
Abstract
Sleep is an integral and constitutive part of life, invariably observed in animals with even a simple nervous system. Importantly, sleep is an active and highly regulated state. Sleep propensity or sleep need and its best established biological marker, electroencephalographic (EEG) slow-wave (or delta) activity, is tightly associated to prior wakefulness and sleep and is homeostatically regulated. Sleep need may be considered an essential aspect of life, just like feeding, drinking, and procreation. Sleep, therefore, likely developed in a primordial state of evolution and should either aid or, at least, not interfere with other essential biological aspects of life such as metabolisms and reproduction. Consistent with this view, brain circuitries regulating sleep need, metabolism, and reward appear to involve the basal ganglia and are tightly linked. They may sense changes in the organism’s major cellular energy store, adenosine-tri-phosphate (ATP), and its derivative adenosine, and act in concert with other important neuromodulatory systems including dopamine, glutamate, and hypocretin.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Twenty years ago, in 1995, Benington and Heller [1] proposed that the function of sleep is to replenish brain energy stores and that extracellular adenosine levels provide the brain signal for measuring sleep need. This seminal and scholarly theory provided and inspired a number of testable hypotheses, some of which are still investigated today. The currently available results suggest that the roles for sleep in regulating energy metabolism are probably more complex than originally proposed [2, 3]. Nevertheless, it is now well established that adenosine and adenosine receptors play important roles in regulating wakefulness and sleep (see [4, 5] for recent reviews). This evidence, as well as some ideas on the intricate possible links among sleep homeostasis, metabolism, and adenosine, will be discussed in this overview.
Wakefulness and Sleep are Regulated by Circadian and Homeostatic Influences
The cyclic alternation between wakefulness and sleep forms a fundamental biological rhythm during the 24-h light-dark cycle. These two distinct states result from the interplay between circadian and homeostatic oscillators, a concept originally described by the two-process model of sleep–wake regulation [6]. The circadian process reflects an endogenous, 24-h variation in the propensity for wakefulness and sleep [6] and is controlled by the suprachiasmatic nuclei (SCN) of the anterior hypothalamus. The SCN is considered the circadian master clock in mammals. In humans, the SCN may promote wakefulness in the early evening, to prevent people from falling asleep during the time when homeostatic sleep pressure reaches its highest level after a waking day. The homeostatic process represents an hourglass mechanism, which gradually builds up with increasing time awake, and roughly exponentially declines during sleep. Thus, in healthy humans, circadian and homeostatic systems work in opposition to ensure consolidated periods of wakefulness and sleep [7]. The interaction of the two processes also allows for consolidated sleep during the biological night. The SCN may promote a circadian increase in sleep tendency, which counteracts the decrease in homeostatic sleep propensity as the individual accumulates sleep [8, 9].
Multiple adenosine receptor subtypes appear to contribute to the control of clock functions and circadian timing. This evidence was recently summarized elsewhere [10]. Here, we will focus on the potential roles for adenosine and adenosine receptors in regulating the homeostatic facet of sleep and metabolism.
Adenosine and Adenosine Receptors
Adenosine Formation, Metabolism, and Clearance
Adenosine is usually regarded as a neuromodulator rather than a neurotransmitter because of the way it operates and is released in the nervous system. The formation of adenosine in the brain changes in an activity-dependent manner and is linked to the intracellular depletion of the energy-rich molecule adenosine-tri-phosphate (ATP) [11, 12]. Triggered by energy consumption, ATP is dephosphorylated to adenosine-di-phosphate, adenosine-mono-phosphate (AMP), and adenosine. Extracellular adenosine binds to one of four specific G-protein-coupled adenosine receptors. Caffeine, the world’s most readily consumed psychostimulant compound, promotes wakefulness and inhibits sleep by antagonizing distinct adenosine receptors [13].
Changes in activity-dependent levels of extracellular adenosine depend on several factors [14]. When intracellular adenosine concentrations are high, adenosine can be released directly from neurons via equilibrative nucleoside transporters (ENTs) [15]. The main metabolic pathways of adenosine are the phosphorylation to AMP by adenosine kinase (ADK) and the irreversible degradation to inosine by adenosine deaminase (ADA). Adenosine can also be produced directly in the extracellular space through hydrolysis and dephosphorylation of ATP by ecto-nucleotidases [12, 16]. The ATP is released from γ-amino-butyric acid (GABA)ergic, cholinergic, monoaminergic, and glutamatergic neurons as a consequence of cellular activity [17, 18]. It may be noteworthy that, in rodents, the final step to release adenosine by dephosphorylation of AMP, occurs primarily in the striatum and olfactory bulb [19]. Especially the striatum, a main structure of the basal ganglia (BG), has recently been proposed to play important roles in sleep–wake regulation [20, 21]. Furthermore, ATP and adenosine can be released by a recently established process called gliotransmission. Molecular genetic manipulations in mice revealed that glial cells provide a significant source of extracellular adenosine in the brain [22, 23•], which is crucial for sleep and distinct sleep-dependent brain functions [24–26].
The neuromodulatory actions of adenosine are mainly terminated by neuronal and astrocytic (re)-uptake by the so-called non-concentrative nucleoside transporters [27]. On the other hand, ADA, which is mainly expressed on the extracellular membrane and on cell surface-bound adenosine receptors, is believed to importantly modulate receptor affinity for adenosine [28]. This enzyme may be of particular importance for adenosine clearance when elevated levels of the nucleoside have to be cleared, for example after prolonged wakefulness.
Adenosine Receptors
Four different subtypes of G-protein-coupled adenosine receptors mediate the cellular effects of adenosine: A1, A2A, A2B, and A3 receptors. Activation of A1 and A3 receptors inhibits adenylate cyclase (AC) via Gi-proteins, whereas A2A and A2B receptors are coupled to Gs proteins that increase AC activity [29]. The divergent second messenger pathways of A1 and A3 compared to A2A/B receptors, as well as their different expression patterns and affinities for endogenous adenosine, are important topics of current adenosine research (see [30] for an extensive recent review). The characteristics of the currently known adenosine receptor subtypes will be briefly summarized in the following paragraphs.
The A1 receptors are expressed throughout the body and located widely on excitatory neurons in the brain where they are found on pre- and postsynaptic membranes. In vivo positron emission tomography (PET) with selective radioligands revealed highest A1 receptor occupancy in striatum and thalamus, as well as in temporo-parietal and occipital cortices [31]. The affinity of A1 receptors for adenosine is high (nanomolar range), and their activation can promote delta activity in nonrapid eye movement (NREM) sleep [32], inhibit lipolysis [33], reduce heart rate [34], and decrease renal blood flow [35]. A recent PET brain imaging study in humans suggested that four to five cups of coffee (corresponding to ~450 mg caffeine) in a 70-kg volunteer can displace endogenous adenosine from 50 % of cerebral A1 receptors [36•].
The A2A receptors have a similarly high affinity for adenosine, yet are expressed in high abundance primarily on post-synaptic membranes in the dorsal striatum [37]. A recent study mapped the projections of A2A-receptor-expressing neurons of the nucleus accumbens (NAc) within the dorsal striatum [38•]. It revealed specific projections to ventral pallidum (VP), lateral hypothalamus, lateral preoptic area, raphe nucleus, ventral tegmental area (VTA), and other parts of the brainstem. Local activation of A2A receptors in the NAc is suggested to promote sleep [39•] and has also been linked to reward, feeding, and other goal-oriented behaviors [40]. Importantly, caffeine not only blocks A1 receptors but also competitively antagonizes A2A receptors in a nonselective manner [13]. Studies in genetically modified mice suggests that A2A, but not A1, receptors mediate the wake-promoting effect of the stimulant [41]. In the periphery, A2A receptors are found in the spleen and leukocytes, and to a lesser extent in heart, lung, and blood vessels. Their activation results in vasodilation and hypotension [42] and has also been associated with immunosuppression and inflammation [43, 44].
