
Abstract
In this manuscript, we discuss the expectations versus the real-world results of four repurposed COVID-19 drugs: tocilizumab, remdesivir, favipiravir, and dexamethasone from a clinical and pharmacovigilant point of view. We suggest that though the results of two-phase III double-blind clinical trials have been less than expected, tocilizumab has a real remaining potential to treat selected critical cases of COVID-19 beyond clinical trials until more data are revealed. On the contrary, remdesivir, though its FDA approval, and favipiravir are least likely to benefit COVID-19 patients. Moreover, we recommend that the RECOVERY dexamethasone should only be considered for critical hospitalized COVID-19 patients and we urge physicians in developing countries to avoid using it in mild-moderate COVID-19 cases. Finally, we recommend considering a personalized risk-benefit ratio before a decision is made using any of these drugs.
Similar content being viewed by others

Introduction
Drug repurposing is considered as a rapid strategy for COVID-19 drug discovery [1] and many drugs are been tried and we would like to discuss the outcomes of four of them from a clinical and pharmacovigilant point of view.
Tocilizumab
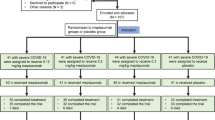
Tocilizumab, a recombinant humanized anti-IL-6 receptor monoclonal antibody which is FDA approved to manage diseases other than COVID-19, was initially shown to shorten the median time to COVID-19 clinical improvement [2] and it also showed non-statistically significant lower mortality results in patients with severe to critical COVID-19 [3]. Interestingly, although several studies have shown tocilizumab to significantly improve the clinical outcomes in severe cases of COVID-19 pneumonia [4,5,6,7,8,9], two-phase III double-blind, placebo-controlled clinical trials have demonstrated that tocilizumab did not improve the clinical status in patients with COVID-19-associated pneumonia and did not prevent intubation or death in moderately ill hospitalized patients with COVID-19, though potential benefit/harm could not be entirely excluded [10, 11]. Importantly, selection criteria of patients included in tocilizumab clinical trials were suggested to be revised [9, 12], and another phase III double-blind, placebo-controlled clinical trial demonstrated that patients with COVID-19-associated pneumonia who received tocilizumab plus standard of care were 44% less likely to progress to mechanical ventilation or death compared to patients who received placebo plus standard of care [13]. However, a recent small open-label trial cautioned from potential safety concerns while using tocilizumab that has not proved superior to standard care [14] and we definitely agree with the clinical vigilant recommendation that prohibits the routine use of tocilizumab for COVID-19 but we, likewise, do not agree with the one that restricts its use for clinical trials only [15]. In our point of view, tocilizumab should be always considered for selected most critical cases of COVID-19 until further data unveils the remaining mysteries.
Remdesivir
In comparison, some preliminary results anticipated the success of remdesivir, a nucleotide analogue prodrug, to treat COVID-19 [16, 17]. However, other studies have suggested that remdesivir is unexpected to possess significant clinical benefits based on its released results and safety profile [18,19,20,21,22,23]. Alarmingly, the overall mortality which is the most important final health outcome of any clinical trial was not included as the primary endpoint of any of the available trials that promoted remdesivir [23]. Moreover, though even an open-label phase III trial showed no significant difference between a 10-day remdesivir course (median length of treatment, 6 days) and standard care while claiming a benefit for the 5-day course [24], yet remdesivir is continued to be marketed globally and priced at 3120 USD for the typical patient with private insurance in the USA. Moreover, a black market has developed in India (https://economictimes.indiatimes.com/industry/healthcare/biotech/pharmaceuticals/remdesivir-sold-at-high-prices-in-mumbai-black-market-some-doctors-suggest-cheaper-alternatives/articleshow/76861773.cms?utm_source=contentofinterest&utm_medium=text&utm_campaign=cppst) and perhaps other developing countries. Notably, the WHO Solidarity Trial Consortium has recently announced the results of randomized trials performed in 405 hospitals located in 30 countries where 2750 patients received remdesivir and it was shown to have little or no effect on hospitalized COVID-19 patients, as indicated by overall mortality, initiation of ventilation, and duration of hospital stay [25]. However, despite all criticism and warnings, the FDA has approved remdesivir to be used for COVID-19 (https://www.fda.gov/news-events/press-announcements/fda-approves-first-treatment-covid-19) after an unprecedented consultation of a diverse group of experts outside the FDA [26]. Fortunately and we totally agree, the WHO has subsequently recommended against its use in COVID-19 regardless of disease severity [27]. Unfortunately, many countries all over the world continue to use it, including the author’s.
