
Abstract
Background
Reduced gas transfer in patients with pulmonary arterial hypertension (PAH) is traditionally attributed to remodeling and progressive loss of pulmonary arterial vasculature that results in decreased capillary blood volume available for gas exchange.
Methods
We tested this hypothesis by determination of lung diffusing capacity (DL) and its components, the alveolar capillary membrane diffusing capacity (Dm) and lung capillary blood volume (Vc) in 28 individuals with PAH in comparison to 41 healthy individuals, and in 19 PAH patients over time. Using single breath simultaneous measure of diffusion of carbon monoxide (DLCO) and nitric oxide (DLNO), DL and Dm were respectively determined, and Vc calculated. Dm and Vc were evaluated over time in relation to standard clinical indicators of disease severity, including brain natriuretic peptide (BNP), 6-minute walk distance (6MWD) and right ventricular systolic pressure (RVSP) by echocardiography.
Results
Both DLCO and DLNO were reduced in PAH as compared to controls and the lower DL in PAH was due to loss of both Dm and Vc (all p < 0.01). While DLCO of PAH patients did not change over time, DLNO decreased by 24 ml/min/mmHg/year (p = 0.01). Consequently, Dm decreased and Vc tended to increase over time, which led to deterioration of the Dm/Vc ratio, a measure of alveolar-capillary membrane functional efficiency without changes in clinical markers.
Conclusions
The findings indicate that lower than normal gas transfer in PAH is due to loss of both Dm and Vc, but that deterioration of Dm/Vc over time is related to worsening membrane diffusion.
Similar content being viewed by others


Background
Lung diffusing capacity for carbon monoxide (DLCO) is a valuable clinical tool in the assessment of pulmonary diseases. It measures the ability of the lungs to transfer gas from the alveolar space to the red blood cells in the pulmonary vessels. Measurement of DL is informative for pathophysiologic diagnoses of lung diseases and serial measurements are used to follow the course of disease [1]. The components of DL can provide more detailed knowledge of the mechanisms of loss of gas exchange capacity. Based on the Roughton and Forster model [2], DLCO is described as a series of resistances: the diffusion of the gas across the alveolar-capillary membrane, the transfer into the plasma and across the red blood cell membrane, and the chemical reaction of the gas with hemoglobin (Hgb). The following equation summarizes these concepts:
Where DL represents total lung diffusing capacity; Dm alveolar-capillary membrane diffusing capacity; Vc pulmonary capillary bed available for gas transfer; and θ is the rate of reaction of the gas with the red cell. Traditionally, measure of the two components of DLCO relied upon repeated performance of the test at different oxygen concentrations and solving the equation for Dm and Vc. These technical challenges resulted in an arduous method and inaccuracies in measures that limited utility. However, nitric oxide (NO) has a greater affinity to Hgb compared to CO or O2, and thus NO diffusion is mainly limited by the transfer of gas across the alveolar capillary membrane [3]. Based on this, DLNO can be used as a direct measure of Dm. Recent advances allow measure of DLNO and DLCO simultaneously and direct determination of Dm and Vc from single breath maneuver at one oxygen tension [3, 4]. Few studies have evaluated the components of DL in pulmonary hypertension (PH) in an attempt to understand the pathophysiology of the decreased DL. Cross-sectional data from studies are inconsistent and there are no longitudinal data. In 1968, Nadel et al. showed that DLCO was reduced in PH as a result of low Vc [5]. Borland et al. were the first to apply a single breath technique to measure DLNO and DLCO and identified that both were reduced in PH [6]. However, recent studies have attributed the low DL to a loss of Dm rather than Vc [7, 8]. Oppenhiemer et al. measured Dm and Vc in different groups of PH patients and found that Dm was reduced out of proportion to Vc as shown by a reduction in the ratio of Dm/Vc[9]. Measuring the components of DL in PAH would give insight into the disease, especially that recent advances have unveiled the intricacy of the pathogenesis of PAH. We hypothesized that both Dm and Vc are decreased in PAH patients and that there is progressive decline of DL and its components over time in parallel to disease progression. To test this, DLNO and DLCO were measured by single breath technique in PAH patients in comparison to healthy controls and over time in order to evaluate changes in Dm and Vc in relation to clinical parameters including echocardiography, 6MWD and BNP levels.
