
Abstract
Background
Kidney transplantation offers the best potential for full rehabilitation in patients with end-stage kidney disease who are treated with dialysis. However, due to organ shortage which is a universal phenomenon, most patients need to be maintained on a period of dialysis therapy before the prospect of transplantation. Peritoneal dialysis (PD) could be an ideal form of renal replacement therapy due to its favorable profile toward preservation of residual renal function, patient survival, lower overall burden on cardiovascular morbidity and infection risks.
Methods
With extensive experience in PD therapy from Hong Kong where PD-first is a mandatory health policy, we reviewed the literature and present current evidence that favors PD as an optimal form of bridging renal replacement therapy prior to kidney transplantation.
Results
PD provides a viable and advantageous form of renal reaplcement particularly in terms of preservation of residual renal function, patient survival and quality of life, and cost among many other factors. Potential misconceptions that PD-related peritonitis and dialysis inadequacy are potentially deterrent factors for initiating PD therapy are clarified.
Conclusion
PD is a practical and noninferior form of renal replacement that serves as an ideal bridge from conservative therapy to kidney transplantation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
As the global burden of chronic kidney disease continues to increase, [1] the demand for renal replacement therapy (RRT) also rises. The lack of organ donors worldwide means that the majority of end-stage kidney disease patients would have to be put on dialysis therapy while awaiting the opportunity for kidney transplantation which is the best form of RRT [2]. It remains uncertain which modality of RRT should be used during this interim period. In Asia where 60% of the world’s population live, [3] accumulating experience and evidence shows that peritoneal dialysis (PD) could be the idea bridge to kidney transplantation. On this score, both Hong Kong [4] and more recently Thailand [5] have adopted a PD-first policy.
Hong Kong has the highest PD utilization rate in the world, being at around 75–80% of all dialysis patients. The PD-first policy was implemented in 1985, initially to cope with the scarcity of hospital space and manpower in performing in-center hemodialysis [6]. The policy meant that all end-stage renal disease patients requiring dialysis were treated with PD first unless they had a medical contraindication in doing so. This allowed the government to support more patients with end-stage renal disease in receiving renal replacement therapy. Over the years, Hong Kong has accumulated good experience with PD in that it is non-inferior or even superior to hemodialysis. Here, we present evidence showing PD can be an ideal bridging therapy to kidney transplantation.
Residual renal function
In consideration of an ideal form of RRT, several principles apply. First, one should consider whether the form of RRT could preserve residual renal function (RRF) as it is associated with improved patient survival [7]. In this regard, PD does preserve RRF and the postulated mechanisms include greater hemodynamic stability, less ischemic kidney insult, and lack of inflammatory mediators generated by the extracorporeal hemodialysis circuit encountered during hemodialysis. Previous studies have shown a more rapid decline in RRF after starting hemodialysis versus PD. Indeed, many subsequent studies found no difference in survival between patients treated with PD and hemodialysis, which is also confirmed by the 2018 US Renal Data System report. In a recent systematic review, [8] PD was also associated with a 16% lower risk of hemorrhagic stroke compared to hemodialysis, though the overall stroke risk was not different between the two modalities. This will have substantial implications with regard to suitability to kidney transplantation and the subsequent cardiovascular risks after transplantation, as patients who survive major hemorrhagic strokes are more likely to have a significant residual neurologic deficit which could undermine their suitability for transplantation. In addition, anti-platelet agents or anti-coagulants which are often needed in CKD/ESRD patients due to advanced vascular age [9] even after kidney transplantation are also relatively contraindicated in patients with a history of major a hemorrhagic stroke.
Patient survival
Second, it is important to know if PD could adversely affect patient survival versus conservative treatment or other forms of RRT. A re-analysis of the CANUSA study [10] has already demonstrated preservation of residual renal function contributed significantly to the overall health and survival of dialysis patients. Many studies have shown a significant association between survival advantage and receiving PD in the initial period of dialysis therapy [11]. This remains true when only incident patients with at least 4 months of pre-dialysis care were included to eliminate any selection bias arising from patients who required emergency start of dialysis. In a propensity-matched mortality comparison of incident hemodialysis and peritoneal dialysis patients from the USA, [12] such survival advantage using PD was most evident during the first 2 years of dialysis initiation. Studies from other continents [13,14,15] reported similar findings (Table 1). The only exception of superior survival in PD over HD is observed in home HD patients in which patients who transitioned to PD after 12 months of dialysis had worse survival than their HHD counterparts [16]. Data from the US Renal Data System also found that mortality rates among patients on hemodialysis patients have declined only very little in the US over the years, while those for patients on PD have a sustained decline over time. Indeed, a systemic review found no evidence-based arguments in favour or against a particular modality of dialysis as the first RRT of choice in patients with diabetes who reach end-stage renal disease [17]. More recently, however, a meta-analysis suggested that PD and in-center HD carry equivalent survival benefits with substantial heterogeneity largely accounted for by differences in cohort period, study type and country of origin [18].