The A2B receptors are widely expressed in brain and periphery, yet their abundance is low. Furthermore, the A2B receptor has low affinity for adenosine (micromolar range). Endogenous activation of these receptors may only be observed in pathological conditions where adenosine levels are elevated, such as during hypoxia [45, 46] or ischemia [47, 48]. Nevertheless, the A2B receptor may play a role for metabolic effects and modulate glucose homeostasis, blood lipid levels, and atherosclerosis [49, 50].
Knowledge about the A3 receptor is scarce, and its role varies among different species. Generally, A3 receptors are only expressed at low levels, show low affinity for adenosine [14] and have been suggested to play a more prominent role during development than later in life [51].
Sleep Homeostasis and Adenosine
Electrical brain activity as measured with the EEG provides distinct neurophysiological fingerprints of wakefulness, NREM sleep, and REM sleep. In deep slow wave sleep, high-amplitude slow waves (or delta waves) with a frequency of 0.5-2 Hz are most prevalent. The duration of slow wave sleep and the preponderance of EEG delta oscillations in NREM sleep (and also to some extent in REM sleep) reliably reflect the duration of prior wakefulness and provide the best established biomarker of sleep need and sleep homeostasis. Many studies in animals and humans demonstrated that EEG power density in the delta range, particularly in NREM sleep, is enhanced after prolonged wakefulness. The reversed pattern can be observed after a daytime nap or during the decline of “sleep intensity” in the course of a sleep episode [52]. Converging evidence accumulated over the last two decades indicates that adenosine and adenosine receptors contribute to the regulation of sleep intensity and, possibly, to sleep need and sleep homeostasis.
Does Adenosine Regulate Sleep Intensity and Sleep Homeostasis?
In animal models, extracellular adenosine levels in the brain, are often higher during the active phase (dominated by wakefulness) than during the rest phase (dominated by sleep) [53–55]. Adenosine fulfills major criteria of an endogenous sleep regulatory substance [56]. Briefly, intra-cerebroventricular infusion of adenosine promotes sleep in rats [57] and adenosine levels in hippocampus, cortex, and basal forebrain (BF) are increased after sleep deprivation and normalized after recovery sleep [58, 59]. In slices prepared from the rodent BF, these sleep–wake dependent changes were recently confirmed in vitro [60]. Furthermore, excitatory glutamatergic inputs from the hypothalamus, amygdala, and hippocampus to GABAergic and cholinergic neurons of the BF contribute to local adenosine production [60, 61]. These findings may further support the idea that the BF acts as an adenosine sensor to determine sleepiness or sleep need following wakefulness. Nevertheless, lesion and pharmacological studies revealed that accumulation of adenosine in the BF is not necessary for sleep induction, nor are BF cholinergic neurons essential for sleep drive [62]. These data challenge a causal role for adenosine in the BF as the regulator of sleep homeostasis. Furthermore, ATP and adenosine in the extracellular space are rapidly metabolized and removed and are, therefore, unlikely to be involved in long-term sleep–wake regulation [18]. The available evidence rather suggests that extracellular adenosine provides a global feedback signal on neuronal networks, including subcortical and cortical structures [23•, 63] and contributes to wake–sleep transitions and the regulation of important functional aspects of sleep such as sleep intensity.
Consistent with this view, genetic studies in mice and humans suggest that the adenosine metabolizing pathway contributes to the generation of EEG delta oscillations reflecting sleep intensity (Table 1). Transgenic mice with increased ADK activity (Adk-tg) show reduced EEG delta power and appear to have a reduced capacity to intensify sleep after sleep deprivation [64]. In addition, a functional polymorphism in the gene encoding ADA in humans, which causes a reduced breakdown of adenosine to inosine [77], has been consistently associated with prolonged slow wave sleep and enhanced EEG delta activity in NREM sleep [66, 67•, 68]. This observation first made in stringently controlled laboratory experiments was independently confirmed by a large, community-based epidemiological sample [69•]. By contrast, the homeostatic response to sleep deprivation was not reliably altered in Adk-tg mice and unaffected by ADA genotype in humans [64, 67•].
In conclusion, the current findings indicate that the adenosinergic tone at the synapse regulates sleep intensity. Nevertheless, it needs to be kept in mind that, in the available studies, information regarding adenosine levels in the brain is generally lacking [78]. The observed phenotypes could, therefore, reflect other changes in the adenosine metabolizing pathways and may not necessarily be due to altered adenosine levels.
Do Adenosine Receptors Regulate Sleep Intensity and Sleep Homeostasis?
One of the most common indications that adenosine signaling contributes to the control of sleep intensity comes from the powerful wake-promoting effects of caffeine, which also attenuates waking and sleep EEG markers of sleep homeostasis [75••, 79]. Nevertheless, while the effects of caffeine on sleep may be independent from adenosine receptors in Drosophila [70], the specific contributions of A1 and A2A receptors also remain controversial in mammals [21].
Adenosine A1 Receptors
It has long been thought that the adenosine A1 receptors, which are widely distributed in the central nervous system (CNS), are responsible for the sleep-promoting effects of adenosine [1]. Prolonged wakefulness appears to be associated with upregulated A1 receptor binding in subcortical and cortical brain structures in rats and humans [31, 80, 81]. Nevertheless, a careful study performed in A1 receptor knockout mice revealed that homeostatic sleep–wake regulation is unaltered in animals that constitutively lack A1 receptors [71]. More recently, a CNS-specific conditional knockout of this receptor was created. This genetic model showed reduced delta power in NREM sleep both in baseline and recovery sleep opportunities following sleep deprivation [72]. The authors concluded that elevated sleep need is, at least in part, signaled through A1 receptors. Nevertheless, as discussed in a recent overview [78], the sleep restriction protocol employed may have allowed the mice to recover from sleep loss and to reduce delta power between the sleep deprivation periods. Furthermore, a general reduction in delta power in wakefulness, NREM sleep, and REM sleep was reported, suggesting that this gene impacts general electrical activity of the brain rather than having a specific effect on sleep homeostasis.
A recent study investigated the presynaptic signaling cascade of A1 receptors and the effects of adenosine on CaV2.1 voltage-dependent calcium channels in a transgenic mouse line [82•]. These channels are predominantly localized on presynaptic nerve terminals where they play a key role in mediating neurotransmitter release. They are specifically susceptible to Gi-protein-coupled neurotransmitter inhibition, for instance by activation of A1 receptors. The findings of Deboer and co-workers suggest that inhibition of CaV2.1 channels by adenosine contributes to increased sleep propensity, sleep initiation, and the sensitivity of caffeine. The data highlight the possibility that the wake-promoting effects of adenosine not only depend on altered postsynaptic signaling but also on ionotropic presynaptic signal transduction [82•].
