
Abstract
Background
The potential of genetic testing to rapidly diagnose drug resistance has lead to the development of new diagnostic assays. However, prior to implementation in a given setting, the association of specific mutations with specific drug resistance phenotypes should be evaluated. The purpose of this study was to evaluate molecular markers in predicting drug resistance in the Central Region of Cameroon.
Results
From April 2010 and March 2011, 725 smear positive pulmonary tuberculosis patients were enrolled and all positive cultures were tested for drug susceptibility. A total of 63 drug resistant and 100 drug sensitive Mycobacterium tuberculosis complex clinical isolates were screened for genetic mutations in katG, inhA, ahpC, rpoB, rpsL, rrs, gidB and embCAB loci using DNA sequencing. Of the 44 isoniazid resistant (INHR) isolates (24 high level, 1 μg/ml and 20 low level, 0.2 μg/ml), 73% (32/44) carried the katG315 and/or the -15 inhA promoter mutations. Of the 24 high level INHR, 17 (70.8%) harbored katG315 mutation, 1 a point mutation (-15C → T) in the inhA promoter and 6 were (25.0%) wild types. Thus, for INHR high level detection, katG315 mutation had a specificity and a sensitivity of 100% and 70.8% respectively. Of the 20 low level INHR, 10 (50.0%) had a -15C → T mutation in the inhA promoter region, and 1 (2.2%) a -32G → A mutation in the ahpC promoter region. All of the 7 rifampicin resistant (RIFR) isolates carried mutations in the rpoB gene (at codons Ser531Leu (71.4%), His526Asp (14.3%), and Asp516Val (14.3%)). Of the 27 streptomycin resistant (SMR) isolates, 7 carried mutations at the rpsL and the gidB genes. 1 of the 2 ethambutol resistant (EMB R) isolates displayed a mutation in embB gene.
Conclusion
This study provided the first molecular investigation assessing the correlation of phenotypic to genotypic characteristics on MTB isolates from the Central Region of Cameroon using DNA sequencing. Mutations on rpoB, katG315 and -15 point mutations in inhA promoter loci could be used as markers for RIF and INH -resistance detection respectively.
Similar content being viewed by others


Background
Despite the availability of an effective treatment for decades, tuberculosis (TB) continues to cause great mortality and suffering, especially in poor and less-developed countries. Its association with the HIV/AIDS pandemic forms a lethal combination. In addition, multidrug resistant (MDR) TB and the recently-described extensively drug resistant (XDR) TB severely complicate the management and control of the disease worldwide [1, 2]. Almost 8.8 million new cases of TB were reported in 2010, and 1.4 million deaths were attributed to the disease. Asia and Sub-Saharan Africa accounted for 85% of new cases of TB worldwide [3]. Of the 8.8 million incident cases in 2010, 1.1 million (13%) were among people living with HIV.
Tuberculosis remains a common disease in Cameroon, with an estimated of 25 000 cases annually [4]. Like in other poor resources countries, therapeutic decisions are most often made by algorithms according to WHO guidelines. Inadequate or improper prescription of drugs, poor patient compliance and supervision of therapy may lead to the emergence of drug resistant strains [5]. Drug resistance in tuberculosis (TB) is a matter of great concern for TB control programs since these strains could spread in the community, stressing the need for early detection of drug resistance and subsequently initiation of adjusted therapy. Conventional diagnosis of drug-resistance in MTB strains relies heavily upon mycobacterial culture and drug susceptibility testing in liquid or solid media. Usually, results are only obtained after weeks to months of incubation and many developing countries lack the resources to establish the stringent laboratory conditions needed for these growth-based methods. From a clinical perspective, the existing growth-based diagnostics are too slow as patients undergoing treatment with drugs to which they are resistant, remain contagious, and those with XDR-TB and HIV often die before they are even diagnosed [6]. Major advances in molecular biology and the availability of new information generated after deciphering the complete genome sequence of M. tuberculosis[7], have led to the development of new tools for rapid detection of drug resistance [8, 9]. Molecular methods are based on assigning the presence or absence of certain mutations in specific positions or genetic locations which are known to be associated with resistance [10]. About 95% of rifampicin (RIF) -resistant strains have mutations in the 81-bp core region of the rpoB gene encoding the β-subunit of the RNA polymerase, named RIF-Resistance Determining Region (RRDR) [11]. In contrast to RIF, the situation for isoniazid (INH) is much more complex. Resistance mutations have been reported in at least 4 different genes including katG, inhA, ahpC and oxyR[10]. Meanwhile, resistance against streptomycin (SM) has been reported to be associated with mutations in rrs gene, which codes for 16S ribosomal RNA, and rpsL coding for the ribosomal protein S12 [12] and these mutations are found in a limited proportion of clinically isolated SM-resistant M. tuberculosis strains. Recently, Okamoto et al. [13] found that mutations within the gidB gene which encodes a conserved 7-methylguanosine (m7G) methyltransferase specific for the 16S rRNA, is associated with low-level SM-resistance and are an important cause of resistance found in 33% of resistant M. tuberculosis isolates. Resistance to ethambutol (EMB) is primarily mediated by mutations in the embB gene, coding for an arabinosyltransferase participating in mycobacterial cell wall synthesis, with codon 306 being most frequently affected [14]. Furthermore, mutations in the embA[15, 16] and upstream of embC[16, 17] are also involved in EMB -resistance.