Favipiravir
Similarly, favipiravir (T-705), a nucleoside analogue, acts as a mutagen with a distinct bias to induce transitions in influenza virus RNAs by incorporating into both positive and negative stranded RNAs inducing lethal mutagenesis of influenza virus which might be a reason for the difficulty in isolating favipiravir-resistant influenza viruses in laboratories or to evolve resistance against clinically [28, 29]. Favipiravir was approved in Japan in 2014 as a treatment for novel or re-emerging influenza viruses, yet its local approval was heavily restricted as its clinical use needed governmental authorization, which was only permitted for potentially lethal diseases and a similar cautious attitude was also adopted in China [29]. Moreover, a highly complex pharmacokinetic profile together with lack of correlation between favipiravir drug concentrations and viral decline confirmed that the current clinical trials do not use an optimized dose or duration of therapy particularly in patients with severe illness [30]. Importantly, the Japanese Drug Safety Bureau, possibly due to limited safety data, recommended favipiravir to be avoided where alternative drugs could be used and adverse effects such as hyperuricemia and teratogenicity/embryotoxicity were reported from favipiravir in human and four different animal species studies, respectively, and a QTc prolongation potential was recommended to be further investigated [29, 31]. Additionally, hepatitis was also reported in 4 out of 63 COVID-19 patients who received favipiravir [32]. Notably, >85% of favipiravir completed clinical trials in registries or in published papers are unavailable which led to failure of conducting meta-analysis to generate conclusive evidence to support recommendation of favipiravir use in COVID-19 or know about its safety and efficacy profile [33], and a Japanese study showed no significant efficacy of favipiravir in SARS-CoV-2 elimination and might has also revealed a cautious attitude of a Japanese health authority, Fujita Health University, which conducted the study as out of 47 facilities across Japan that took part; only 88 patients were enrolled and completed the study (https://english.kyodonews.net/news/2020/07/af1418fc25ba-breaking-news-avigan-clinical-study-shows-no-effectiveness-in-treating-covid-19.html). Unfortunately, two manuscripts claiming favorable favipiravir trial results for COVID-19 came from China and were responsible to promote favipiravir, one published at the Journal of “Engineering” with the following timeline: received on 7 March 2020, revised on 11 March 2020, accepted on 12 March 2020; and the other is a heavily cited preprint (more than 330 citations) which has not been peer-reviewed yet and no updated version was posted since its first publishing on the 15 of April 2020. We opted not to cite either but we, instead, cite one article that used them to justify another small clinical trial performed in some Indian states, as elsewhere, using favipiravir to manage mild to moderate COVID-19, and though the results of this trial were anticipated by those authors on October 2020, no data are currently available and the link provided to refer to it was not functioning when accessed on the 5 of February 2021 [34]. Unfortunately, favipiravir has been included in the official protocols managing COVID-19 in several countries [34] including Egypt where it is described to manage selected mild COVID-19 cases according to the Egyptian MOH manual version 1.4 published on November 2020. We are strongly recommending against the continued use of favipiravir for management of COVID-19 as from our point of view, the risks are too high and the potential benefit, if present, is minimal or below compared to those risks.