Adenosine A2A Receptors
Accumulating evidence indicates that A2A receptors also contribute to the effects of adenosine on sleep. Mice lacking functional A2A receptors show an absent sleep rebound after sleep deprivation [83], and A2A receptors in rats appear to be downregulated by sleep loss [81]. Furthermore, local administration of a selective A2A receptor agonist in the vicinity of the ventrolateral preoptic area and NAc of the hypothalamus [84], as well as in the pontine reticular formation [85], promotes NREM sleep. Recently, studies in conditional knockout mice revealed that A2A receptors in the shell region of the striatal NAc may play an essential role in the wakefulness-promoting effects of caffeine [39•].
Importantly, findings in humans also support a role for adenosine A2A receptors in sleep–wake regulation. More specifically, genetic variation of the A2A receptor (ADORA2A) gene was shown to modulate the sleep-deprivation-induced increase in EEG delta activity in NREM sleep, as well as subjective and objective effects of caffeine on the sleep EEG [74, 75••]. A role for the common 1976T>C polymorphism (rs5751876) of ADORA2A for caffeine-related sleep disturbances was recently confirmed in a large genome-wide-association study [86••].
In conclusion, although contradictory findings exist, the current evidence indicates that both A1 and A2A receptors contribute to the regulation of sleep intensity and sleep homeostasis (Table 1). The two adenosine receptor families may act in region-specific manner, and their effects may not be independent. Indeed, an interesting recent PET brain imaging study in humans shed new light on the possible functional consequences of genetic variants of ADORA2A. The study shows that the rs5751876 T-allele, which has been associated with caffeine insensitivity [74] and a stronger increase in EEG delta activity after sleep deprivation [74, 75••], corresponds to higher A1 receptor availability in the brain [87••]. These data suggest that the sleep-related effects of ADOARA2A polymorphism rs5751876 may not reflect A2A receptor function alone, but could also be linked to differential A1 receptor expression.
Purine Type-2 (P2X) Receptors
As mentioned above, extracellular adenosine is rapidly metabolized and removed. It has, therefore, been questioned whether adenosine alone can be responsible for long-term sleep–wake regulation [18]. Adenosine is released in response to neuronal activity and may modulate sleep–wake regulatory processes indirectly via ATP. The activity-dependent transient changes in extracellular ATP are slower and can be detected by membrane purine type-2 (P2X) receptors. For example, independently of adenosine, P2X7 receptors cause the release of other, activity-dependent sleep regulatory substances, such as brain-derived neurotrophic factor, which also modulate sleep intensity and sleep homeostasis [88].
Adenosine Receptor Heteromers and Receptor–Receptor Interactions
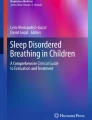
An important and currently intensively investigated aspect of adenosine signaling is the ability of adenosine receptors to form heteromers and receptor–receptor interactions. In striatal astrocytes, A1–A2A receptor heteromers are observed, and their activation may depend on the concentration of adenosine. At low adenosine concentrations, the activation of Gi-protein coupled A1 receptors in the A1–A2A oligomer will predominate, whereas at high adenosine concentrations, A1 receptors are inhibited, leading to the preferential activation of Gs-protein coupled A2A receptors [89, 90]. Furthermore, adenosine A1 and A2A receptors form functional heteromers with dopamine D1 and D2 receptors. In both cases, binding of adenosine results in reduced dopaminergic signaling. The A1–D1 receptor heteromers are preferentially expressed in the so-called direct pathway on striato-nigral neurons in the BG [91, 92]. By contrast, A2A–D2 heteromers are mainly expressed on striato-pallidal neurons originating in VTA and NAc, which are part of the so-called indirect pathway [21, 92]. The NAc has been suggested to play a crucial role in sleep–wake regulation, by integrating signals from cortex, thalamus, amygdala, and midbrain dopaminergic neurons [21, 93, 94]. The co-localization of adenosine and dopamine receptors may allow the NAc to integrate adenosinergic and dopaminergic interactions to promote sleep. The NAc is ideally located and inhibits via GABAergic interneurons four pathways of the brain’s arousal and activation system (Fig. 1). These pathways include the following: (1) VP, thalamus, and medial prefrontal cortex (mPFC), a pathway important for cognition and emotional processes, which are sensitive to sleep need; (2) lateral hypothalamus (LHA), tuberomammillary nucleus (TMN), and locus coeruleus (LC), an essential pathway for maintaining wakefulness; (3) parabrachial nucleus (PB) and BF, a pathway involved in maintaining wakefulness and cognitive performance; and (4) dopaminergic neurons of the VTA, which feeds back to the NAc, primarily via dopamine D2 receptors [21, 94]. According to this model proposed by Lazarus and colleagues, stimulation of the VTA promotes wakefulness by activating inhibitory dopamine D2 receptors of the NAc, which results in a disinhibition of the four activating pathways. By contrast, activation of excitatory A2A receptors of the NAc actively promotes sleep by inhibiting the four activating pathways.

Schematic representation of adenosine dependent basal ganglia projections involved in sleep wake regulation (dark purple) and metabolism (orange), and their modulation by adenosinergic, dopaminergic, and glutamatergic receptor heteromers. The model proposes that adenosine by activating excitatory (red circles) A2A receptors (or glutamate by activating metabotropic glutamate type 5 [mGlu5] receptors) in the nucleus accumbens (NAc), can inhibit brain pathways, essential for arousal and feeding behavior, via GABAergic neurotransmission. Oppositely, activation of inhibitory (blue circles) dopamine D2 receptors by dopaminergic projections from the ventral tegmental area (VTA) reduces NAc activity and thereby promotes wake and feeding behavior. Secondly, activation of inhibitory adenosine A1 receptors in the lateral hypothalamus (LHA) inhibits LHA activity and thereby promotes sleep and fasting. Activation of LHA excitatory dopamine D1 receptors, on the other hand, promotes LHA activity and thereby promotes arousal and metabolic pathways. Finally, insulin and leptin, which signals the availability of food, are able to promote feeding and inhibit sleep by directly binding to the NAc and VTA. Taken together, the dopaminergic and adenosinergic modulations of the NAc and LHA are ideally positioned within the basal ganglia to modulate sleep–wake regulation and metabolism. VP ventral pallidum, VLPO ventrolateral preoptic nucleus, TMN hypothalamic tuberomammillary nucleus, LC locus coeruleus, NTS nucleus tractus solitarius, BF basal forebrain, PB Parabrachial nucleus, PVN paraventricular nucleus, ARC arcuate nucleus, VMN ventro-medial nuclei, NAc nucleus accumbens, LHA lateral hypothalamus (hypocretin), VTA ventral tegmental area (dopamine)
In accordance with these hypotheses, dopamine levels in mPFC and NAc of freely moving rats were reported to be elevated in wakefulness and REM sleep, yet to be reduced in NREM sleep [95]. Elimination of dopamine D2 receptors in mice reduces wakefulness and enhances sleep [96], whereas either activation or blockage of dopamine D2-type receptors in the NAc enhances wakefulness or sleep, respectively [97]. Finally, genetic removal of the murine dopamine transporter (DAT), a presynaptic protein responsible for reuptake of dopamine primarily in the BG, is associated with enhanced sleep and hypersensitivity to wake promotion by caffeine [98].