Materials and methods
41 healthy controls and 28 subjects with PAH were enrolled in the study. The Institutional Review Board at the Cleveland Clinic approved the study and all subjects gave written informed consent (IRB 7853). Healthy controls were recruited from the community, had no medical problems and were on no medications. PAH subjects were recruited from the PH clinic. They had an established diagnosis of PAH based on right heart catheterization. Their medical records were reviewed to verify diagnosis. Clinical data including 6MWD, BNP, complete cell count and metabolic panel were collected from the medical records when available. Lung function testing including spirometry, lung volumes, DLCO and DLNO as well as exhaled NO and echocardiogram were measured as part of the study. These tests were repeated longitudinally for a subgroup of PAH patients.
Exhaled NO, lung function, volumes and diffusing capacity for carbon monoxide and nitric oxide
Single-breath on-line measurement of fractional NO concentration in expired breath (FENO) was measured at the beginning of each visit using the NIOX (Aerocrine, NJ) [10].
The forced expiratory volume at 1 second (FEV1) and vital capacity (FVC) were measured by spirometry (MasterLab; Viasys/Jaeger; Höchberg, Germany) following established guidelines [11]. Total lung capacity (TLC) was measured using the single breath measurement method [12]. Helium was used as a tracer gas following the ATS/ERS guidelines.
Single breath measurements of DLCO and DLNO were performed using a modified Masterscreen PFT (Viasys/Jaeger; Höchberg, Germany) adapted to measure nitric oxide. The measurement was performed with the patient rested in a seated position using a nose clip. The inspired gas contained 70 ppm nitric oxide (Ikara, NJ) and a blend of ultra high purity 21% oxygen, 0.28% carbon monoxide, 9.5% helium and balance nitrogen. The single breath DLCO method was performed in duplicate to a maximum of 4 measurements to obtain 2 measurements within 5%, ~4 minutes apart using a washout volume of 750 ml and an alveolar volume of 750 ml per standard guidelines [1, 13]. The breathhold time was ~6 seconds [13]. The instrument was calibrated daily. DmCO was calculated as DLNO divided by 1.97 based on solubility factors for CO and NO respectively of 0.0183 and 0.0364 [14].
Vc was calculated from the following formula [2]:
Echocardiogram
Two dimensional echocardiograms and doppler exams were performed on the same day as the DL test or in some cases (mainly for the first visit) within up to 8 weeks of the DL test for convenience of the participant.
Echocardiographic analysis
All echocardiographic analysis were performed following the American Society of Echocardiography Guidelines and Standards [15].
From the parasternal long axis view the Interventricular septal (IVS) thickness in end-diastole, left ventricular end-diastolic dimension (LVEDD), left ventricular end-systolic dimension (LVESD) and posterior wall thickness in diastole were measured from the 2D parasternal long axis image following ASE guidelines. Left ventricular (LV) mass was determined from 2D measurements using the cubed formula:
LV function: LV ejection fraction was determined by visual assessment, and/or apical biplane volumes. LV end-diastolic and end-systolic volumes were calculated from the apical 4 and 2 chamber views using the modified Simpson method. LV fractional shortening was determined from parasternal 2D analysis as [(LVEDD-LVESD)/LVEDD] × 100.
Right ventricular (RV) function: RV end-diastolic area (RVAD) and end-systolic area (RVAS) were measured in the apical 4-chamber view by tracing the endocardial border of the RV and the tricuspid annular plane. RV fractional area change was calculated as follows:
Right atrial volume was measured in the apical 4 chamber view by using the single plane area length method.