Dexamethasone
On the other side, the randomized open-label evaluation of COVID-19 therapy (RECOVERY) collaborative group showed a small mortality benefit to dexamethasone therapy among patients who were receiving invasive mechanical ventilation: 482/2104 patients (22.9%) in the dexamethasone group and 1110/4321 patients (25.7%) in the usual care group [35], yet several concerns regarding the study design and the data and its interpretation were raised [36, 37]. Moreover, the RECOVERY results showing a potential benefit of dexamethasone in SRAS CoV-2 complicated patients contradicted the conclusive outcomes of several previous studies showing evidence of a possibly harmful effect when corticosteroids were used to manage SARS, MERS, and influenza pneumonia patients [38,39,40]. On the same day, the results of the RECOVERY study were published (July 17, 2020); we have submitted a letter to the New England Journal of Medicine (NEJM, ID 20-25534) representing some concerns about this study. Four emails were sent to NEJM, once every month, wondering about the unprecedented delay in publishing a short letter and the response was that the editor has been contacted on multiple occasions but he/she is busy because of the large number of COVID-19-related submissions and eventually, it was withdrawn on the next day we have requested it to be withdrawn (November 30, 2020). Our concerns included a wonder about the reason that the RECOVERY group chose 2:1 randomization though dexamethasone is a cheap drug and a 1:1 randomization maximizes the statistical power to detect the same difference [41, 42]. Furthermore, according to the RECOVERY preliminary report [35], the death ratio included in secondary outcomes was similar in both groups: 21.7% in the dexamethasone group and 22.7% in the usual care group, and we encouraged the authors to explain the potential reasons and to provide a more clarification to the included numbers; e.g., the number of living patients who have not been discharged from the hospital within 28 days does not match the subsequent subgroups. Furthermore, a second randomization of 4.5% of patients, complaining of hypoxia and inflammation, performed in the dexamethasone arm to compare the addition of tocilizumab on top of dexamethasone, has not been excluded in interpretation of the small mortality benefit assumed to be attributed only to dexamethasone. Unfortunately, we have encountered many Egyptian physicians who have not read the RECOVERY results or the clinical guidelines to use dexamethasone in severe-critical hospitalized COVID-19 patients and prescribed it to mild-moderate COVID-19 private patients leading sometimes to catastrophic complications and we suggest that this medical malpractice might have also been encountered in other developing countries.
Importantly, we would like to restress our previous agreement with the clinical recommendation against the routine use of glucocorticoids in the management of COVID-19 especially after important concerns were raised regarding the interpretation of data as well as the limitations of several studies showing potential benefit of glucocorticoids in COVID-19 [43]. Furthermore, patient characteristics were suggested to be assessed before prescribing corticosteroids to critical COVID-19 cases and a higher dose of corticosteroids administered to those patients was suggested to be more beneficial [44]. Thus, we recommend that for the patients’ best interests, a potential benefit from the RECOVERY dexamethasone as well as to assess its optimal dose and duration of administration in selected COVID-19 critical cases should be confirmed, or denied, by other well-designed and interpreted large randomized and controlled clinical trials [45,46,47].
Conclusion
In conclusion, we would like to join the WHO in its recommendation against the use of remdesivir for COVID-19. Furthermore, a teratogenic, embryotoxic favipiravir should undergo extensive studies to assess its potential gene mutation and/or chromosomal damage effects as well as to evaluate its long-term potential human carcinogenicity before allowing wide-scale global trialing and we suggest it is also least likely to safely manage COVID-19. On the other hand, we would like to recommend considering tocilizumab and dexamethasone for selected severe-critical cases of COVID-19 until the results of other much-needed large clinical trials fill some important missing gaps as regards to their COVID-19 efficacy/inefficacy.
Data Availability
N/A
References
Singh TU, Parida S, Lingaraju MC, Kesavan M, Kumar D, Singh RK. Drug repurposing approach to fight COVID-19. Pharmacol Rep. 2020;72:1479–508.
Kewan T, Covut F, Al-Jaghbeer MJ, Rose L, Gopalakrishna KV, Akbik B. Tocilizumab for treatment of patients with severe COVID-19: a retrospective cohort study. EClinicalMedicine. 2020;24:100418.
Rojas-Marte G, Khalid M, Mukhtar O, Hashmi AT, Waheed MA, Ehrlich S, et al. Outcomes in patients with severe COVID-19 disease treated with tocilizumab: a case-controlled study. QJM. 2020;113(8):546–50.
Toniati P, Piva S, Cattalini M, Garrafa E, Regola F, Castelli F, et al. Tocilizumab for the treatment of severe COVID-19 pneumonia with hyperinflammatory syndrome and acute respiratory failure: a single center study of 100 patients in Brescia, Italy. Autoimmun Rev. 2020;19(7):102568.
Alattar R, Ibrahim TBH, Shaar SH, Abdalla S, Shukri K, Daghfal JN, et al. Tocilizumab for the treatment of severe coronavirus disease 2019. J Med Virol. 2020. https://doi.org/10.1002/jmv.25964.
Klopfenstein T, Zayet S, Lohse A, Selles P, Zahra H, Kadiane-Oussou NJ, et al. Impact of tocilizumab on mortality and/or invasive mechanical ventilation requirement in a cohort of 206 COVID-19 patients. Int J Infect Dis. 2020;99:491–5.
Samaee H, Mohsenzadegan M, Ala S, Maroufi SS, Moradimajd P. Tocilizumab for treatment patients with COVID-19: Recommended medication for novel disease. Int Immunopharmacol. 2020;89:107018.