These preclinical observations were recently corroborated in humans. More specifically, brain imaging studies revealed that dopamine D2 receptors are downregulated in NAc and ventral striatum following sleep deprivation and that the decrease correlates with reduced cognitive performance [99, 100]. Furthermore, the functional polymorphism rs28363170 of the gene encoding DAT (SLC6A3 or DAT1) modulates neurophysiological markers of sleep homeostasis and the effects of caffeine on these markers in NREM sleep [101•]. The fact that genetically determined alterations in striatal dopaminergic neurotransmission modulates the actions of caffeine to promote wakefulness in rodents and humans highlights the important interplay between adenosine and dopamine in sleep–wake regulation. While other dopaminergic influences may also be important [102, 103], these findings may be consistent with an integrative role played by the NAc, and a reciprocal interplay between A2A- and D2-receptor mediated signals in regulating wakefulness and sleep.
Finally, A2A receptors have also been reported to form functional heteromers with subtype-5 metabotropic glutamate (mGlu5) receptors. The stimulation of mGlu5 receptors in A2A–mGlu5–D2 receptor heteromers causes reduced affinity of D2 receptors for dopamine, and co-stimulation of both mGlu5 and A2A receptors reduces their affinity even further [104]. Concerted activation of both mGlu5 and A2A receptors in these receptor heteromers may, therefore, efficiently reduce arousal and promote sleep. In accordance with this hypothesis, the functional availability of mGlu5 receptors in a striatal region including the NAc is enhanced compared to baseline after the experimental deprivation of one night of sleep in humans [105]. Intriguingly, the same procedure was found to reduce dopamine D2/3 receptor availability in the ventral striatum by almost the identical magnitude (~5 %) [100]. Taken together, the convergent findings may indirectly support the notion that A2A–mGlu5–D2 receptor heteromers modulate the quality of wakefulness and sleep via the NAc.
Metabolism and Adenosine
Adenosine in its basic form is an energy and ATP derivate, released from all major organs including liver, fat tissues, pancreas, and muscles. As such, it is not surprising that adenosine and adenosine receptors have been associated with the regulation of various metabolic effects in the periphery. These effects include insulin secretion from the pancreas, glucose release, glucose clearance, glycogenolysis, glycogenesis, insulin-mediated inhibition of lipolysis, leptin release from adipocytes, inhibition of ghrelin release, as well as enhancement of cholesterol synthesis in the liver (see [106] for recent in-depth review).
One hypothesis concerning the functions of sleep is that sleep is needed to conserve energy and enhance energy stores. Indeed, the regulation of metabolism by the brain has been repeatedly linked to sleep–wake regulation. This mutual relationship can be illustrated by the findings that energy demands are increased during prolonged wakefulness, whereas energy expenditure is reduced during sleep [107]. By reflecting ATP breakdown, adenosine may be an indicator of activity-dependent neuronal energy use. In accordance with a role for sleep in restoring brain energy, recent data in rats indicate that brain regions with predominantly wake-active neuronal activity such as the LHA undergo a surge in ATP during the initial hours of spontaneous sleep [108]. Interestingly, this spontaneous sleep-related ATP surge correlates positively with homeostatic sleep pressure as reflected in EEG delta activity in NREM sleep.
The neuropeptide hypocretin, which is released from the LHA, is one of the major molecules involved in feeding, temperature regulation, and metabolism. The LHA widely projects to cortex, paraventricular nucleus (PVN), nucleus tractus solitarius (NTS), NAc, VTA, as well as other parts of the ascending arousal system (Fig. 1) [21, 94, 109, 110]. Indeed, hypocretin is also a key player in regulating wakefulness and sleep. Activation of hypocretin neurons via hypocretin receptors maintains wakefulness and results in enhanced feeding, whereas loss of hypocretin neurons causes narcolepsy (see [110, 111] for recent reviews). Interestingly, adenosine can modulate the activity of hypocretin neurons of the LHA. Local injection of the selective A1 receptor antagonist 1,3-diethyl-8-phenylxanthine (DPX) enhances activity in hypocretinergic neurons and promotes waking [112]. By contrast, activation of A1 receptors in the LHA by adenosine promotes sleep [113, 114]. These findings illustrate that adenosine may contribute to sleep–wake regulation, as well as metabolism and feeding by modulating the activity of hypocretin neurons in vivo.
Other important areas for the regulation of metabolism and appetite are the ventro-medial (VMN) and arcuate (ARC) nuclei of the hypothalamus, which integrate a variety of peripheral and central signals including inputs from hypocretin neurons of the LHA [109]. The ARC modulates appetite mainly via the two hormones leptin and ghrelin. Leptin is released from adipocytes after food intake and mediates the perception of satiety. Ghrelin, on the other hand, is produced in cells of the stomach and intestines. Ghrelin levels rise during fasting and fall rapidly after food intake [115]. Apart from the ARC, neurons within the PVN and the NTS are important for satiety, taste, and autonomic functions controlling energy balance [109]. Given that adenosine modulates the activity of hypocretin neurons of the LHA, adenosine may play an indirect role in regulating satiety and appetite through these nuclei and pathways (Fig. 1), although direct evidence for this remains scarce.
A key element of metabolism is our ability to balance food intake with actual energy output. This motivational aspect of feeding is mainly associated with dopaminergic neurotransmission from VTA to NAc, which modulate hedonic and non-homeostatic food intake [109]. Food and water, or even just cues of their availability, promote dopaminergic firing of the VTA [116]. Moreover, insulin and leptin, which reflect the abundance of circulating carbohydrates and fat, can directly inhibit VTA activity and NAc signaling. By contrast, ghrelin, signaling hunger, can activate the VTA and promote dopaminergic NAc signaling. Evidence for a role of adenosine in modulating dopamine-dependent feeding behavior, comes from caffeine studies in rats. When administered orally or intraperitoneally, caffeine reduced food intake [117, 118]. Nevertheless, because adenosine receptors are widely expressed in the periphery and also modulate peripheral metabolism [106], these studies should be interpreted with caution. On the other hand, as explained above, the actions of dopamine in VTA and BG depend largely on adenosine, and especially on adenosine A2A receptors. Thus, adenosine may be excellently positioned to not only regulate sleep intensity and sleep homeostasis but also to modulate the balance between energy intake and starvation (Fig. 1). The exact roles of the distinct adenosine receptors in these processes are complex and are subject of intense ongoing research.
Conclusion
The possible roles for adenosine and adenosine receptors in regulating wakefulness and sleep were an area of active research during the past two decades. Although it is now widely accepted that endogenous adenosine acts as a sleep regulatory substance, the actions of adenosine in cortical and subcortical areas of the brain are complex and region specific. Accumulating evidence suggests that both A1 and A2A receptors modulate sleep intensity and sleep homeostasis. Much of this evidence stems from experiments in vitro and in animal models and has also been corroborated in humans. Nevertheless, causal roles for adenosine in long-term aspects of sleep–wake regulation, such as sleep homeostasis, remain controversial, especially because of its rapid synaptic removal and degradation. Thus, associated changes in adenosine signaling pathways are also under investigation. It is more and more appreciated that adenosine receptors form functional receptor heteromers with dopamine and metabotropic glutamate receptors. They may be ideally positioned, for example in NAc and LHA, not only to regulate wakefulness and sleep but also to regulate metabolism and food intake. Nevertheless, important open questions remain, highlighting the importance of future research to elucidate the exact roles for adenosine in sleep homeostasis and metabolism. This research has important implications for society and public health because the adenosine receptor antagonist, caffeine, is readily available and the most widely consumed stimulant in the world.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Benington JH, Heller HC. Restoration of brain energy metabolism as the function of sleep. Prog Neurobiol. 1995;45:347–60.