Since the frequency and type of gene mutation varies greatly among different geographic regions in the world [18], it is important to evaluate the type and distribution of resistance associated mutations as a prerequisite for a large-scale implementation of genotypic approaches aimed at rapidly detecting resistance. However, up to now data assessing sensitivity and specificity of specific mutations for the detection of drug resistance phenotypes in our settings is still unavailable. Therefore CANTAM (Central Africa Network for Tuberculosis, HIV/AIDS and Malaria) an EDCTP (European and Developing Clinical Trials Partnership) funded network [19], with the goal to establish a cohort and prepare new sites for conducting future clinical trials of new TB drugs and vaccines in Central Africa countries, carried out a population based study, involving MTBC strains from Central region of Cameroon, to determine the genetic basis of first line drug resistance.
Methods
Mycobacterial isolates
During this baseline study carried out between April 2010 and March 2011, 725 smear positive pulmonary tuberculosis patients were enrolled at Jamot Hospital and Mbalmayo District Hospital. All positive cultures were tested for drug susceptibility to INH (0.2 μg/ml and 1 μg/ml), RIF (40 μg/ml), EMB (2 μg/ml), SM (4 μg/ml), OFX (2 μg/ml) and KAN (20 μg/ml) by the indirect proportion method on Lowenstein Jensen medium [20]. Phenotypically, 44 isolates were INHR (24 high level and 20 low level), 27 isolates were SMR, 7 isolates were RIFR and 2 isolates were EMBR. The 63 resistant isolates to INH, RIF, SM and EMB or MDR were screened for genetic mutations. In addition, M. tuberculosis strain H37Rv (susceptible) and 100 fully susceptible clinical isolates from the panel of susceptible strains collected during the study period were included to serve as controls. The study was approved by the Cameroon National Ethic Committee and the Cameroonian Ministry of Public Health. Written informed consent was obtained from all study subjects.
DNA extraction
Briefly, a loop-full of mycobacterial colonies was suspended in 400 μl of 10 mM Tris–HCl, 1 mM EDTA (pH 7.0) buffer and inactivated at 90°C for 30 min. The suspension was then centrifuged at 12,000 g for 1 min and the supernatant, containing nucleic acids, was harvested and transferred into a new eppendorf tube. Crude DNA extracts were stored at -20°C and then shipped to Germany for molecular analysis according to International Air Transport Association guidelines.
PCR amplification of target genes
The DNA extract was used as a template for PCR with the primers listed in Table 1. Each final PCR volume of 20 μl contained 10× PCR buffer (Qiagen, Germany), 5% DMSO, 20 pmol of forward and 20 pmol of reverse primers, 11.9 μl of distilled water, 0.5 μl MgCl2 25 mM (Qiagen, Germany), dNTPs at a final concentration of 500 μM, 0.2 μl of Taq polymerase 5 U/μL (Qiagen, Germany), and 2 μl of crude DNA extract (≈50 ng). The cycling program included a cycle of an initial denaturation step at 94°C for 5 min, followed by 35 cycles of denaturation at 94°C for 1 min, annealing at the temperature and time indicated in Table 1, and elongation at 72°C for 1 min. The final elongation step was set at 72°C for 10 min for one cycle. The PCR products were examined by gel electrophoresis and purified by use of a Nucleospin Extract II kit (Macherey Nagel, Germany) according to the manufacturer instructions.
Sequencing
Purified PCR products were sequenced with the same primers using the ABI’s Big dye terminator kit (Applied Biosystems, USA) according to the manufacturer’s instructions. At each locus, both forward and reverse primers at each locus were included in order to maximize the coverage of the amplified gene fragment, and the reproducibility of the results. Sequencing reactions include 1 μl big dye, 2 μl sequencing buffer, 0.5 μl of each 2.5 μM primer, a volume of PCR template corresponding approximately to 2–3 ng of DNA, and sufficient distilled water for obtaining a 10 μl final volume. Unincorporated terminators were removed by treatment on a sephadex column. The obtained sequences were aligned using the assembling application of vector NTI (Invitrogen) and CodonCode Aligner, and polymorphisms detection was achieved by comparison with the published M. tuberculosis H37Rv sequence.
Quality control
M. tuberculosis H37Rv (ATCC 27294) was included as a quality controls for the phenotypic and genotypic tests.
Results
Analysis of INH -resistance associated mutation
A total of 44 INHR (24 high level and 20 low level)) and 100 matched INHS sensitive control strains were screened for mutations at katG codon 315, the fabG1-inhA regulatory region, the inhA ORF, the oxyR-ahpC intergenic region by DNA sequence analysis. A complete list of specific mutations, which had been identified is provided in Table 2.
Polymorphisms in the katG gene
Among the 24 high level INH-resistant isolates, 18 (75%) were genetically altered in the katG region. Out of these, 17 (70.8%) had a resistance associated mutation in katG codon 315 and one isolate had a partial katG gene deletion (Table 2).
Of the 18 isolates altered in the katG gene, 7 had an additional mutation in the fabG1-inhA regulatory region (2 at position -15C → T and 5 at position -47G → C). The katG315 mutations resulted in a change of the wild-type codon, AGC (Ser) to ACC (Thr) in 17 strains and AAC (Asn) in one strain. All of the INH susceptible strains lacked mutations in katG 315. Thus for detection of high level INH -resistance, mutation/partial deletion of the katG gene had a specificity of 100.0% and a sensitivity of 75% (18/44).
Of the 20 low level INH-resistant isolates, 2 (10%) harboured the katG315 mutation. In total, the katG315 mutation was seen in 19 isolates with 16 (84.2%) being high level INH-resistant isolates. Therefore, this mutation might be associated with high level INH -resistance (1 μg/ml). Overall, for the detection of INH -resistance, mutation/partial deletion of the katG gene had a specificity of 100.0% and a sensitivity of 45.5% (20/44).