The right ventricular systolic pressure (RVSP) was estimated from the systolic pressure gradient between the RV and the right atrium by the peak continuous-wave Doppler velocity of the TR jet using the modified Bernoulli equation plus estimated right atrial pressure (RAP). RAP was estimated from the subcostal window approach measuring changes in inferior vena caval size and collapsibility as determined by the respiratory sniff test following ASE guidelines.
Echo-Doppler estimation of pulmonary vascular resistance (PVR): The highest Doppler continuous wave tricuspid valve peak velocity jet obtained from multiple views (parasternal long axis, parasternal short axis, apical 4 chamber, subcostal or apical off-axis imaging) was determined as the maximum tricuspid regurgitant velocity (TRV). Pulsed wave Doppler sample was placed in the right ventricular outflow tract (RVOT) at the level of the aortic valve in the parasternal short axis view just below the pulmonic valve so that pulmonic valve closure is identified. The Doppler spectrum was traced to determine the time velocity integral of the RVOT (RVOT-TVI). PVR calculation was determined by:
Statistics
For PAH patients, individual patient slopes representing changes over actual time were calculated using linear regression for each continuous study variable. For individual variables, Wilcoxon signed rank tests were used to test the null hypotheses of zero mean slopes for the PAH patients. The 2 groups were compared with respect to baseline variables using Fisher's exact and chi-square tests for categorical variables, and Kruskal-Wallis and Wilcoxon rank sum tests for quantitative variables. Spearman correlation coefficients measured at specified time points, were used to describe relationships among pairs of quantitative variables in a manner free of the normality assumption. All analyses were performd using R version 2.4.1. (R Development Core Team (2011). R Foundation for Statistical Computing, Vienna, Austria. ISBN 3-900051-07-0, URL http://www.R-project.org/).
Results
Patients were classified according to Dana Point classification of pulmonary hypertension: Class 1.1 (n = 21) 75%, Class 1.2 (n = 3) 10.7%, Class 1.3 (n = 1) 3.6% and Class 1.4 (n = 3) 10.7%. Three patients were Class 1.4 and respectively had systemic sclerosis, lupus and chronic hemolytic anemia. None of the PAH patients had interstitial lung disease or obstructive lung disease based on clinical history, exam, computerized chest tomography imaging, as part of the evaluation and assignment of PAH class. One patient had mild pulmonary edema on chest X-ray. Height, weight and gender distribution was similar among PAH patients and controls; however, PAH patients were older (p < 0.01). Table 1 shows the baseline characteristics of the two groups and Table 2 lists the clinical data of the PAH patients. The study spanned 15 months with a mean time of 5 months between visit 1 and visit 2 and of 4 months between visit 2 and visit 3. Twenty-eight PAH patients were evaluated at baseline, of those 19 elected to continue with the longitudinal study and were followed over time. Fourteen patients completed all 3 visits. There was no difference in baseline characteristics between the patients who were followed longitudinally and those who were not. The patients followed longitudinally had mainly idiopathic PAH [Class 1.1 (N = 15) 79%, Class 1.2 (N = 2) 11%, Class 1.3 (N = 1) 5% and Class 1.4 (N = 1) 5%]. During the time span of the study, none of the PAH patients developed new findings on chest imaging performed as part of their clinical follow up.
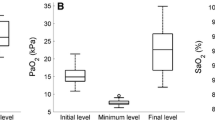
Airflow and diffusion capacity
Oxygen saturation at rest was lower in PAH patients compared to controls [Table 1. PAH patients had reduced airflow as compared to controls [Table 1. As previously reported in PAH patients treated with prostacyclins [16, 17], exhaled NO of patients was similar to controls [Table 1. DL measured by CO or NO was lower in PAH as in previous reports [Table 1. The alveolar volume was not different in PAH compared to controls [Table 1. DL corrected for VA was reduced in PAH compared to controls [DLCO/VA (1/min/mmHg): PAH 3.9 ± 0.1, controls 5 ± 0.1; p < 0.01, DLNO/VA (1/min/mmHg): PAH 14.9 ± 0.7, controls 19.3 ± 0.4; p < 0.01]. Similarly, DL corrected for Hgb was lower in PAH [DLCO corrected for Hgb (ml/min/mmHg): PAH 17.3 ± 1.0, controls 23.6 ± 1.3; p < 0.01, DLNO corrected for Hgb (ml/min/mmHg): PAH 65.5 ± 4.5, controls 90.4 ± 5.0; p < 0.01]. Both Dm and Vc were reduced in PAH [Table 1. To delineate whether proportionate loss was accountable for the lower DL in PAH, the ratio of Dm/Vc was calculated. The ratio was similar between the two groups, suggesting a proportionate loss of Dm and Vc in PAH [Table 1. Mean variabilities of DLCO and DLNO for healthy controls were 3% and 5% respectively and for PAH 4% and 7%.