Peritonitis and other infective risks
One fear and hence reluctance in accepting PD in some countries has been PD-related peritonitis, which is a common serious complication of PD that results in considerable morbidity, mortality, and health care costs including hospitalization. With extensive use of the disconnect and double bag system, PD patients in general have a fairly low peritonitis rate. According to the Hong Kong Renal Registry, the PD peritonitis rate has improved from 1 per 25 patient-months (or 0.48 episode per patient year) in 2001 to 1 per 35 patient-months (or 0.34 episode per patient year) in 2011 [11] By 2018, the peritonitis rate in Australia has further dropped to 0.33 episode per patient year. Likewise PD peritonitis rates also improved in Australia and New Zealand from 0.63 episode per patient year in 2003–2004 to 0.43 episodes per patient year in 2011 [19]. By 2018, the peritonitis rate in Australia has further dropped to 0.32 episode per patient year (ANZDATA Annual Report 2019—Chapter 5). In a recently analysis from the Peritoneal Dialysis Outcomes and Practice Patterns Study (PDOPPS), [20] the overall peritonitis rates, in episodes per patient-year, were 0.40 (95% CI 0.36–0.46) in Thailand, 0.38 (95% CI 0.32–0.46) in the United Kingdom, 0.35 (95% CI 0.30–0.40) in Australia/New Zealand, 0.29 (95% CI 0.26–0.32) in Canada, 0.27 (95% CI 0.25–0.30) in Japan, and 0.26 (95% CI 0.24–0.27) in the United States. Thus, it is envisaged that peritonitis improves with time and experience of the PD center. Significant differences in peritonitis rates among different countries may result from varied and potentially modifiable treatment practices. In addition to peritonitis, overall infection rates between hemodialysis and PD patients were similar (hemodialysis 0.77/year vs. PD 0.86/year, p = 0.24) [21]. Hemodialysis patients are at risk of bacteremia during the first 90 days of access creation, whereas the risk of peritonitis for PD patients was not different over time. Therefore, the access for PD is not particularly more problematic than that for hemodialysis.
For hemodialysis patients, although there is no concern about treatment related peritonitis, they are susceptible to vascular access infection and appear to be more susceptible to infection than PD patients. In a USRDS study including nearly 300,000 incident dialysis patients, the rate of pneumonia was 59% higher in hemodialysis versus PD patients.
Dialysis adequacy
Adequacy of dialysis should be interpreted clinically rather than by targeting only solute and fluid removal, but it is generally accepted that a weekly Kt/V for urea should be at least 1.7 [22]. Evaluation should also include both peritoneal and renal creatinine clearances, electrolyte and acid–base balance, nutritional status, calcium and phosphate control, haemoglobin, responsiveness to erythropoietin-stimulating agents, and diabetic control. For patients with signs and symptoms of under-dialysis, one should ensure compliance to the prescribed PD, followed by a trial of increasing dialysis dose such as by increasing the frequency or volume of each exchange [6]. Conversion to hemodialysis is an option if these manoeuvres fail. It is important to note that adequate doses of dialysis could improve the overall well-being such as hemoglobin levels, nutrition, blood pressure and even bone health of the patient which has an indirect positive impact on the outcome of kidney transplantation.
Quality of life
Quality of life is an important aspect of dialysis care. In a meta-analysis, continuous ambulatory PD was found to have better psychological health and less emotional stress than in-center or even home hemodialysis patients [23]. In another prospective cohort study including 37 US centers, patients receiving PD rated their care higher than those receiving hemodialysis [24]. It is envisaged that PD as a home based therapy that involves only limited time for each PD fluid exchange would allow patients to work normally, where in-center hemodialysis mandates time off work at least for 2–3 half-days per week. Besides, hemodialysis induced electrolyte shifts causing muscle cramps, hypotension or even myocardial stunning is not observed with PD therapy. Thus, it is not surprising that PD confers a better quality of lift versus hemodialysis.
Role of incremental PD
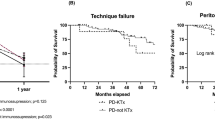
Another interesting notion is the use of incremental PD as a first-choice RRT. This strategy involves elective start of low-dose PD which is gradually increased to compensate for subsequent loss of residual renal function to maintain dialysis adequacy in terms of small solute clearance (i.e., peritoneal plus endogenous Kt/V). It appears to be a suitable home-based RRT modality affecting less of the patient’s social and active work schedules at first, and spares vascular access and cost due to lower usage of PD fluids. In Italy, this approach has become the standard of practice at some institutions as a bridge to renal transplantation. In a comparative study, [25] 17 patients on incremental PD and 24 patients on hemodialysis received their first renal transplant and it was observed that incremental PD was associated with low morbidity and better 1-year graft function versus the hemodialysis group. A recent systematic review also found that incremental dialysis allows longer preservation of residual kidney function without increasing mortality [26].