Keske Ş, Tekin S, Sait B, İrkören P, Kapmaz M, Çimen C, et al. Appropriate use of tocilizumab in COVID-19 infection. Int J Infect Dis. 2020;99:338–43.
Wise J. Covid-19: arthritis drugs improve survival in intensive care patients, shows study. BMJ. 2021;372:n61.
Roche. Roche provides an update on the phase III COVACTA trial of Actemra/RoActemra in hospitalised patients with severe COVID-19 associated pneumonia, https://www.roche.com/investors/updates/inv-update-2020-07-29.htm; 2020, July 29.
Stone JH, Frigault MJ, Serling-Boyd NJ, Fernandes AD, Harvey L, Foulkes AS, et al. Efficacy of tocilizumab in patients hospitalized with Covid-19. N Engl J Med. 2020;383:2333–44.
Hojyo S, Uchida M, Tanaka K, Hasebe R, Tanaka Y, Murakami M, et al. How COVID-19 induces cytokine storm with high mortality. Inflamm Regener. 2020;40(1):37.
Roche. Roche’s phase III EMPACTA study showed Actemra/RoActemra reduced the likelihood of needing mechanical ventilation in hospitalised patients with COVID-19 associated pneumonia, https://www.roche.com/media/releases/med-cor-2020-09-18.htm; 2020, September 18.
Veiga VC, Prats JAGG, Farias DLC, Rosa RG, Dourado LK, Zampieri FG, et al. Effect of tocilizumab on clinical outcomes at 15 days in patients with severe or critical coronavirus disease 2019: randomised controlled trial. BMJ. 2021;372:n84.
Parr JB. Time to reassess tocilizumab’s role in COVID-19 pneumonia. JAMA Intern Med. 2021;181(1):12–5.
Ko W-C, Rolain J-M, Lee N-Y, Chen P-L, Huang C-T, Lee P-I, et al. Arguments in favour of remdesivir for treating SARS-CoV-2 infections. Int J Antimicrob Agents. 2020;55(4):105933.
Lamb YN. Remdesivir: first approval. Drugs. 2020;80(13):1355–63.
Marcolino VA, Pimentel TC, Barão CE. What to expect from different drugs used in the treatment of COVID-19: a study on applications and in vivo and in vitro results. Eur J Pharmacol. 2020;887:173467.
Kelleni M. Rapid response: remdesivir is least likely to be effective for safe treatment of COVID-19: a pharmacovigilant point of view. BMJ. 2020;369:m2097rr.
Kelleni MT. Remdesivir-gate for COVID-19. Acta Sci Gastrointest Disord. 2020;3(8):01.
Carothers C, Birrer K, Vo M. Acetylcysteine for the treatment of suspected remdesivir-associated acute liver failure in COVID-19: a case series. Pharmacotherapy. 2020.
Remdesivir-related acute kidney injury in patients with COVID-19. React Wkly. 2020;1826(1):5.
Piscoya A, Ng-Sueng LF, Parra del Riego A, Cerna-Viacava R, Pasupuleti V, Roman YM, et al. Efficacy and harms of remdesivir for the treatment of COVID-19: a systematic review and meta-analysis. PLoS ONE. 2020;15(12):e0243705.
Spinner CD, Gottlieb RL, Criner GJ, Arribas López JR, Cattelan AM, Soriano Viladomiu A, et al. Effect of remdesivir vs standard care on clinical status at 11 days in patients with moderate COVID-19: a randomized clinical trial. JAMA. 2020;324(11):1048–57.
Pan H, Peto R, Abdool Karim Q, Alejandria M, Henao Restrepo AM, Hernandez Garcia C, et al. Repurposed antiviral drugs for COVID-19; interim WHO SOLIDARITY trial results. medRxiv. 2020:2020.10.15.20209817.
Jon Cohen KK. The ‘very, very bad look’ of remdesivir, the first FDA-approved COVID-19 drug. Science. 2020.
WHO. WHO recommends against the use of remdesivir in COVID-19 patients. 2020.
Goldhill DH, Langat P, Xie H, Galiano M, Miah S, Kellam P, et al. Determining the mutation bias of favipiravir in influenza virus using next-generation sequencing. J Virol. 2019;93(2):e01217–8.
Shiraki K, Daikoku T. Favipiravir, an anti-influenza drug against life-threatening RNA virus infections. Pharmacol Ther. 2020;209:107512.