Dm and Vcin subjects with PAH over time
Although DLCO was stable over time [median DLCO = −1.2 ml/min/mmHg/year (IQR −2.8, 1.5), Wilcoxon SR p = 0.7], there was a significant decline in DLNO and hence Dm [median DLNO = −23.8 ml/min/mmHg/year (IQR −36.8, -9.9), Wilcoxon SR p = 0.01] [median Dm = −11.9 ml/min/mmHg/year (IQR −18.5, -4.3), Wilcoxon SR p = 0.01] (Figure 1) [Table 3]. On the other hand, Vc tended to increase over time, accounting for stability of DLCO [median Vc = 10.9 ml/year (IQR 4.2, 46.9), Wilcoxon SR p = 0.07] (Figure 1). The ratio of Dm/Vc decreased over time, which indicated a disproportionate loss of membrane diffusion compared to capillary bed [median Dm/Vc = −0.4 1/min/mmHg/year (IQR −0.5, -0.05), Wilcoxon SR p = 0.04] [Table 3]. Hgb did not vary over time [Table 3]. Likewise, DLCO corrected for Hgb did not vary significantly (Wilcoxon SR p = 0.3) whereas DLNO corrected for Hgb decreased (Wilcoxon SR p < 0.01). The alveolar volume did not change over time (Wilcoxon SR p = 0.4) [Table 3].

Lung diffusion capacity and its components over time in pulmonary arterial hypertension. Lung diffusing capacity for NO (DLNO) and the alveolar-capillary membrane diffusing capacity (Dm) decreases over time (both p = 0.01). Lung capillary blood volume (Vc) tends to increase over time (p = 0.07). Conversely, DLCO did not change significantly (p = 0.7).
The rest of the lung functions measured and exhaled NO did not vary (all Wilcoxon SR p > 0.05).
Changes in clinical parameters over time
Baseline clinical data for the PAH patients are summarized in Table 2. Right heart catheterization data were retrieved from the medical records and the most recent one was used. Some (N = 15) were performed within the same year, however others were performed in past years. Clinical parameters including echocardiogram, 6MWD and BNP, did not decline significantly over time of the study. At baseline, DLNO and Dm did not correlate with clinical markers [Table 4]. BNP was associated with Vc and Dm/ Vc (Vc: Spearman R = 0.5, p = 0.02; Dm/ Vc: Spearman R = −0.5, p = 0.03) (Figure 2) at visit 1 but not at visit 2 or 3 (p > 0.1). In addition, Vc was inversely related to RV function (RVAD: Spearman R = 0.4, p = 0.05, RVAS: Spearman R = 0.4, p = 0.04) suggesting that Vc increases with worsening PAH/RV function. Vc and RV fractional area change did not correlate significantly (Spearman R = −0.4, p = 0.09). DL and its components did not correlate with left ventricular systolic and diastolic function (all p > 0.1). DLCO correlated with the 6MWD (Spearman R = 0.5, p = 0.05) [Table 4].

Association of brain natriuretic peptide (BNP) to lung capillary blood volume (V c ) and to the ratio of membrane diffusing capacity (D m ) and V c . Dm/Vc is inversely related to disease severity measured by BNP whereas Vc correlates directly to BNP. The points represent measurements obtained at time of first visit.