Polymorphisms in the inhA gene
The inhA region consists of two genes, fabG1 and inhA. Among the 24 high level INH-resistant isolates, 3 harboured the mutation -15C → T in the regulatory region of inhA with 2 of them carrying an additional katG315 mutation and 5 had nucleotide changes (G → C) at position -47. All the 5 INH-resistant isolates with -47 G → C mutation also harbored the katG 315 mutation.
Out of the 20 low level INH-resistant isolates, 10 (50%) had mutations in fabG1-inhA leading to a C → T change at position -15 of the start site of fabG. In total, the fabG1-inhA mutation at -15 position was observed in 13 isolates with 10 (77%) being low level INH-resistant isolates. Therefore, this mutation seems to be associated with low level INH -resistance (0.2 μg/ml). None of the INH susceptible isolates had the mutation affecting the inhA promoter region at position -15. On the contrary, the nucleotide change at position -47 was also seen in 24 isoniazid susceptible isolates and a new mutation -102C → T not yet described was detected in 3 other INH susceptible isolates. No mutation was observed in inhA ORF gene (Table 3).
Polymorphisms in the oxyR-ahpC intergenic region
One low level INH-resistant isolate displayed a G → A substitution at position 32 upstream of the transcriptional start site of ahpC in the oxyR-ahpC intergenic region, which has previously been shown to be involved in INH -resistance [15].
Combined sensitivity and specificity of katG and inhA promoter region for INH resistance
Mutations in katG315 and -15 C → T in inhA promoter region accounted together for 73% (33/44) INH -resistance. Since none of these mutations was observed in susceptible isolates, the combined specificity is 100%.
Analysis of the rpoB gene responsible for RIF-resistance
In this study, 7 RIFR isolates, and 100 RIF-sensitive (RIFs) clinical isolates were examined for mutations in a 158-bp fragment of rpoB gene. Of 7 RIFR isolates, resistance-associated mutations in the core region of rpoB were found in all 7 (100.0%) isolates (Table 3). The nucleotide and amino acid changes identified in drug-resistant isolates are shown in Table 4. Three different rpoB mutations were identified involving codons 516, 526, and 531. The most common mutation, which changes TCG (Ser) to TTG (Leu) in codon 531, was detected in 5 (71.4%) of the 7 mutated RIF-resistant isolates (Table 3). A mutation affecting codon 516 and leading to a substitution of aspartate to tyrosine was observed in the rpoB gene of one RIF sensitive isolate. Hence, mutations in the rpoB gene exhibited a sensitivity of 100.0% and a specificity of 99.0%.
Analysis of mutations in the target regions of SM -resistance
All strains were first sequenced (27 SMR isolates and 100 fully susceptible isolates) in the rrs gene. As none of the resistant strains displayed a mutation in this gene, sequence analysis of rpsL was performed. Among the 27 SMR strains 2 carried a mutation in rpsL gene at codon 43 and none showed a polymorphism at codon 88. The 2 resistant isolates mutated at codon 43 had a Lys → Arg substitution (Table 4). The remainder of the phenotypically resistant strains (n = 25) did not carry a mutation in rpsL gene and no changes were found in the drug-susceptible isolates. The specificity of rpsL43 mutation for resistance detection of SMR was 100%.
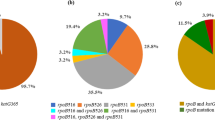
Additionally all strains were sequenced in gidB gene. In this very polymorphic gene, 5 different mutations with 3 of them never been reported were found in 5 SMR strains and 2 different mutations in 6 SMS strains (see Table 4). The 5 mutations at codon 36GTG → GGG, 48CAT → AAT, 75CCG → TCG, 79TTG → TGG, 138GCG → CCG were exclusively found in streptomycin resistant strains while the mutations at codon 205GCA → GCG and 16CTT → CGT were exclusively found in streptomycin sensitive strains.
Analysis of mutations in the target regions of EMB -resistance
In this study, we analyzed polymorphisms in the embCAB operon for 2 ethambutol resistant isolates and 100 ethambutol sensitive isolates. Among our 2 EMB -resistant isolates, sequence analysis of the embB gene identified 1 isolate with EMB-resistance-associated nucleotide substitutions in codon 306ATG → GTG that result in amino acid replacement (306Met → Val) and the remaining isolate as well as all sensitive isolates had no amino acid replacements in embB gene. As embB mutations are not the only ones involved in EMB-resistance mechanisms in M. tuberculosis, we also analyzed embC and embA loci for mutations. Sequence analyses of embC and embA revealed no mutations in EMB -resistant isolates while 6 of 100 fully susceptible isolates have mutations at position -20A → C and -230A → C of embC upstream region. Although the substitutions at position -20A → C were present only in EMB-susceptible organisms in our sample, these three strains also had synonymous mutation at codon 330CTG → TTG of the embA gene and nucleotides replacement at position -102C → T in the regulatory region of fabG1-inhA operon; this is exclusively found in susceptible organisms. The 3 samples with mutations at position -230A → C also harbored simultaneously a nucleotide replacement at position -47 in the regulatory region of fabG1-inhA operon. Three of 100 fully susceptible strains had synonymous mutations at codon 330CTG → TTG of embA gene, which did not resulting in amino acid replacement. These 3 isolates harbored simultaneously nucleotide replacement at position -20 upstream of the initiation site of embC gene. All EMB susceptible strains (n = 100) had a wild-type embB sequence.