Scharf MT, Naidoo N, Zimmerman JE, Pack AI. The energy hypothesis of sleep revisited. Prog Neurobiol. 2008;86:264–80.
Petit J-M, Burlet-Godinot S, Magistretti PJ, Allaman I. Glycogen metabolism and the homeostatic regulation of sleep. Metab Brain Dis 2014:1–17.
Landolt H-P. Sleep homeostasis: a role for adenosine in humans? Biochem Pharmacol. 2008;75:2070–9.
Porkka-Heiskanen T, Kalinchuk AV. Adenosine, energy metabolism and sleep homeostasis. Sleep Med Rev. 2011;15:123–35.
Borbély AA. A two process model of sleep regulation. Hum Neurobiol. 1982;1:195–204.
Cajochen C, Chellappa S, Schmidt C. What keeps us awake?—the role of clocks and hourglasses, light, and melatonin. Int Rev Neurobiol. 2010;93:57–90. doi: 10.1016/S0074-7742(10)93003-1.
Dijk DJ, Czeisler CA. Paradoxical timing of the circadian rhythm of sleep propensity serves to consolidate sleep and wakefulness in humans. Neurosci Lett. 1994;166:63–8.
Dijk DJ, Czeisler CA. Contribution of the circadian pacemaker and the sleep homeostat to sleep propensity, sleep structure, electroencephalographic slow waves, and sleep spindle activity in humans. J Neurosci. 1995;15:3526–38.
Muheim C, Brown SA. Adenosine and other purinergic products in circadian timing. In: Masino S, Masino S, Boison D, editors. Adenosine. New York, NY: Springer New York; 2012. p. 213–32.
Wall M, Dale N. Activity-dependent release of adenosine: a critical re-evaluation of mechanism. Curr Neuropharmacol. 2008;6:329–37.
Klyuch BP, Dale N, Wall MJ. Deletion of ecto-5′-nucleotidase (CD73) reveals direct action potential-dependent adenosine release. J Neurosci. 2012;32:3842–7.
Fredholm BB, Bättig K, Holmén J, Nehlig A, Zvartau EE. Actions of caffeine in the brain with special reference to factors that contribute to its widespread use. Pharmacol Rev. 1999;51:83–133.
Sebastião AM, Cristóvão-Ferreira S, Ribeiro JA. Downstream pathways of adenosine. In: Masino S, Masino S, Boison D, editors. Adenosine. New York, NY: Springer New York; 2012.
Brundege JM, Dunwiddie TV. Metabolic regulation of endogenous adenosine release from single neurons. Neuroreport. 1998;9:3007–11.
Zimmermann H. Biochemistry, localization and functional roles of ecto-nucleotidases in the nervous system. Prog Neurobiol. 1996;49:589–618.
Burnstock G. Physiology and pathophysiology of purinergic neurotransmission. Physiol Rev. 2007;87:659–797.
Krueger JM, Huang YH, Rector DM, Buysse DJ. Sleep: a synchrony of cell activity-driven small network states. Eur J Neurosci. 2013;38:2199–209.
Langer D, Hammer K, Koszalka P, Schrader J, Robson S, Zimmermann H. Distribution of ectonucleotidases in the rodent brain revisited. Cell Tissue Res. 2008;334:199–217.
Qiu M-H, Liu W, Qu W-M, Urade Y, Lu J, Huang Z-L. The role of nucleus accumbens core/shell in sleep–wake regulation and their involvement in modafinil-induced arousal. PLoS ONE. 2012;7:e45471.
Lazarus M, Huang Z-L, Lu J, Urade Y, Chen J-F. How do the basal ganglia regulate sleep–wake behavior? Trends Neurosci. 2012;35:723–32.
Haydon PG, Carmignoto G. Astrocyte control of synaptic transmission and neurovascular coupling. Physiol Rev. 2006;86:1009–31.
Lovatt D, Xu Q, Liu W, Takano T, Smith NA, Schnermann J, et al. Neuronal adenosine release, and not astrocytic ATP release, mediates feedback inhibition of excitatory activity. Proc Natl Acad Sci U S A. 2012;109:6265–70. This study highlights the importance of astrocytes in the regulation of synaptic adenosine. It reveals how the reduction in adenosine observed following prolonged neuronal activity is not solely dependent on astrocytic ATP release, but rather on the level and duration of previous excitatory transmission. This highlights how adenosine may be able to provide activity dependent feedback signals on neuronal networks.
Halassa MM, Florian C, Fellin T, Munoz JR, Lee S-Y, Abel T, et al. Astrocytic modulation of sleep homeostasis and cognitive consequences of sleep loss. Neuron. 2009;61:213–9.
Florian C, Vecsey CG, Halassa MM, Haydon PG, Abel T. Astrocyte-derived adenosine and a1 receptor activity contribute to sleep loss-induced deficits in hippocampal synaptic plasticity and memory in mice. J Neurosci. 2011;31:6956–62.
Schmitt LI, Sims RE, Dale N, Haydon PG. Wakefulness affects synaptic and network activity by increasing extracellular astrocyte-derived adenosine. J Neurosci. 2012;32:4417–25.
Fredholm BB, Chen J-F, Cunha RA, Svenningsson P, Vaugeois J-M. Adenosine and brain function. Int Rev Neurobiol. 2005;63:191–270.
Ciruela F, Saura C, Canela EI, Mallol J, Lluis C, Franco R. Adenosine deaminase affects ligand-induced signalling by interacting with cell surface adenosine receptors. FEBS Lett. 1996;380:219–23.
Sebastião AM, Ribeiro JA. Adenosine receptors and the central nervous system. Handb Exp Pharmacol 2009:471–534.
Chen J-F, Eltzschig HK, Fredholm BB. Adenosine receptors as drug targets—what are the challenges? Nat Rev Drug Discov. 2013;12:265–86.
Elmenhorst D, Meyer PT, Winz OH, Matusch A, Ermert J, Coenen HH, et al. Sleep deprivation increases A1 adenosine receptor binding in the human brain: a positron emission tomography study. J Neurosci. 2007;27:2410–5.
Oishi Y, Huang Z-L, Fredholm BB, Urade Y, Hayaishi O. Adenosine in the tuberomammillary nucleus inhibits the histaminergic system via A1 receptors and promotes non-rapid eye movement sleep. Proc Natl Acad Sci U S A. 2008;105:19992–7.
Johansson SM, Yang JN, Lindgren E, Fredholm BB. Eliminating the antilipolytic adenosine A1 receptor does not lead to compensatory changes in the antilipolytic actions of PGE2 and nicotinic acid. Acta Physiol. 2007;190:87–96.
Yang JN, Tiselius C, Daré E, Johansson B, Valen G, Fredholm BB. Sex differences in mouse heart rate and body temperature and in their regulation by adenosine A1 receptors. Acta Physiol (Oxf). 2007;190:63–75.
Sun D, Samuelson LC, Yang T, Huang Y, Paliege A, Saunders T, et al. Mediation of tubuloglomerular feedback by adenosine: evidence from mice lacking adenosine 1 receptors. Proc Natl Acad Sci U S A. 2001;98:9983–8.