Discussion
This is the first longitudinal study to describe the changes in gas transfer in PAH over time. Lung diffusing capacity for NO, but not CO, dropped due to the disproportionate loss of membrane diffusion, Dm, as compared to changes in the vascular bed available for gas exchange, Vc. These findings suggest that the efficiency of the alveolar-capillary unit in PAH worsens over time independent of traditional clinical and echocardiographic measures. The results also put forward the potential utility of DLNO in tracking progression of disease in PAH.
As in prior work, DL was reduced in PAH patients. Although PAH patients and controls were not well matched by age and gender, the decrease in DL is not likely explained by age and gender alone. Earlier studies measured DLCO at two different oxygen concentrations and calculated Dm and Vc except for the study by Borland et al. where the single breath test measuring both CO and NO uptake was used. All discovered a decrease in DL, but earlier studies showed predominant loss of Vc while more recent ones showed that Dm is reduced out of proportion to Vc. The difference between earlier studies and more recent ones could be attributed to differences in techniques or use of pulmonary vasodilators leading to higher measured Vc. In this study, the single breath technique measuring DLNO and DLCO was used to assess Dm and Vc. Dm was reduced proportionally to Vc in patients with PAH, and thus Dm/Vc was not different from controls. This confirms the interdependence of Dm and Vc in pulmonary vascular diseases and any change in the vascular bed that reduces Vc would lead to a reduction in Dm through a reduction in the surface area available to gas exchange.
In PAH, the reduction in Vc is likely multifactorial: increased pulmonary vascular resistance, decreased cardiac output and local thrombosis of the vascular bed. Mechanisms underlying the reduced Dm may include an increase in the alveolar-capillary membrane thickness caused by fibrotic or proliferative process, and/or interstitial edema. Of note, none of the patients recruited for the study had interstitial lung disease. The decreased DL in association with decreased Dm and Vc has been described in chronic heart failure patients in stable clinical condition [18]. There is growing evidence that as disease progresses; the left ventricular function may become independently compromised in PAH [19, 20]. This may contribute to the reduced DL, Dm and Vc.
Over time, the increase in Vc in association with a decrease in Dm could be explained by the effect of vasodilator therapy on the diseased pulmonary vasculature. Dm would not be expected to increase proportionally to Vc with vasodilation alone as the thickened alveolar-capillary membrane is not affected and the fibroproliferative process is not responsive to pulmonary vasodilators. Another explanation could be worsening left side function with increase pulmonary capillary pressure and congestion associated with interstitial edema. In fact, similar findings are noted in heart failure, in which acute decompensation and increased wedge pressure cause a drop in Dm paralleled by an increase in Vc[21]. Worsening RV function in PAH can lead to LV dysfunction through ventricular interdependence. Our findings showed that Vc increased with worsening RV function but there was no relation between Vc and LV function. In view of the limitations of echocardiography and the absence of repeat right heart catheterization, the contribution of LV dysfunction to the increase of Vc noted over time remains undetermined. Overall, the lack of perceptible changes in standard clinical markers highlights the limitations of available tests, and suggests the possibility that lung diffusing capacity as measured by NO, i.e. the lung Dm, may be a potential marker for disease progression in PAH. A limitation of the study is the small number of patients followed longitudinally and studies with a large cohort of PAH patients over time in correlation with clinical parameters and outcomes are needed to confirm our findings.
Evidence of airway obstruction in PAH is suggested in this study based on the decreased %FEV1 and FEV1/FVC. This is in keeping with published data that identifies peripheral airway obstruction in PAH by lung functions and pathologic findings [22–26]. Inflammation typically surrounds plexiform lesions in PAH [27] and abundant mast cells have been noted in PAH lungs [28]. Lung biopsies show small airways narrowing with thickened walls infiltrated by lymphocytes, plasma cells and polymorphonuclear leukocytes [29]. Moreover, studies reveal shared mechanistic features of asthma and PAH in experimental models [30, 31]. Thus, although PAH is defined as a pure vascular disease, impaired airflow occurs in patients on PAH therapies, suggesting a potential role for airway-directed therapies in the care of these patients.