Discussion
Early detection of drug resistance constitutes one of the priorities of TB control programs. It allows initiation of the appropriate treatment in patients and avoids dissemination of resistant strains in the community. In the context of a poor resource country, detection of drug resistance is performed in the reference laboratory by so-called ‘conventional methods’ based on detection of growth of M. tuberculosis in the presence of the respective antibiotics. Depending on the method, this process requires at least 10 days to 8 weeks before drug sensitivity results are available. During this time the infected patient may be treated incorrectly which may have serious health implications in particular in patients with HIV-TB coinfection. The disclosure of the genetic basis of resistance to anti-tuberculous agents has enabled development of new molecular tests to detect mutations associated with reduced susceptibility to antituberculous drugs [9, 10]. In order to detect and validate the drug resistance associated mutations, DNA sequencing is the most accurate among the molecular techniques. We used PCR fragment sequencing since molecular mechanisms explaining resistance to anti-tuberculous agents are not fully understood [24]. It presents the advantage, over methods that use DNA probes, to detect unknown mutations. Recently the GeneXpert has been endorsed by the WHO for point of care testing [25]. Drug sensitivity testing with this method is based on the detection of mutations in the core region of the rpoB gene, thus only RIF-resistance or MDR would be detected.
In this study, we set out to investigate the association of phenotypic resistance with genetic mutations in drug resistance TB isolates in Cameroon. The majority of the isolates in this study were from the Jamot Hospital (Central Region of Cameroon), the reference hospital for diagnostic and treatment of pulmonary diseases throughout the country. Therefore, the data obtained in this study can be considered to be representative of the make-up of resistance conferring mutations present in M. tuberculosis strains in this region.
A 158-bp fragment of the rpoB gene from codon 507 to 533 was amplified and sequenced to detect mutations in RIFR strains. Of the 7 phentotypically RIFR strains, mutations were found in the rifampicin resistant determining region (RRDR) for all the 7 isolates. These alterations affected the codons Ser531Thr (71.4%), His526Asp (14.3%) and Asp516Val (14.3%). The rpoB codons 531, 526, and 516 are the most frequently mutated codons worldwide, although variations in the relative frequencies of mutations in these codons have been described for M. tuberculosis isolates from different geographic locations. The most common site of nucleotide substitutions in RIFR isolates was codon 531. This finding was similar to those reported in Russia [26], the US [27], Tunisia [28] Ghana [21] and Germany [29]. The codon 531 mutation was also reported as the most frequent (68%) in M. tuberculosis isolates of the LAM family in Cameroon [30]. For codons 526 and 516 involved in RIFR, mutations in our strains occurred at equal frequencies than in strains from other geographical regions [31–33]. It has been shown that various substitutions in the same codon can lead to different level of resistance. Mutations at codon 516 of the rpoB gene can confer either low or high level resistance depending on the codon change [34]. It has been reported that substitution of aspartate by tyrosine in codon 516 induced RIF-resistance of M. tuberculosis with minimum inhibitory concentration (MIC) between 15 μg/ml and 25 μg/ml in BACTEC 460-TB system [34]. In our study, RIF susceptibility was evaluated in Lowenstein Jensen at a concentration of 50 μg/ml. This might explain why strains harbouring this mutation in our study were phenotypically RIF-susceptible. Among the 7 isolates which were altered genetically, 6 were MDR strains and one a RIF-SM-resistant isolate. Thus, rpoB could be an indicator of multidrug resistance among M. tuberculosis strains. This observation was previously reported among Cameroonian M. tuberculosis isolates [30].
It has been previously shown that about 10–15.9% of RIF -resistant isolates do not have mutations in the RRDR [15]. More than 90% of RIF -resistant strains from other regions had mutations located in the 81-bp core region [35–38]. This indicated a possible occurrence of alteration outside the core region of 81 bp of the examined rpoB. Among other explanations, several additional genes might be involved in RIF-resistance such as rpoA, rpoC or rpoD[39]. The natural resistance to RIF in some M. avium and M. intracellular strains is known to be a result of efficient cell wall permeability and exclusion barrier, suggesting that these elements could also play an important role in M. tuberculosis[34]. However, in our study, all the isolates harboured mutations in the RRDR core region.
Common genes known to be involved in INH-resistance are katG, inhA, ahpC, oxyR[10]. Several investigators have shown that INH-resistance in M. tuberculosis isolates arise principally from a katG gene alteration [40–42] that corresponds essentially to point mutations in codon 315 (point mutations in two bases 944 and 945). In this study, 18 (40.0%) INH -resistant isolates were genetically altered in the katG codon 315. Others studies have reported 95% of all INH-resistant isolates with mutations in codon 315 [43]. Out of the 6 MDR strains identified in this study, 5 displayed a high level resistance to isoniazid with a katG alteration and the remaining one displayed a low level INH-resistance with -32G → A mutation in oxyR-ahpC intergenic region. Therefore, it will be useful to combine katG315 and -15 point mutation inhA promoter region with rpoB in molecular assays looking at drug resistance. Since some of the INHR strains in this study had no mutation in katG 315 and -15 inhA promoter region, it is likely that mutations in other genes, such as the inhA locus, contribute to resistance. Previous studies have shown that mutations in the upstream region of the inhA locus result in increased levels of InhA (NADH-dependent enoyl-acyl carrier protein reductase) expression, thereby elevating the drug target levels and producing INH -resistance via a titration mechanism [15]. We assessed for mutations in the inhA regulatory region of all the 44 INHR M. tuberculosis strains and found a substitution at position 15 upstream of the start codon in 13 (28.9%) isolates. The frequency of the occurrence of specific INH-resistance conferring mutations varied between geographical regions in the world [26]. A study in Equatorial Guinea reported the absence of mutation in the katG gene of M. tuberculosis INH -resistant isolates [44]. The unique katG mutation observed in this study was the substitution of Serine to Threonine at codon 315. High proportion of Ser315katG mutations has been reported in Russia (76.9%) [26], in Morocco (68.6%) [45], in isolates of the LAM family in Cameroon [30] and also in Korea (49.1%) [46]. In INHR strains, neither insertions nor complete deletions of katG were found, which is evidence of the rare occurrence of these mutations in clinical isolates, although they were reported previously by other authors [47, 48]. Fourteen (31.8%) INHR isolates did not show mutations at the four loci analyzed. This discrepancy between the phenotypic results and the genotypic drug resistance tests could be attributed to the presence of other mutations located either outside the selected target region or the selected genes. Several others studies have reported that mutations in inhA or its promoter region are usually associated with low-level resistance of INH. Moreover, INH-resistant isolates with inhA mutations can have additional mutations in katG, conferring higher levels of INH-resistance [11].