Elmenhorst D, Meyer PT, Matusch A, Winz OH, Bauer A. Caffeine occupancy of human cerebral A1 adenosine receptors: in vivo quantification with 18F-CPFPX and PET. J Nucl Med. 2012;53:1723–9. Human PET study investigating the displacement of 18F-CPFPX, a selective and competitive ligand for A 1 receptors, by caffeine. Estimating a half-life of 5 hours for caffeine in the human brain, the study suggests that roughly 4.5 cups of coffee per day will occupy up to 50% of cerebellar A 1 receptors.
Brooks DJ, Doder M, Osman S, Luthra SK, Hirani E, Hume S, et al. Positron emission tomography analysis of [11C]KW-6002 binding to human and rat adenosine A2A receptors in the brain. Synapse. 2008;62:671–81.
Zhang J-P, Xu Q, Yuan X-S, Cherasse Y, Schiffmann SN, De Kerchove d’Exaerde A, et al. Projections of nucleus accumbens adenosine A2A receptor neurons in the mouse brain and their implications in mediating sleep–wake regulation. Front Neuroanat. 2013;43. By specifically staining NAc A 2A receptor expressing neurons with a green fluorescent protein, the authors were able to accurately map their cerebral projections.
Lazarus M, Shen H-Y, Cherasse Y, Qu W-M, Huang Z-L, Bass CE, et al. Arousal effect of caffeine depends on adenosine A2A receptors in the shell of the nucleus accumbens. J Neurosci. 2011;31:10067–75. Selective and NAc specific deletion of the A 2A receptor gene in mice, reveal that A 2A receptors specifically in the shell region of the NAc are essential for the wakefulness-promoting effects of caffeine.
Yu C, Gupta J, Chen J-F, Yin HH. Genetic deletion of A2A adenosine receptors in the striatum selectively impairs habit formation. J Neurosci. 2009;29:15100–3.
Huang Z-L, Qu W-M, Eguchi N, Chen J-F, Schwarzschild MA, Fredholm BB, et al. Adenosine A2A, but not A1, receptors mediate the arousal effect of caffeine. Nature Neurosci. 2005;8:858–9.
Ledent C, Vaugeois JM, Schiffmann SN, Pedrazzini T, El Yacoubi M, Vanderhaeghen JJ, et al. Aggressiveness, hypoalgesia and high blood pressure in mice lacking the adenosine A2a receptor. Nature. 1997;388:674–8.
Ohta A, Sitkovsky M. Role of G-protein-coupled adenosine receptors in downregulation of inflammation and protection from tissue damage. Nature. 2001;414:916–20.
Lappas CM, Rieger JM, Linden J. A2A adenosine receptor induction inhibits IFN-γ production in murine CD4+ T cells. J Immunol. 2005;174:1073–80.
Eckle T, Faigle M, Grenz A, Laucher S, Thompson LF, Eltzschig HK. A2B adenosine receptor dampens hypoxia-induced vascular leak. Blood. 2008;111:2024–35.
Rosenberger P, Schwab JM, Mirakaj V, Masekowsky E, Mager A, Morote-Garcia JC, et al. Hypoxia-inducible factor-dependent induction of netrin-1 dampens inflammation caused by hypoxia. Nat Immunol. 2009;10:195–202.
Grenz A, Bauerle JD, Dalton JH, Ridyard D, Badulak A, Tak E, et al. Equilibrative nucleoside transporter 1 (ENT1) regulates postischemic blood flow during acute kidney injury in mice. J Clin Invest. 2012;122:693–710.
Eckle T, Hartmann K, Bonney S, Reithel S, Mittelbronn M, Walker LA, et al. Adora2b-elicited Per2 stabilization promotes a HIF-dependent metabolic switch crucial for myocardial adaptation to ischemia. Nat Med. 2012;18:774–82.
Johnston-Cox H, Koupenova M, Yang D, Corkey B, Gokce N, Farb MG, et al. The A2b adenosine receptor modulates glucose homeostasis and obesity. PLoS ONE. 2012;7:e40584.
Koupenova M, Johnston-Cox H, Vezeridis A, Gavras H, Yang D, Zannis V, et al. A2b adenosine receptor regulates hyperlipidemia and atherosclerosis. Circulation. 2012;125:354–63.
Björklund O, Halldner-Henriksson L, Yang J, Eriksson TM, Jacobson MA, Daré E, et al. Decreased behavioral activation following caffeine, amphetamine and darkness in A3 adenosine receptor knock-out mice. Physiol Behav. 2008;95:668–76.
Achermann P, Borbély AA. Sleep homeostasis and models of sleep regulation. In: Kryger MH, Roth T, Dement WC, editors. Principles and practice of sleep medicine. 5th ed. St. Louis: Saunders; 2011. p. 431–44.
Huston JP, Haas HL, Boix F, Pfister M, Decking U, Schrader J, et al. Extracellular adenosine levels in neostriatum and hippocampus during rest and activity periods of rats. Neuroscience. 1996;73:99–107.
Basheer R, Porkka-Heiskanen T, Stenberg D, McCarley RW. Adenosine and behavioral state control: adenosine increases c-Fos protein and AP1 binding in basal forebrain of rats. Brain Res Mol Brain Res. 1999;73:1–10.
Murillo-Rodriguez E, Blanco-Centurion C, Gerashchenko D, Salin-Pascual RJ, Shiromani PJ. The diurnal rhythm of adenosine levels in the basal forebrain of young and old rats. Neuroscience. 2004;123:361–70.
Krueger JM, Rector DM, Roy S, Van Dongen HPA, Belenky G, Panksepp J. Sleep as a fundamental property of neuronal assemblies. Nat Rev Neurosci. 2008;9:910–9.
Virus RM, Djuricic-Nedelson M, Radulovacki M, Green RD. The effects of adenosine and 2′-deoxycoformycin on sleep and wakefulness in rats. Neuropharmacology. 1983;22:1401–4.
Porkka-Heiskanen T, Strecker RE, Thakkar M, Bjorkum AA, Greene RW, McCarley RW. Adenosine: a mediator of the sleep-inducing effects of prolonged wakefulness. Science. 1997;276:1265–8.
Porkka-Heiskanen T, Strecker RE, McCarley RW. Brain site-specificity of extracellular adenosine concentration changes during sleep deprivation and spontaneous sleep: an in vivo microdialysis study. Neuroscience. 2000;99:507–17.
Sims RE, Wu HHT, Dale N. Sleep–wake sensitive mechanisms of adenosine release in the basal forebrain of rodents: an in vitro study. PLoS ONE. 2013;8:e53814.
Yang C, Franciosi S, Brown RE. Adenosine inhibits the excitatory synaptic inputs to basal forebrain cholinergic, GABAergic, and parvalbumin neurons in mice. Front Neurol. 2013;4:77.
Blanco-Centurion C, Shiromani PJ. Adenosine and sleep homeostasis in the basal forebrain. Sleep. 2006;26:8092–8100.
Franks NP. General anaesthesia: from molecular targets to neuronal pathways of sleep and arousal. Nat Rev Neurosci. 2008;9:370–86.
Palchykova S, Winsky-Sommerer R, Shen H-Y, Boison D, Gerling A, Tobler I. Manipulation of adenosine kinase affects sleep regulation in mice. J Neurosci. 2010;30:13157–65.
Franken P, Chollet D, Tafti M. The homeostatic regulation of sleep need is under genetic control. J Neurosci. 2001;21:2610–21.