Ison MG, Scheetz MH. Understanding the pharmacokinetics of favipiravir: implications for treatment of influenza and COVID-19. EBioMedicine. 2021;63:103204.
Pilkington V, Pepperrell T, Hill A. A review of the safety of favipiravir - a potential treatment in the COVID-19 pandemic? J Virus Erad. 2020;6(2):45–51.
Rattanaumpawan P, Jirajariyavej S, Lerdlamyong K, Palavutitotai N, Saiyarin J. Real-world experience with favipiravir for treatment of COVID-19 in Thailand: results from a multi-center observational study. medRxiv. 2020:2020.06.24.20133249.
Khambholja K, Asudani D. Potential repurposing of favipiravir in COVID-19 outbreak based on current evidence. Travel Med Infect Dis. 2020;35:101710.
Joshi S, Parkar J, Ansari A, Vora A, Talwar D, Tiwaskar M, et al. Role of favipiravir in the treatment of COVID-19. Int J Infect Dis. 2021;102:501–8.
Dexamethasone in hospitalized patients with Covid-19 — Preliminary Report. N Engl J Med. 2020.
Waterer GW, Rello J. Steroids and COVID-19: we need a precision approach, not one size fits All. Infect Dis Ther. 2020;9(4):701–5.
Lanthier L, Mayette M, Huard G, Plourde ME, Cauchon M. In patients hospitalized for COVID-19, does dexamethasone reduce 28-days mortality compared to standard treatment? Rev Med Interne. 2020;41(11):790–1.
Russell CD, Millar JE, Baillie JK. Clinical evidence does not support corticosteroid treatment for 2019-nCoV lung injury. Lancet. 2020;395(10223):473–5.
Arabi YM, Mandourah Y, Al-Hameed F, Sindi AA, Almekhlafi GA, Hussein MA, et al. Corticosteroid therapy for critically ill patients with Middle East respiratory syndrome. Am J Respir Crit Care Med. 2017;197(6):757–67.
Ni Y-N, Chen G, Sun J, Liang B-M, Liang Z-A. The effect of corticosteroids on mortality of patients with influenza pneumonia: a systematic review and meta-analysis. Crit Care. 2019;23(1):99.
Torgerson D, Campbell M. Unequal randomisation can improve the economic efficiency of clinical trials. J Health Serv Res Policy. 1997;2(2):81–5.
Hey SP, Kimmelman J. The questionable use of unequal allocation in confirmatory trials. Neurology. 2014;82(1):77–9.
Kelleni MT. Early use of non-steroidal anti-inflammatory drugs in COVID-19 might reverse pathogenesis, prevent complications and improve clinical outcomes. Biomed Pharmacother. 2021;133:110982.
Monedero P, Gea A, Castro P, Candela-Toha AM, Hernández-Sanz ML, Arruti E, et al. Early corticosteroids are associated with lower mortality in critically ill patients with COVID-19: a cohort study. Crit Care. 2021;25(1):2.
Shang L, Zhao J, Hu Y, Du R, Cao B. On the use of corticosteroids for 2019-nCoV pneumonia. Lancet. 2020;395(10225):683–4.
Singh AK, Majumdar S, Singh R, Misra A. Role of corticosteroid in the management of COVID-19: a systemic review and a Clinician’s perspective. Diabetes Metab Syndr. 2020;14(5):971–8.
Ahmed MH, Hassan A. Dexamethasone for the treatment of coronavirus disease (COVID-19): a review. SN Compr Clin Med. 2020:1–10.
Acknowledgments
The author would like to thank two anonymous peer reviewers who have provided very precious comments that heavily enriched this manuscript and without their approval, this manuscript would have never seen the light. I am also very thankful for the highly professional and scientific attitude that I have experienced dealing with SN Comprehensive Clinical Medicine and its editorial board especially its managing editor, Dr. Peter Butler.
Code Availability
N/A
Author information
Authors and Affiliations
Contributions
Sole author.
Corresponding author
Ethics declarations
Ethics approval
N/A
Consent to participate
N/A
Consent for publication
N/A
Competing Interests
The author declares no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on COVID-19
Rights and permissions
About this article

Cite this article
Kelleni, M.T. Tocilizumab, Remdesivir, Favipiravir, and Dexamethasone Repurposed for COVID-19: a Comprehensive Clinical and Pharmacovigilant Reassessment. SN Compr. Clin. Med. 3, 919–923 (2021). https://doi.org/10.1007/s42399-021-00824-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s42399-021-00824-4