There are several limitations to the study. Patients were recruited from our PH clinic and the research testing was done on the day of their scheduled clinical visits. Their primary physician scheduled follow up visits and adjusted PAH therapy. We had no control on the time interval between visits or on treatment. As such though most patients were stable on their PAH therapies, the effect of medications on the findings can not be excluded. Another limitation is the difference in age between the PAH and control groups. However, the novel finding here is the longitudinal changes in the PAH group. The drop in Dm over time has not been described previously. Another limitation is the lack of concurrent hemodynamic data at the time of the DL measurements. Future studies evaluating Dm and Vc in relation to hemodynamic data are essential to better understand the significance of the changes noted here.
Conclusion
In summary, a reduction in both Dm and Vc was noted in PAH patients in association with highly efficient alveolar-capillary units. However, over time, there was a drop in Dm/Vc. Although the present study does not fully unveil the clinical importance of the decline in Dm/Vc, it opens the field to further investigate the single breath measurement of DLNO/DLCO and its components in PAH.
Abbreviations
- BNP:
-
Brain natriuretic peptide
- CO:
-
Carbon monoxide
- DL:
-
Lung diffusion for carbon monoxide
- DLCO:
-
Lung diffusion for carbon monoxide
- DLNO:
-
Lung diffusion for nitric oxide
- Dm:
-
Alveolar-capillary membrane diffusing capacity
- F/M:
-
Female/male
- FENO:
-
Fractional exhaled nitric oxide
- FEV1:
-
Forced expiratory volume in one second
- FVC:
-
Forced vital capacity
- Hgb:
-
Hemoglobin
- IVS:
-
Interventricular Septal thickness
- LVEDD:
-
Left Ventricular end diastolic diameter
- LVESD:
-
Left Ventricular end systolic diameter
- NO:
-
Nitric oxide
- O2:
-
Oxygen
- PAH:
-
Pulmonary arterial hypertension
- PH:
-
Pulmonary hypertension
- PVR:
-
Pulmonary vascular resistance
- PW:
-
Posterior wall thickness
- RV:
-
Right ventricle
- RVAD:
-
Right ventricular end-diastolic area
- RVAS:
-
Right ventricular end-systolic area
- RVOT-TVI:
-
Right ventricular outflow tract-time velocity integral
- RVSP:
-
Right ventricular systolic pressure
- TLC:
-
Total lung capacity
- TRV:
-
Tricuspid regurgitant velocity
- VA:
-
Alveolar volume
- Vc:
-
Lung capillary blood volume
- 6MWD:
-
6-minute walk distance.
References
Macintyre N, Crapo RO, Viegi G, Johnson DC, van der Grinten CP, Brusasco V, Burgos F, Casaburi R, Coates A, Enright P, et al: Standardisation of the single-breath determination of carbon monoxide uptake in the lung. Eur Respir J. 2005, 26 (4): 720-735. 10.1183/09031936.05.00034905.
Roughton FJ, Forster RE: Relative importance of diffusion and chemical reaction rates in determining rate of exchange of gases in the human lung, with special reference to true diffusing capacity of pulmonary membrane and volume of blood in the lung capillaries. J Appl Physiol. 1957, 11 (2): 290-302.
Guenard H, Varene N, Vaida P: Determination of lung capillary blood volume and membrane diffusing capacity in man by the measurements of NO and CO transfer. Respir Physiol. 1987, 70 (1): 113-120. 10.1016/S0034-5687(87)80036-1.
Borland CD, Higenbottam TW: A simultaneous single breath measurement of pulmonary diffusing capacity with nitric oxide and carbon monoxide. Eur Respir J. 1989, 2 (1): 56-63.
Nadel JA, Gold WM, Burgess JH: Early diagnosis of chronic pulmonary vascular obstruction. Value of pulmonary function tests. Am J Med. 1968, 44 (1): 16-25. 10.1016/0002-9343(68)90233-7.
