
Abstract
Headache occurs in only about 13% of patients within the cohort of presenting COVID-19 symptoms. The hypothesis that such a painful symptomatic picture could be considered a prognostic factor for COVID-19 positive evolution or its trend of severity, or the co-generation of hyposmia/anosmia and/or hypogeusia/ageusia, needs robust epidemiological data, punctual pathophysiological demonstrations, and a detailed comparative analysis on drug–drug interactions (DDIs).
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Viewpoint
To date, scientific literature is regrettably and exceedingly generous towards the term “COVID-19”: 71,664 scientific articles published [1], 49,578,590 confirmed cases, and 1,245,717 confirmed deaths for COVID-19 in less than 1 year [2].
As the number of new registered cases continues to rise on a daily basis, 441,696 on the 9th of November 2020, so too is there an increase in questions for the scientific community while certainties struggle to emanate from this immensity of scientific data. It is clear that all systems have been crushed by this cytokine release syndrome (CRS) and that the list of epidemiological and clinical characteristics, including headache, does not appear to be subject to further updates. Headache as a symptom of COVID-19 is present in only 12.9% of patients afferent to COVID-19 emergency medicine [3].
Headache, for those experiencing the COVID-19 clinic at first hand, does not seem to be of such clinical relevance, but only an epiphenomenon secondary to the involvement of complex systems, the cardiovascular/coagulative and respiratory/neurological, other than to a febrile state.
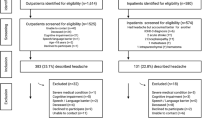
The assumption that the international scientific community should use headache as prognostic factor of COVID-19 duration or severity in a COVID-19 emergency medicine clinical setting is a recent concept. Such assumption is expressed in two recent articles, Caronna and Magdy [4, 5]. The first study has been carried out on 130 COVID-19 patients (74.6% with headache), while the latter on 172 COVID-19 patients with headache selected from a cohort total of 238 COVID-19 patients (52.9%) is the highest percentile reported in the majority of the scientific literature [1]. Interestingly, these data came from the use of face-to-face interviews in patients strongly compromised and in a clinical setting strictly sealed and in operational emergency.
The methodology of the two reports is not the dominant concept now, but we wish to highlight how every subtended COVID-19 disease is scotomized, like radiological and blood coagulation data, parameters on pulmonary, renal, cerebral functionality [6, 7] without stating clear correlations, apart from generic considerations on pathophysiological hypothesis with the clinical manifestations of headache [4, 5].
We must not overlook the fact that in order to curb this unbridled pathology, we are struggling with therapeutic approaches centering on this CRS, applying a variety of drugs with uncertain impact on the multifarious COVID-19 disease and with little known action on headache symptomatology as protease inhibitors, heparin, macrolide antibiotics, hydroxychloroquine, and monoclonal antibodies for CAR T cells [8]. It is not yet known to what extent they could interfere, increase, suppress, or cause alone or through a drug–drug interaction (DDI) any clinical symptom related to headache [8]. We should also be very cautious when conjugating headache with hyposmia/anosmia and/or hypogeusia/ageusia present in COVID-19 patients [9] following a generic concept of proximity [10].
A rigorous big data analysis would help obtain more transparent numbers that headache experts might then translate into verified, steady, and consolidated prognostic indications useful for a clearly different medical scientific community operating in and studying COVID-19 emergency medicine.
Data Availability
Not applicable.
References
https://pubmed.ncbi.nlm.nih.gov/?term=COVID-19&sort=date (last accessed 9 November 2020).
https://covid19.who.int (last accessed 9 November 2020).
Kaur N, Gupta I, Singh H, Karia R, Ashraf A, Habib A, et al. Epidemiological and clinical characteristics of 6635 COVID-19 patients: a pooled analysis. SN Compr Clin Med. 2020;2:1048–52. https://doi.org/10.1007/s42399-020-00393-y.
Caronna E, Ballvé A, Llauradó A, Gallardo VJ, Ariton DM, Lallana S, et al. Headache: a striking prodromal and persistent symptom, predictive of COVID-19 clinical evolution. Cephalalgia. 2020;40(13):1410–21. https://doi.org/10.1177/0333102420965157.
Magdy R, Hussein M, Ragaie C, Abdel-Hamid HM, Khallaf A, Rizk HI, et al. Characteristics of headache attributed to COVID-19 infection and predictors of its frequency and intensity: a cross sectional study. Cephalalgia. 2020 Nov;40(13):1422–31. https://doi.org/10.1177/0333102420965140.
Arcari L, Luciani M, Cacciotti L, Musumeci MB, Spuntarelli V, Pistella E, et al. Incidence and determinants of high-sensitivity troponin and natriuretic peptides elevation at admission in hospitalized COVID-19 pneumonia patients. Intern Emerg Med. 2020;15(8):1467–76. https://doi.org/10.1007/s11739-020-02498-7.
Spuntarelli V, Luciani M, Bentivegna E, Marini V, Falangone F, Conforti G, et al. COVID-19: is it just a lung disease? A case-based review. SN Compr Clin Med. 2020;2:1401–6. https://doi.org/10.1007/s42399-020-00418-6.
Pennica A, Conforti G, Falangone F, Martocchia A, Tafaro L, Sentimentale A, et al. Clinical management of adult coronavirus infection disease 2019 (COVID-19) positive in the setting of low and medium intensity of care: a short practical review. SN Compr Clin Med. 2020;2:694–9. https://doi.org/10.1007/s42399-020-00333-w.
Schönegger CM, Gietl S, Heinzle B, Freudenschuss K, Walder G. Smell and taste disorders in COVID-19 patients: objective testing and magnetic resonance imaging in five cases. SN Compr Clin Med. 2020. https://doi.org/10.1007/s42399-020-00606-4.
Rocha-Filho PAS, Magalhães JE. Headache associated with COVID-19: frequency, characteristics and association with anosmia and ageusia. Cephalalgia. 2020 Nov;40(13):1443–51. https://doi.org/10.1177/0333102420966770.
Code Availability
Not applicable.
Funding
Open access funding provided by Università degli Studi di Roma La Sapienza within the CRUI-CARE Agreement.
Author information
Authors and Affiliations
Contributions
All authors substantially contributed to the conception, design, and drafting of the article and approved the final version to be published.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethics Approval
Not applicable.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on COVID-19
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Martelletti, P., Bentivegna, E., Luciani, M. et al. Headache as a Prognostic Factor for COVID-19. Time to Re-evaluate. SN Compr. Clin. Med. 2, 2509–2510 (2020). https://doi.org/10.1007/s42399-020-00657-7
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s42399-020-00657-7