All mutations found in fabG1-inhA promoter region were not associated with phenotypic resistance. The substitution of G to C at position -47 first described by Homolka and al. [21] in an INH-resistant strain has been found in both susceptible (24/44; 54.5%) and resistant isolates (5/44; 11.4%). Thus, this mutation seems to not correlate with INH-resistance. The mutation -102 C → T not yet described is also not relevant to INH-resistance since it was found only in susceptible isolates.
The analysis of SM-resistance mechanism revealed that none of the SM-resistant strains carried a mutation in the rrs gene although those mutations have been described as main resistance mechanism that confer high level SM -resistance [12]. Clinical isolates showing no mutations in rpsL or rrs gene have been reported in the literature [49]. A previous investigation from Cameroon encountered rpsL or rrs mutations in SM-resistant isolates from the Central Region of Cameroon [50]. In contrast in the current investigation only rpsL mutations were associated with SM-resistance. This indicates that further studies are necessary to delineate the molecular markers for SM-resistance. Mutations in the rpsL locus have been hypothesized to be an alternative mechanism of SM-resistance like mutations in the gidB[51] or efflux pumps [13]. Overall, we detected gidB mutations in 18.5% of SM-resistant isolates and 6% of SM susceptible isolates. Although the encountered mutations in resistant samples were not observed in susceptible isolates, their association with SM-resistance needs to be confirmed.
Three contiguous genes encoding arabinosyl transferases and designated embC, embA, and embB were analyzed in the present study. These 3 genes have been identified in M. tuberculosis[52]. Previous studies based on limited sequencing region containing the embCAB genes have identified mutations that result in replacement of amino acid residues and are found only in EMB-resistant organisms cultured from humans [52]. In this study, the embB analysis gene identified 1 of 2 resistant isolates with EMB-resistance-associated nucleotide substitutions in codon 306ATG → GTG that result in amino acid replacement (Met → Val). This is in accordance with others studies analyzing EMB-resistant clinical isolates of M. tuberculosis that identified embB amino acid-conferring mutations in approximately 50 to 70% isolates with resistance-associated polymorphisms [52]. Certain variations affecting embA (330CTG → TTG) and embC (-20A → C and -230 A → C) appeared to be not associated with drug resistance. Given the low number of EMB-resistant isolates in our investigation further studies are needed to confirm these findings.
Conclusion
This study provided the first molecular characterization of M. tuberculosis drug resistance in the Central Region of Cameroon using DNA sequencing. rpoB and katG315 mutations known to be involved in resistance had high specificities and sensitivities for detecting RIF- and INH-resistance respectively. However, the correlation between molecular and phenotypic resistance testing for the determination of SM- and EMB-resistance was lower. This study clearly shows the need for continuous phenotypic and genotypic characterization of drug resistance at the national level in order to determine the most suitable molecular marker for drug resistance in our setting. The fact that mutations at codon katG315 and at the rpoB gene show high specificities for resistance against INH or RIF respectively suggests that these may be suitable molecular marker for diagnostic test in Cameroon. Consequently the WHO recommended GeneXpert technology is appropriate for the detection RIF-resistance in the Central Region of Cameroon.
Abbreviations
- TB:
-
Tuberculosis
- MDR:
-
Multi-drug resistance
- SLD:
-
Second-line drug
- DOTS:
-
Directly observed treatment short course
- HIV:
-
Human immunodeficiency virus
- ATCC:
-
American type culture collection
- INH:
-
Isoniazid
- RIF:
-
Rifampicin
- SM:
-
Streptomycin
- EMB:
-
Ethambutol
- AST:
-
Antimicrobial susceptibility testing
- MIC:
-
Minimal inhibitory concentration
- DNA:
-
Désoxyribonucleic acid
- CANTAM:
-
Central Africa Network on Tuberculosis, AIDS/HIV and Malaria
- RRDR:
-
Rifampicin resistant determining region.
References
Cauthen GM, Dooley SW, Onorato IM, Ihle WW, Burr JM, Bigler WJ, Witte J, Castro KG:Transmission ofMycobacterium tuberculosisfrom tuberculosis patients with HIV infection or AIDS.Am J Epidemiol. 1996, 144 (1): 69-77.
Gandhi NR, Moll A, Sturm AW, Pawinski R, Govender T, Lalloo U, Zeller K, Andrews J, Friedland G: Extensively drug-resistant tuberculosis as a cause of death in patients co-infected with tuberculosis and HIV in a rural area of South Africa. Lancet. 2006, 368 (9547): 1575-1580.
WHO: Global Tuberculosis Control: WHO Report 2011. 2011, Geneva, Switzerland: WHO/HTM/TB/2011.16
WHO: Global Tuberculosis Report 2012. 2012, Geneva Switzerland: WHO/HTM/TB/20126
Gillespie SH: Evolution of drug resistance in Mycobacterium tuberculosis: clinical and molecular perspective. Antimicrob Agents Chemother. 2002, 46 (2): 267-274.