Rétey JV, Adam M, Honegger E, Khatami R, Luhmann UFO, Jung HH, et al. A functional genetic variation of adenosine deaminase affects the duration and intensity of deep sleep in humans. Proc Natl Acad Sci U S A. 2005;102:15676–81.
Bachmann V, Klaus F, Bodenmann S, Schäfer N, Brugger P, Huber S, et al. Functional ADA polymorphism increases sleep depth and reduces vigilant attention in humans. Cereb Cortex. 2012;22:962–70. A controlled human sleep deprivation study which shows that a genetic reduction in ADA enzymatic activity (G/A-carriers) is associated with elevated sleep pressure, measured by enhanced EEG delta activity, as well as increased sleepiness and reduced cognitive performance.
Reichert CF, Maire M, Gabel V, Viola AU, Kolodyazhniy V, Strobel W, et al. Insights into behavioral vulnerability to differential sleep pressure and circadian phase from a functional ADA polymorphism. J Biol Rhythms. 2014;29:119–30.
Mazzotti DR, Guindalini C, de Souza AAL, Sato JR, Santos-Silva R, Bittencourt LRA, et al. Adenosine deaminase polymorphism affects sleep EEG spectral power in a large epidemiological sample. PLoS ONE. 2012;7:e44154. A large epidemiological study including 958 individuals genotyped for the ADA polymorphism and underwent polysomnographic recordings in a sleep laboratory. Their data confirmed the association between the low activity ADA variant (G/A-carriers) and enhanced EEG delta activity, supporting the association between adenosine and human sleep–wake regulation.
Wu MN, Ho K, Crocker A, Yue Z, Koh K, Sehgal A. The effects of caffeine on sleep in Drosophila require PKA activity, but not the adenosine receptor. J Neurosci. 2009;29:11029–37.
Stenberg D, Litonius E, Halldner L, Johansson B, Fredholm BB, Porkka-Heiskanen T. Sleep and its homeostatic regulation in mice lacking the adenosine A1 receptor. J Sleep Res. 2003;12:283–90.
Bjorness TE, Kelly CL, Gao T, Poffenberger V, Greene RW. Control and function of the homeostatic sleep response by adenosine A1 receptors. J Neurosci. 2009;29:1267–76.
Urade Y, Eguchi N, Qu WM, Sakata M, Huang ZL. Minireview: Sleep regulation in adenosine A2A receptor-deficient mice. Neurology. 2003;61:s94–6.
Rétey JV, Adam M, Khatami R, Luhmann UFO, Jung HH, Berger W, et al. A genetic variation in the adenosine A2A receptor gene (ADORA2A) contributes to individual sensitivity to caffeine effects on sleep. Clin Pharmacol Ther. 2007;81:692–8.
Bodenmann S, Hohoff C, Freitag C, Deckert J, Rétey JV, Bachmann V, et al. Polymorphisms of ADORA2A modulate psychomotor vigilance and the effects of caffeine on neurobehavioural performance and sleep EEG after sleep deprivation. Brit J Pharmacol. 2012;165:1904–13. Study investigating the effects ADORA2A haplotypes, corroborating, with neurophysiological measures, that caffeine sensitivity is enhanced among C alleles carriers of the 1976T > C polymorphism of the in the ADORA2A gene.
Landolt H-P. “No thanks, coffee keeps me awake”: individual caffeine sensitivity depends on ADORA2A genotype. Sleep. 2012;35:899–900.
Riksen NP, Franke B, van den Broek P, Naber M, Smits P, Rongen GA. The 22G > A polymorphism in the adenosine deaminase gene impairs catalytic function but does not affect reactive hyperaemia in humans in vivo. Pharmacogenet Genomics. 2008;18:843–6.
Mang GM, Franken P. Genetic dissection of sleep homeostasis. Curr Top Behav Neurosci 2013. doi: 10.1007/7854_2013_270.
Landolt H-P, Rétey JV, Tönz K, Gottselig JM, Khatami R, Buckelmüller I, et al. Caffeine attenuates waking and sleep electroencephalographic markers of sleep homeostasis in humans. Neuropsychopharmacol. 2004;29:1933–9.
Elmenhorst D, Basheer R, McCarley RW, Bauer A. Sleep deprivation increases A1 adenosine receptor density in the rat brain. Brain Res. 2009;1258:53–8.
Kim Y, Bolortuya Y, Chen L, Basheer R, McCarley RW, Strecker RE. Decoupling of sleepiness from sleep time and intensity during chronic sleep restriction: evidence for a role of the adenosine system. Sleep. 2012;35:861–9.
Deboer T, van Diepen HC, Ferrari MD, Van den Maagdenberg AMJM, Meijer JH. Reduced sleep and low adenosinergic sensitivity in cacna1a R192Q mutant mice. Sleep. 2013;36:127–36. This study shows that sleep induction and the responses to caffeine are modulated by a presynaptic calcium channel (the Ca(V)2.1 channel) known to be modulated by inhibitory G i -protein coupled receptors such as the A 1 receptor. Combined the data proposes a role for presynaptic calcium channels in modulating sleep–wake regulation, potentially in an A 1 receptor dependent manner.
Hayaishi O, Urade Y, Eguchi N, Huang ZL. Genes for prostaglandin d synthase and receptor as well as adenosine A2A receptor are involved in the homeostatic regulation of NREM sleep. Arch Ital Biol. 2004;142:533–9.
Scammell TE, Gerashchenko DY, Mochizuki T, McCarthy MT, Estabrooke IV, Sears CA, et al. An adenosine A2a agonist increases sleep and induces Fos in ventrolateral preoptic neurons. Neuroscience. 2001;107:653–63.
Coleman CG, Baghdoyan HA, Lydic R. Dialysis delivery of an adenosine A2A agonist into the pontine reticular formation of C57BL/6 J mouse increases pontine acetylcholine release and sleep. J Neurochem. 2006;96:1750–9.
Byrne EM, Johnson J, McRae AF, Nyholt DR, Medland SE, Gehrman PR, et al. A genome-wide association study of caffeine-related sleep disturbance: confirmation of a role for a common variant in the adenosine receptor. Sleep. 2012;35:967–75. A genome wide association study in 2,402 Australians confirms a role for the common 1976T>C polymorphism of the ADORA2A gene in modulating effects of caffeine and caffeine-related sleep disturbances.
Hohoff C, Garibotto V, Elmenhorst D, Baffa A, Kroll T, Hoffmann A, et al. Association of adenosine receptor gene polymorphisms and in vivo adenosine A1 receptor binding in the human brain. Neuropsychopharmacol. 2014;39:2989–99. An important human imaging study revealing that the ADORA2A polymorphism modulates the availability of adenosine A 1 , but not A 2A receptors in the human brain. Therefore, the data may suggest that the previous associations between this polymorphism and altered caffeine sensitivity and augmented responses to sleep deprivation are modulated by A 1 and not A 2A receptor dependent signaling.
Bachmann V, Klein C, Bodenmann S, Schäfer N, Berger W, Brugger P, et al. The BDNF Val66Met polymorphism modulates sleep intensity: EEG frequency- and state-specificity. Sleep. 2012;35:335–44.
Ciruela F, Casadó V, Rodrigues RJ, Lujan R, Burgueño J, Canals M, et al. Presynaptic control of striatal glutamatergic neurotransmission by adenosine A1-A2A receptor heteromers. J Neurosci. 2006;26:2080–7.
