arrest.
Abbreviations
- AOP:
-
aortic pressure
- ETCO2 :
-
end-tidal CO2
- SEM:
-
standard error of the mean
- VF:
-
ventricular fibrillation
References
Clark JJ, Larsen MP, Culley LL, Graves JR, Eisenberg MS: Incidence of agonal respirations in sudden cardiac arrest. Ann Emerg Med. 1992, 21: 1464-1467. 10.1016/S0196-0644(05)80062-9.
Bobrow BJ, Zuercher M, Ewy GA, Clark L, Chikani V, Donahue D, Sanders AB, Hilwig RW, Berg RA, Kern KB: Gasping during cardiac arrest in humans is frequent and associated with improved survival. Circulation. 2008, 118: 2550-2554. 10.1161/CIRCULATIONAHA.108.799940.
Bang A, Herlitz J, Martinell S: Interaction between emergency medical dispatcher and caller in suspected out-of-hospital cardiac arrest calls with focus on agonal breathing. A review of 100 tape recordings of true cardiac arrest cases. Resuscitation. 2003, 56: 25-34. 10.1016/S0300-9572(02)00278-2.
Noc M, Weil MH, Sun S, Tang W, Bisera J: Spontaneous gasping during cardiopulmonary resuscitation without mechanical ventilation. Am J Respir Crit Care Med. 1994, 150: 861-864.
Noc M, Weil MH, Tang W, Turner T, Fukui M: Mechanical ventilation may not be essential for initial cardiopulmonary resuscitation. Chest. 1995, 108: 821-827. 10.1378/chest.108.3.821.
Berg RA, Kern KB, Hilwig RW, Berg MD, Sanders AB, Otto CW, Ewy GA: Assisted ventilation does not improve outcome in a porcine model of single-rescuer bystander cardiopulmonary resuscitation. Circulation. 1997, 95: 1635-1641.
Xie J, Weil MH, Sun S, Yu T, Tang W: Spontaneous gasping generates cardiac output during cardiac arrest. Crit Care Med. 2004, 32: 238-240. 10.1097/01.CCM.0000105042.52059.5A.
Ristagno G, Tang W, Sun S, Weil MH: Spontaneous gasping produces carotid blood flow during untreated cardiac arrest. Resuscitation. 2007, 75: 366-371. 10.1016/j.resuscitation.2007.04.020.
Srinivasan V, Nadkarni VM, Yannopoulos D, Marino BS, Sigurdsson G, McKnite SH, Zook M, Benditt DG, Lurie KG: Spontaneous gasping decreases intracranial pressure and improves cerebral perfusion in a pig model of ventricular fibrillation. Resuscitation. 2006, 69: 329-334. 10.1016/j.resuscitation.2005.08.013.
Manole MD, Hickey RW, Momoi N, Tobita K, Tinney JP, Suciu GP, Johnnides MJ, Clark RS, Keller BB: Preterminal gasping during hypoxic cardiac arrest increases cardiac function in immature rats. Pediatr Res. 2006, 60: 174-179. 10.1203/01.pdr.0000228333.11132.fa.
Campbell AGM, Cross KW, Dawes GS, Hyman AI: A comparison of air and O2, in a hyperbaric chamber or by positive pressure ventilation, in the resuscitation of newborn rabbits. J Pediatr. 1966, 68: 153-163. 10.1016/S0022-3476(66)80146-4.
Gozal D, Torres JE, Gozal YM, Nuckton TJ: Characterization and developmental aspects of anoxia-induced gasping in the rat. Biol Neonate. 1996, 70: 280-288. 10.1159/000244377.
Manole MD, Hickey RW: Preterminal gasping and effects on the cardiac function. Crit Care Med. 2006, 34: S438-441. 10.1097/01.CCM.0000246010.88375.E4.
St-John WM, Paton JF: Respiratory-modulated neuronal activities of the rostral medulla which may generate gasping. Respir Physiol Neurobiol. 2003, 135: 97-101. 10.1016/S1569-9048(03)00018-1.
Ewy GA, Zuercher M, Hilwig RW, Sanders AB, Berg RA, Otto CW, Hayes MM, Kern KB: Improved neurological outcome with continuous chest compressions compared with 30:2 compressions-to-ventilations cardiopulmonary resuscitation in a realistic swine model of out-of-hospital cardiac arrest. Circulation. 2007, 116: 2525-2530. 10.1161/CIRCULATIONAHA.107.711820.
Bartels H, Dejours P, Kellogg RH, Mead J: Glossary on respiration and gas exchange. J Appl Physiol. 1973, 34: 549-558.
Chamberlain D, Frenneaux M, Steen S, Smith A: Why do chest compressions aid delayed defibrillation?. Resuscitation. 2008, 77: 10-15. 10.1016/j.resuscitation.2007.11.010.
Frenneaux MP, Steen S: Hemodynamics of cardiac arrest. Cardiac Arrest: The science and practice of resuscitation medicine. Edited by: Paradis NA, Halperin RA, Kern KB, Wenzel V, Chamberlain DA. 2007, New York: Cambridge University Press, 347-366. full_text. 2
von Planta I, Weil MH, von Planta M, Bisera J, Bruno S, Gazmuri RJ, Rackow EC: Cardiopulmonary resuscitation in the rat. J Appl Physiol. 1988, 65: 2641-2647.
Menegazzi JJ, Check BD: Spontaneous agonal respiration in a swine model of out-of-hospital cardiac arrest. Acad Emerg Med. 1995, 2: 1053-1056. 10.1111/j.1553-2712.1995.tb03149.x.
Forber NE, Pagel PS, Warltier DC: Pulmonary Pharmacology. Miller's Anesthesia. Edited by: Miller RD. 2005, Philadelphia: Churchill Livingstone, 1: 155-189. 6
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2261/10/36/prepub
Acknowledgements
Mathias Zuercher has significant support by the "Anaesthesieverein" of the Department of Anaesthesia and Intensive Care, University Hospital Basel, Switzerland. Gordon A. Ewy has an unrestricted grant from private donations to the University of Arizona Foundation for support of Sarver Heart Center's Resuscitation Research and is co-investigator on an unrestricted grant from the Laerdal Foundation of Stavanger, Norway, both significant. Robert A. Berg has an unrestricted grant from the Laerdal Foundation of Stavanger, Norway, and has Grants from the National Institutes of Health, National Heart, Lung, and Blood Institute, Bethesda, MD, USA, and from Medtronics Inc., all significant, and is on the Scientific Advisory Board of the AHA National Registry of CPR. Karl B. Kern is the principal investigator of a significant unrestricted grant from the Laerdal Foundation of Stavanger, Norway, and is on the Scientific Advisory committee.
We would like to acknowledge Nick Hurst and Alice McArthur for their technical assistance, Vatsal Chikani, MPH, for statistical assistance, and Allison Dwileski, BS, for excellent graphical assistance and editorial support.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
This study was conceived and designed by MZ, GAE, RWH, RAB and KBK. MZ, GAE, RWH, ABS, CWO and KBK analyzed and interpreted the data. MZ conducted the statistical analysis, and MZ and GAE drafted the original version of the manuscript. MZ, GAE, RWH, ABS, CWO and KBK revised the manuscript critically for important intellectual content and share responsibility for the final approval of the manuscript. All authors have read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Zuercher, M., Ewy, G.A., Hilwig, R.W. et al. Continued breathing followed by gasping or apnea in a swine model of ventricular fibrillation cardiac arrest. BMC Cardiovasc Disord 10, 36 (2010). https://doi.org/10.1186/1471-2261-10-36
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2261-10-36