Shah NS, Richardson J, Moodley P, Moodley S, Babaria P, Ramtahal M, Heysell SK, Li X, Moll AP, Friedland G, Sturm AW, Gandhi NR: Increasing drug resistance in extensively drug-resistant tuberculosis South Africa. Emerg Infect Dis. 2011, 17 (3): 510-513.
Cole ST, Brosch R, Parkhill J, Garnier T, Churcher C, Harris D, Gordon SV, Eiglmeier K, Gas S, Barry CE, Tekaia F, Badcock K, Basham D, Brown D, Chillingworth T, Connor R, Davies R, Devlin K, Feltwell T, Gentles S, Hamlin N, Holroyd S, Hornsby T, Jagels K, Krogh A, McLean J, Moule S, Murphy L, Oliver K, Osborne J, Quail MA, Rajandream MA, Rogers J, Rutter S, Seeger K, Skelton J, Squares R, Squares S, Sulston JE, Taylor K, Whitehead S, Barrell BG:Deciphering the biology ofMycobacterium tuberculosisfrom the complete genome sequence.Nature. 1998, 393 (6685): 537-544.
Shamputa IC, Rigouts L, Portaels F: Molecular genetic methods for diagnosis and antibiotic resistance detection of mycobacteria from clinical specimens. APMIS. 2004, 112 (11–12): 728-752.
Boehme CC, Nabeta P, Hillemann D, Nicol MP, Shenai S, Krapp F, Allen J, Tahirli R, Blakemore R, Rustomjee R, Milovic A, Jones M, O'Brien SM, Persing DH, Ruesch-Gerdes S, Gotuzzo E, Rodrigues C, Alland D, Perkins MD: Rapid molecular detection of tuberculosis and rifampin resistance. N Engl J Med. 2010, 363 (11): 1005-1015.
Garcia De Viedma D: Rapid detection of resistance in Mycobacterium tuberculosis: a review discussing molecular approaches. Clin Microbiol Infect. 2003, 9 (5): 349-359.
Zhang Y, Yew WW:Mechanisms of drug resistance inMycobacterium tuberculosis.Int J Tuberc Lung Dis. 2009, 13 (11): 1320-1330.
Sreevatsan S, Pan X, Stockbauer KE, Williams DL, Kreiswirth BN, Musser JM:Characterization of rpsL and rrs mutations in streptomycin-resistantMycobacterium tuberculosisisolates from diverse geographic localities.Antimicrob Agents Chemother. 1996, 40 (4): 1024-1026.
Okamoto S, Tamaru A, Nakajima C, Nishimura K, Tanaka Y, Tokuyama S, Suzuki Y, Ochi K: Loss of a conserved 7-methylguanosine modification in 16S rRNA confers low-level streptomycin resistance in bacteria. Mol Microbiol. 2007, 63 (4): 1096-1106.
Plinke C, Rüsch-Gerdes S, Niemann S:Significance of mutations inembBcodon 306 for prediction of ethambutol resistance in clinicalMycobacterium tuberculosisisolates.Antimicrob Agents Chemother. 2006, 50 (5): 1900-1902.
Ramaswamy S, Musser JM: Molecular genetic basis of antimicrobial agent resistance in Mycobacterium tuberculosis: 1998 update. Tuber Lung Dis. 1998, 79 (1): 3-29.
Plinke C, Cox H, Zarkua N, Karimovich H, Braker K, Diel R, Rüsch-Gerdes S, Feuerriegel S, Niemann S:embCAB sequence variation among ethambutol-resistantMycobacterium tuberculosisisolates without embB306 mutation.J Antimicrob Chemother. 2010, 65: 1359-1367.
Jadaun GPS, Das R, Prashant U, Chauhan DS, Charma VD, Katoch VM: Role of embCAB gene mutations in ethambutol resistance in Mycobacterium tuberculosis isolates from India. Int J Antimicrob Agents. 2009, 33: 483-486.
Dalla Costa ER, Ribeiro MO, Silva MS, Arnold LS, Rostirolla DC, Cafrune PI, Espinoza RC, Palaci M, Telles MA, Ritacco V, Suffys PN, Lopes ML, Campelo CL, Miranda SS, Kremer K, da Silva PE, Fonseca Lde S, Ho JL, Kritski AL, Rossetti ML:Correlations of mutations in katG, oxyR-ahpC and inhA genes and in vitro susceptibility inMycobacterium tuberculosisclinical strains segregated by spoligotype families from tuberculosis prevalent countries in South America.BMC Microbiol. 2009, 9: 39-
Dolgin E: African networks launch to boost clinical trial capacity. Nat Med. 2010, 16 (1): 8-
Canetti G, Fox W, Khomenko A, Mahler HT, Menon NK, Mitchison DA, Rist N, Smelev NA: Advances in techniques of testing mycobacterial drug sensitivity, and the use of sensitivity tests in tuberculosis control programmes. Bull World Health Organ. 1969, 41 (1): 21-43.
Homolka S, Meyer CG, Hillemann D, Owusu-Dabo E, Adjei O, Horstmann RD, Browne EN, Chinbuah A, Osei I, Gyapong J, Kubica T, Ruesch-Gerdes S, Niemann S:Unequal distribution of resistance-conferring mutations amongMycobacterium tuberculosisandMycobacterium africanumstrains from Ghana.Int J Med Microbiol. 2010, 300 (7): 489-495.
Sreevatsan S, Stockbauer KE, Pan X, Kreiswirth BN, Moghazeh SL, Jacobs WR, Telenti A, Musser JM:Ethambutol resistance inMycobacterium tuberculosis: critical role of embB mutations.Antimicrob Agents Chemother. 1997, 41 (8): 1677-1681.
Srivastavaa S, Ayyagaria A, Dholea TN, Nyatia KK, Dwivedi SK:Emb nucleotide polymorphisms and the role ofembB306mutations inMycobacterium tuberculosisresistance to ethambutol.Int J Med Microbiol. 2009, 299: 269-280.