Ciruela F, Fernández-Dueñas V, Llorente J, Borroto-Escuela D, Cuffí ML, Carbonell L, et al. G protein-coupled receptor oligomerization and brain integration: focus on adenosinergic transmission. Brain Res. 2012;1476:86–95.
Ferraro L, Beggiato S, Tomasini MC, Fuxe K, Antonelli T, Tanganelli S. A2A/D2 receptor heteromerization in a model of Parkinson's disease. Focus on striatal aminoacidergic signaling. Brain Res. 2012;1476:96–107.
Calabresi P, Picconi B, Tozzi A, Ghiglieri V, Di Filippo M. Direct and indirect pathways of basal ganglia: a critical reappraisal. Nature Neurosci. 2014;17:1022–30.
Monti JM, Monti D. The involvement of dopamine in the modulation of sleep and waking. Sleep Med Rev. 2007;11:113–33.
Lazarus M, Chen J-F, Urade Y, Huang Z-L. Role of the basal ganglia in the control of sleep and wakefulness. Curr Opin Neurobiol. 2013;23:780–5.
Léna I, Parrot S, Deschaux O, Muffat-Joly S, Sauvinet V, Renaud B, et al. Variations in extracellular levels of dopamine, noradrenaline, glutamate, and aspartate across the sleep–wake cycle in the medial prefrontal cortex and nucleus accumbens of freely moving rats. J Neurosci Res. 2005;81:891–9.
Qu W-M, Xu X-H, Yan M-M, Wang Y-Q, Urade Y, Huang Z-L. Essential role of dopamine D2 receptor in the maintenance of wakefulness, but not in homeostatic regulation of sleep, in mice. J Neurosci. 2010;30:4382–9.
Barik S, de Beaurepaire R. Dopamine D3 modulation of locomotor activity and sleep in the nucleus accumbens and in lobules 9 and 10 of the cerebellum in the rat. Prog Neuro-Psychoph. 2005;29:718–26.
Wisor JP, Nishino S, Sora I, Uhl GH, Mignot E, Edgar DM. Dopaminergic role in stimulant-induced wakefulness. J Neurosci. 2001;21:1787–94.
Volkow ND, Tomasi D, Wang G-J, Telang F, Fowler JS, Wang RL, et al. Hyperstimulation of striatal D2 receptors with sleep deprivation: implications for cognitive impairment. Neuroimage. 2009;45:1232–40.
Volkow ND, Tomasi D, Wang GJ, Telang F, Fowler JS, Logan J, et al. Evidence that sleep deprivation downregulates dopamine D2R in ventral striatum in the human brain. J Neurosci. 2012;32:6711–7.
Holst SC, Bersagliere A, Bachmann V, Berger W, Achermann P, Landolt H-P. Dopaminergic role in regulating neurophysiological markers of sleep homeostasis in humans. J Neurosci. 2014;34:566–73. Human sleep deprivation study suggesting that a genetic reduction in human dopamine transporter expression (10 repeat homozygotes) is associated with an enhanced sleep propensity in response to sleep deprivation, as well as an enhanced sensitivity to caffeine. The data corroborates previous findings in mice and drosophila, and also supports the proposed link between dopaminergic and adenosinergic signaling in the basal ganglia and their involvement in sleep–wake regulation.
Lu J, Jhou TC, Saper CB. Identification of wake-active dopaminergic neurons in the ventral periaqueductal gray matter. J Neurosci. 2006;26:193–202.
Ueno T, Tomita J, Tanimoto H, Endo K, Ito K, Kume S, et al. Identification of a dopamine pathway that regulates sleep and arousal in Drosophila. Nature Neurosci. 2012;15:1516–23.
Popoli P, Pèzzola A, Torvinen M, Reggio R, Pintor A, Scarchilli L, et al. The selective mGlu5 receptor agonist CHPG inhibits quinpirole-induced turning in 6-hydroxydopamine-lesioned rats and modulates the binding characteristics of dopamine D2 receptors in the rat striatum. Neuropsychopharmacol. 2001;25:505–13.
Hefti K, Holst SC, Sovago J, Bachmann V, Buck A, Ametamey SM, et al. Increased metabotropic glutamate receptor subtype 5 availability in human brain after one night without sleep. Biol Psychiat. 2013;73:161–8.
Koupenova M, Ravid K. Adenosine, adenosine receptors and their role in glucose homeostasis and lipid metabolism. J Cell Physiol 2013. doi: 10.1002/jcp.24352.
Jung CM, Melanson EL, Frydendall EJ, Perreault L, Eckel RH, Wright KP. Energy expenditure during sleep, sleep deprivation and sleep following sleep deprivation in adult humans. J Physiol Lond. 2011;589:235–44.
Dworak M, McCarley RW, Kim T, Kalinchuk AV, Basheer R. Sleep and brain energy levels: ATP changes during sleep. J Neurosci. 2010;30:9007–16.
Beccuti G, Pannain S. Sleep and obesity. Curr Opin Clin Nutr Metab Care. 2011;14:402–12.
Tsujino N, Sakurai T. Role of orexin in modulating arousal, feeding, and motivation. Front Behav Neurosci. 2013;7:28.
Inutsuka A, Yamanaka A. The physiological role of orexin/hypocretin neurons in the regulation of sleep/wakefulness and neuroendocrine functions. Front Endocrinol (Lausanne). 2013;4:18.
Thakkar MM, Engemann SC, Walsh KM, Sahota PK. Adenosine and the homeostatic control of sleep: effects of A1 receptor blockade in the perifornical lateral hypothalamus on sleep–wakefulness. Neuroscience. 2008;153:875–80.
Rai S, Kumar S, Alam MA, Szymusiak R, McGinty D, Alam MN. A1 receptor mediated adenosinergic regulation of perifornical-lateral hypothalamic area neurons in freely behaving rats. Neuroscience. 2010;167:40–8.
Cun Y, Tang L, Yan J, He C, Li Y, Hu Z, et al. Orexin A attenuates the sleep-promoting effect of adenosine in the lateral hypothalamus of rats. Neurosci Bull. 2014;30:877–86.
Wren AM, Seal LJ, Cohen MA, Brynes AE, Frost GS, Murphy KG, et al. Ghrelin enhances appetite and increases food intake in humans. J Clin Endocrinol Metab. 2001;86:5992–2.
Palmiter RD. Is dopamine a physiologically relevant mediator of feeding behavior? Trends Neurosci. 2007;30:375–81.
Racotta IS, Leblanc J, Richard D. The effect of caffeine on food intake in rats: involvement of corticotropin-releasing factor and the sympatho-adrenal system. Pharmacol Biochem Behav. 1994;48:887–92.
Pettenuzzo LF, Noschang C, Von Pozzer Toigo E, Fachin A, Vendite D, Dalmaz C. Effects of chronic administration of caffeine and stress on feeding behavior of rats. Physiol Behav. 2008;95:295–301.
Compliance with Ethics Guidelines
ᅟ
Conflict of Interest
Sebastian C. Holst and Hans-Peter Landolt declare that they have no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Author information
Authors and Affiliations
Corresponding author
Additional information
This article is part of the Topical Collection on Function of Sleep
Rights and permissions
About this article

Cite this article
Holst, S.C., Landolt, HP. Sleep Homeostasis, Metabolism, and Adenosine. Curr Sleep Medicine Rep 1, 27–37 (2015). https://doi.org/10.1007/s40675-014-0007-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40675-014-0007-3