Borland C, Cox Y, Higenbottam T: Reduction of pulmonary capillary blood volume in patients with severe unexplained pulmonary hypertension. Thorax. 1996, 51 (8): 855-856. 10.1136/thx.51.8.855.
Bernstein RJ, Ford RL, Clausen JL, Moser KM: Membrane diffusion and capillary blood volume in chronic thromboembolic pulmonary hypertension. Chest. 1996, 110 (6): 1430-1436. 10.1378/chest.110.6.1430.
Steenhuis LH, Groen HJ, Koeter GH, van der Mark TW: Diffusion capacity and haemodynamics in primary and chronic thromboembolic pulmonary hypertension. Eur Respir J. 2000, 16 (2): 276-281. 10.1034/j.1399-3003.2000.16b15.x.
Oppenheimer BW, Berger KI, Hadjiangelis NP, Norman RG, Rapoport DM, Goldring RM: Membrane diffusion in diseases of the pulmonary vasculature. Respir Med. 2006, 100 (7): 1247-1253. 10.1016/j.rmed.2005.10.015.
ATS/ERS recommendations for standardized procedures for the online and offline measurement of exhaled lower respiratory nitric oxide and nasal nitric oxide, 2005. Am J Respir Crit Care Med. 2005, 171 (8): 912-930.
Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, Crapo R, Enright P, van der Grinten CP, Gustafsson P, et al: Standardisation of spirometry. Eur Respir J. 2005, 26 (2): 319-338. 10.1183/09031936.05.00034805.
Wanger J, Clausen JL, Coates A, Pedersen OF, Brusasco V, Burgos F, Casaburi R, Crapo R, Enright P, van der Grinten CP, et al: Standardisation of the measurement of lung volumes. Eur Respir J. 2005, 26 (3): 511-522. 10.1183/09031936.05.00035005.
Cotes J: Lung Function. 1993, Oxford: Blackwell Scientific Publications
Meyer M, Schuster KD, Schulz H, Mohr M, Piiper J: Pulmonary diffusing capacities for nitric oxide and carbon monoxide determined by rebreathing in dogs. J Appl Physiol. 1990, 68 (6): 2344-2357.
Rudski LG, Lai WW, Afilalo J, Hua L, Handschumacher MD, Chandrasekaran K, Solomon SD, Louie EK, Schiller NB: Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr. 2010, 23 (7): 685-713. 10.1016/j.echo.2010.05.010. quiz 786–688
Ozkan M, Dweik RA, Laskowski D, Arroliga AC, Erzurum SC: High levels of nitric oxide in individuals with pulmonary hypertension receiving epoprostenol therapy. Lung. 2001, 179 (4): 233-243. 10.1007/s004080000064.
Machado RF, Londhe Nerkar MV, Dweik RA, Hammel J, Janocha A, Pyle J, Laskowski D, Jennings C, Arroliga AC, Erzurum SC: Nitric oxide and pulmonary arterial pressures in pulmonary hypertension. Free Radic Biol Med. 2004, 37 (7): 1010-1017. 10.1016/j.freeradbiomed.2004.06.039.
Agostoni P, Bussotti M, Cattadori G, Margutti E, Contini M, Muratori M, Marenzi G, Fiorentini C: Gas diffusion and alveolar-capillary unit in chronic heart failure. Eur Heart J. 2006, 27 (21): 2538-2543. 10.1093/eurheartj/ehl302.
Tonelli AR, Plana JC, Heresi GA, Dweik RA: Prevalence and prognostic value of left ventricular diastolic dysfunction in idiopathic and heritable pulmonary arterial hypertension. Chest. 2012, 141 (6): 1457-1465. 10.1378/chest.11-1903.
Puwanant S, Park M, Popovic ZB, Tang WH, Farha S, George D, Sharp J, Puntawangkoon J, Loyd JE, Erzurum SC, et al: Ventricular geometry, strain, and rotational mechanics in pulmonary hypertension. Circulation. 2010, 121 (2): 259-266. 10.1161/CIRCULATIONAHA.108.844340.