Abbadi SH, Sameaa GA, Morlock G, Cooksey RC:Molecular identification of mutations associated with anti-tuberculosis drug resistance among strains ofMycobacterium tuberculosis.Int J Infect Dis. 2009, 13 (6): 673-678.
Nakiyingi L, Nankabirwa H, Lamorde M: Tuberculosis diagnosis in resource-limited settings: clinical use of GeneXpert in the diagnosis of smear-negative PTB: a case report. Afr Health Sci. 2013, 13 (2): 522-524.
Afanas’ev MV, Ikryannikova LN, Il’ina EN, Sidorenko SV, Kuz’min AV, Larionova EE, Smirnova TG, Chernousova LN, Kamaev EY, Skorniakov SN, Kinsht VN, Cherednichenko AG, Govorun VM:Molecular characteristics of rifampicin- and isoniazid-resistantMycobacterium tuberculosisisolates from the Russian Federation.J Antimicrob Chemother. 2007, 59 (6): 1057-1064.
Campbell PJ, Morlock GP, Sikes RD, Dalton TL, Metchock B, Starks AM, Hooks DP, Cowan LS, Plikaytis BB, Posey JE:Molecular detection of mutations associated with first and second-line drug resistance compared with conventional drug susceptibility testing inM. tuberculosis.Antimicrob Agents Chemother. 2011, 55 (5): 2032-2041.
Soudani A, Hadjfredj S, Zribi M, Masmoudi A, Messaoud T, Tiouri H, Fendri C:Characterization of TunisianMycobacterium tuberculosisrifampin-resistant clinical isolates.J Clin Microbiol. 2007, 45 (9): 3095-3097.
Hillemann D, Weizenegger M, Kubica T, Richter E, Niemann S:Use of the genotype MTBDR assay for rapid detection of rifampin and isoniazid resistance inMycobacterium tuberculosiscomplex isolates.J Clin Microbiol. 2005, 43 (8): 3699-3703.
Penlap BV, Victor T, Warren R, Jordaan A, Tedom ES, Titanji V:Evidence of drug resistance among the LAM-Cameroon family inMycobacterium tuberculosisisolates from Yaoundé Cameroon.Cam J Acad Sc. 2010, 9 (1): 11-15.
Taniguchi H, Aramaki H, Nikaido Y, Mizuguchi Y, Nakamura M, Koga T, Yoshida S:Rifampicin resistance and mutation of the rpoB gene inMycobacterium tuberculosis.FEMS Microbiol Lett. 1996, 144 (1): 103-108.
Pozzi G, Meloni M, Iona E, Orru G, Thoresen OF, Ricci ML, Oggioni MR, Fattorini L, Orefici G: rpoB mutations in multidrug-resistant strains of Mycobacterium tuberculosis isolated in Italy. J Clin Microbiol. 1999, 37 (4): 1197-1199.
Qian L, Abe C, Lin TP, Yu MC, Cho SN, Wang S, Douglas JT:rpoB genotypes ofMycobacterium tuberculosisBeijing family isolates from East Asian countries.J Clin Microbiol. 2002, 40 (3): 1091-1094.
Zaczek A, Brzostek A, Augustynowicz-Kopec E, Zwolska Z, Dziadek J:Genetic evaluation of relationship between mutations inrpoBand resistance ofMycobacterium tuberculosisto rifampin.BMC Microbiol. 2009, 9: 10-
Telenti A, Imboden P, Marchesi F, Lowrie D, Cole S, Colston MJ, Matter L, Schopfer K, Bodmer T:Detection of rifampicin-resistance mutations inMycobacterium tuberculosis.Lancet. 1993, 341 (8846): 647-650.
Williams DL, Waguespack C, Eisenach K, Crawford JT, Portaels F, Salfinger M, Nolan CM, Abe C, Sticht-Groh V, Gillis TP: Characterization of rifampin-resistance in pathogenic mycobacteria. Antimicrob Agents Chemother. 1994, 38 (10): 2380-2386.
Ohno H, Koga H, Kohno S, Tashiro T, Hara K:Relationship between rifampin MICs for and rpoB mutations ofMycobacterium tuberculosisstrains isolated in Japan.Antimicrob Agents Chemother. 1996, 40 (4): 1053-1056.
Mani C, Selvakumar N, Narayanan S, Narayanan PR:Mutations in the rpoB gene of multidrug-resistantMycobacterium tuberculosisclinical isolates from India.J Clin Microbiol. 2001, 39 (8): 2987-2990.
Johnson R, Streicher EM, Louw GE, Warren RM, van Helden PD, Victor TC:Drug Resistance inMycobacterium tuberculosis.Curr Issues Mol Biol. 2009, 8: 97-112.
Mokrousov I, Narvskaya O, Otten T, Limeschenko E, Steklova L, Vyshnevskiy B:High prevalence of KatG Ser315Thr substitution among isoniazid-resistantMycobacterium tuberculosisclinical isolates from northwestern Russia, 1996 to 2001.Antimicrob Agents Chemother. 2002, 46 (5): 1417-1424.
Sajduda A, Brzostek A, Poplawska M, Augustynowicz-Kopec E, Zwolska Z, Niemann S, Dziadek J, Hillemann D:Molecular characterization of rifampin- and isoniazid-resistantMycobacterium tuberculosisstrains isolated in Poland.J Clin Microbiol. 2004, 42 (6): 2425-2431.
van Doorn HR, An DD, de Jong MD, Lan NT, Hoa DV, Quy HT, Chau NV, Duy PM, Tho DQ, Chinh NT, Farrar JJ, Caws M:Fluoroquinolone resistance detection inMycobacterium tuberculosiswith locked nucleic acid probe real-time PCR.Int J Tuberc Lung Dis. 2008, 12 (7): 736-742.