Agostoni P, Cattadori G, Bianchi M, Wasserman K: Exercise-induced pulmonary edema in heart failure. Circulation. 2003, 108 (21): 2666-2671. 10.1161/01.CIR.0000097115.61309.59.
Jing ZC, Xu XQ, Badesch DB, Jiang X, Wu Y, Liu JM, Wang Y, Pan L, Li HP, Pu JL, et al: Pulmonary function testing in patients with pulmonary arterial hypertension. Respir Med. 2009, 103 (8): 1136-1142. 10.1016/j.rmed.2009.03.009.
Rastogi D, Ngai P, Barst RJ, Koumbourlis AC: Lower airway obstruction, bronchial hyperresponsiveness, and primary pulmonary hypertension in children. Pediatr Pulmonol. 2004, 37 (1): 50-55. 10.1002/ppul.10363.
Spiekerkoetter E, Fabel H, Hoeper MM: Effects of inhaled salbutamol in primary pulmonary hypertension. Eur Respir J. 2002, 20 (3): 524-528. 10.1183/09031936.02.02572001.
Meyer FJ, Ewert R, Hoeper MM, Olschewski H, Behr J, Winkler J, Wilkens H, Breuer C, Kubler W, Borst MM: Peripheral airway obstruction in primary pulmonary hypertension. Thorax. 2002, 57 (6): 473-476. 10.1136/thorax.57.6.473.
O'Hagan AR, Stillwell PC, Arroliga A: Airway responsiveness to inhaled albuterol in patients with pulmonary hypertension. Clin Pediatr. 1999, 38 (1): 27-33. 10.1177/000992289903800104.
Price LC, Wort SJ, Perros F, Dorfmuller P, Huertas A, Montani D, Cohen-Kaminsky S, Humbert M: Inflammation in pulmonary arterial hypertension. Chest. 2012, 141 (1): 210-221. 10.1378/chest.11-0793.
Heath D, Yacoub M: Lung mast cells in plexogenic pulmonary arteriopathy. J Clin Pathol. 1991, 44 (12): 1003-1006. 10.1136/jcp.44.12.1003.
Fernandez-Bonetti P, Lupi-Herrera E, Martinez-Guerra ML, Barrios R, Seoane M, Sandoval J: Peripheral airways obstruction in idiopathic pulmonary artery hypertension (primary). Chest. 1983, 83 (5): 732-738. 10.1378/chest.83.5.732.
Said SI, Hamidi SA, Gonzalez Bosc L: Asthma and pulmonary arterial hypertension: do they share a key mechanism of pathogenesis?. Eur Respir J. 2010, 35 (4): 730-734. 10.1183/09031936.00097109.
Daley E, Emson C, Guignabert C, de Waal MR, Louten J, Kurup VP, Hogaboam C, Taraseviciene-Stewart L, Voelkel NF, Rabinovitch M, et al: Pulmonary arterial remodeling induced by a Th2 immune response. J Exp Med. 2008, 205 (2): 361-372. 10.1084/jem.20071008.
Acknowledgements
Deep gratitude and appreciation to Werner Steinhaeusser for all his support. We thank Ikaria for provision of gases for DLNO measures. We also thank Jacqueline Sharp for study coordination.
Grants
This work was supported by grant HL60917 and the Cleveland Clinic Research Programs Council.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
SF conducted the study, performed research, analyzed and interpreted data and wrote the manuscript, DL performed research, DG conducted the study and recruited subjects, MMP conducted research and recruited subjects, WHWT analyzed data and reviewed manuscript, RAD reviewed manuscript, SCE designed research, analyzed data and wrote the manuscript. All authors participated in the study and have seen and approved the final version.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Farha, S., Laskowski, D., George, D. et al. Loss of alveolar membrane diffusing capacity and pulmonary capillary blood volume in pulmonary arterial hypertension. Respir Res 14, 6 (2013). https://doi.org/10.1186/1465-9921-14-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1465-9921-14-6