Bakonyte D, Baranauskaite A, Cicenaite J, Sosnovskaja A, Stakenas P:Molecular characterization of isoniazid-resistantMycobacterium tuberculosisclinical isolates in Lithuania.Antimicrob Agents Chemother. 2003, 47 (6): 2009-2011.
Tudo G, Gonzalez J, Obama R, Rodriguez JM, Franco JR, Espasa M, Simarro PR, Escaramis G, Ascaso C, Garcia A, Jimenez De Anta MT: Study of resistance to anti-tuberculosis drugs in five districts of Equatorial Guinea: rates, risk factors, genotyping of gene mutations and molecular epidemiology. Int J Tuberc Lung Dis. 2004, 8 (1): 15-22.
Chaoui I, Sabouni R, Kourout M, Jordaan AM, Lahlou O, Elouad R, Akrim M, Victor TC, El Mzibri M:Analysis of isoniazid, streptomycin and ethambutol resistance inMycobacterium tuberculosisisolates from Morocco.J Infect Dev Ctries. 2009, 3 (4): 278-284.
Cho EH, Bae HK, Kang SK, Lee EH:Detection of isoniazid and rifampicin resistance by sequencing ofkatG, inhA,andrpoBgenes in Korea.Korean J Lab Med. 2009, 29 (5): 455-460.
Siddiqi N, Shamim M, Hussain S, Choudhary RK, Ahmed N, Prachee BS, Savithri GR, Alam M, Pathak N, Amin A, Hanief M, Katoch VM, Sharma SK, Hasnain SE:Molecular characterization of multidrug-resistant isolates ofMycobacterium tuberculosisfrom patients in North India.Antimicrob Agents Chemother. 2002, 46 (2): 443-450.
Torres MJ, Criado A, Gonzalez N, Palomares JC, Aznar J:Rifampin and isoniazid resistance associated mutations inMycobacterium tuberculosisclinical isolates in Seville Spain.Int J Tuberc Lung Dis. 2002, 6 (2): 160-163.
Tudo G, Rey E, Borrell S, Alcaide F, Codina G, Coll P, Martin-Casabona N, Montemayor M, Moure R, Orcau A, Salvado M, Vicente E, Gonzalez-Martin J:Characterization of mutations in streptomycin-resistantMycobacterium tuberculosisclinical isolates in the area of Barcelona.J Antimicrob Chemother. 2010, 65 (11): 2341-2346.
Mbacham FW, Tientcheu LD, Beng Penlap V, Kuaban C, Eyangoh S, Wang H, Bickii J, Netongo PM, Titi Lembe W, Olama A, Njikam N, Teyim P, Khan B:Detection of resistance-associated mutations inMycobacterium tuberculosisisolates in Cameroon using a dot-blot hybridisation technique.Afr J Biotechnol. 2011, 10 (53): 11016-11022.
Silva PE, Bigi F, Santangelo MP, Romano MI, Martin C, Cataldi A, Ainsa JA:Characterization of P55, a multidrug efflux pump inMycobacterium bovisandMycobacterium tuberculosis.Antimicrob Agents Chemother. 2001, 45 (3): 800-804.
Telenti A, Philipp WJ, Sreevatsan S, Bernasconi C, Stockbauer KE, Wieles B, Musser JM, Jacobs WR:Theemboperon, a gene cluster ofMycobacterium tuberculosisinvolved in resistance to ethambutol.Nat Med. 1997, 3 (5): 567-570.
Acknowledgements
This study was financially supported by CANTAM EDCTP grant N° CB.2007.41700.006. Emmanuel Mouafo Tekwu and Larissa Kamgue Sidze were research fellow students at the Institute for Tropical Medicine in Tübingen (Germany). Veronique Penlap Beng, Francine Ntoumi, Emmanuel Mouafo Tekwu, Larissa Kamgue Sidze, Jean-Paul Assam Assam and Matthias Frank were supported by the DAAD PAGEL-Program of the University of Tübingen to attend expert meetings and workhops throughout the duration of the project. We thank Mrs Augusta Tsasse, the technician at the Centre Pasteur of Yaoundé; Dr Ellen Bruske and Mrs Andrea Weierich of the University of Tübingen (Germany) for their technical assistance.
Author information
Authors and Affiliations
Corresponding authors
Additional information
Competing interests
The authors declare there are no competing interests.
Authors’ contributions
EMT and LKS contributed equally, they carried out all the molecular analysis as Ph.D students, participated in field work and drafted the manuscript. JPAA, JCT, ST, GGM, ALTW participated in field work and revised the manuscript. CK participated in the conception, design and supervision of field work. SE supervised mycobacteria culture and DST. FN is the coordinator and project manager of the CANTAM network. She revised the manuscript. VNPB is the Workpackage Leader of the CANTAM-TB project. She was the overall supervisor and chief designer of the project and critically revised the manuscript. MF is the Co-Workpackage Leader of CANTAM-TB project and Coordinator of the DAAD PAGEL-Program of the University of Tübingen. He designed and supervised the molecular analysis and critically revised the manuscript. All authors read and approved the final manuscript before submission.
Emmanuel Mouafo Tekwu, Larissa Kamgue Sidze contributed equally to this work.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Tekwu, E.M., Sidze, L.K., Assam, JP.A. et al. Sequence analysis for detection of drug resistance in Mycobacterium tuberculosis complex isolates from the Central Region of Cameroon. BMC Microbiol 14, 113 (2014). https://doi.org/10.1186/1471-2180-14-113
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2180-14-113