Outcome of transplant recipients by previous RRT modality
One lingering question is whether previous PD or hemodialysis confers a better clinical outcome after successful kidney transplantation. A recent study showed that the modality of renal replacement therapy prior to renal transplantation, be it PD or hemodialysis, did not affect the outcomes of the living donor renal allograft recipients [27]. On the other hand, in a meta-analysis that compared key transplant outcomes for patients on hemodialysis with those on PD, [28] improved patient survival and a lower incidence of delayed graft function (DGF) was observed in PD patients. The reported adjusted risk ratios for 5-year mortality and DGF, being 0.89 (95% confidence interval [CI] 0.82–0.97, p = 0.006) and 0.5 (95% CI 0.41–0.63, p < 0.005), respectively, were both in favor of PD, though there was no demonstrable graft survival advantages at 5 years with an adjusted risk ratio of 0.97 (95% CI 0.92–1.01, p = 0.16). These data favor PD as a pre-transplant modality. In reality, nephrologists need to balance the potential merits of these data during the decision-making process when managing patients with transplant potential who are approaching the need for RRT.
Cost
Renal replacement therapy is always one of the most costly forms of chronic treatment in any healthcare system around the world. To this end, different countries have different reimbursement systems, [3] and a head-to-head comparison is hard to make. In Hong Kong, one important reason for prioritizing PD in incident dialysis patients is the perceived economic advantage. Opinion leaders seem to have a general consensus that in-center hemodialysis is more expensive than home-based modalities, including CAPD, automated PD, and nocturnal home hemodialysis. As a home-based therapy, PD can improve patient survival, preserve RRF and lower infection risk in patients with end-stage renal disease while at the same time reduce financial stress to the government because of its cost-effectiveness.
Role of PD in special scenarios
In late-presenting end-stage renal disease patients, urgent-start hemodialysis is usually performed via a central venous catheter. However, PD can be a safe, efficient and cost-effective alternative to hemodialysis. Compared to urgent-start haemodialysis via a central venous catheter, urgent-start PD has significantly lower incidences of catheter-related bloodstream infections, dialysis-related complications and need for dialysis catheter re-insertions during the initial phase of the therapy [29].
Another subgroup of patients who may benefit from PD as a bridge to transplantation is chronic combined liver and kidney failure patients. These patients face multiple challenges, including complications related to fluid shifts, bleeding esophageal varices, and spontaneous infections. RRT in the form of hemodialysis is often poorly tolerated due to intravascular instability found in cirrhotic subjects. The ideal treatment is simultaneous liver-kidney transplantation, but organ scarcity often mandates a long waiting time of months to even years for transplant. PD is an alternative strategy to hemodialysis in this context, as it provides both renal clearance and management of large-volume ascites. Traditionally, PD has been rarely practiced in patients with liver failure due to concerns about increased peritonitis rates, protein loss, which could have a negative impact on the suitability of transplantation. A recent study comparing 285 PD to 1140 hemodialysis patients with cirrhosis have shown that PD is associated with a lower mortality independent of patients’ comorbidity, severity of liver cirrhosis, and serum albumin levels [30]. However, data regarding the severity of liver disease and successful SLKT after PD maintenance are lacking. In a small single-center series of 12 patients [31] who were awaiting combined liver and kidney transplant and put on PD, there was no mortality and the need for large-volume paracentesis often seen in cirrhotics was obviated. A quarter of the subjects were subsequently successfully transplanted, suggesting that PD is a viable bridging therapy for patients with liver and kidney failure who await SLKT.
Conclusion
Given the utility and potential advantages of PD as a bridging therapy to kidney transplantation, there is a need to increase its utilization which is low in many parts of the world especially in western countries. The US administration also signed an executive order in Jul 2019 to drastically increase home therapy for kidney disease in USA, by getting 80% of patients who are under treatment either in-home dialysis or transplanted eventually (https://www.npr.org/sections/health-shots/2019/07/10/740276389/trump-administration-announces-plans-to-shake-up-the-kidney-care-industry). Home therapy is also particularly relevant in the face of the COVID-19 pandemic as it combines dialysis with social distancing and elimination of transportation needs [32, 33]. The success of the PD-first policy requires the support of dedicated staff and well-designed patient training programmes [6] as well as a timely start of PD [34] To ensure the sustainability of advocating PD-first, potential problems with PD also need to be addressed adequately, including peritonitis, ultrafiltration failure and dialysis adequacy. A Kt/V for urea of 1.7 per week has been defined as a threshold for anuric PD patients [35]. In addition, enhancing hemodialysis support as back-up and promoting organ donation are necessary to meet the demands of the rapidly growing dialysis population. Apart from CAPD, other PD modalities also have distinct advantages such as automated PD which was introduced in Hong Kong since 1988. The success of a PD program also hinges upon a critical threshold size of a PD unit that would accumulate experience in PD care with time.
References
Collaboration GBDCKD. Global, regional, and national burden of chronic kidney disease, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 395:709–733
Tang S, Lui SL, Li FK et al (1999) Long-term renal allograft recipients from South-east Asia in the pre- cyclosporin era. IntJ Artif Org 22:131–137
Tang SCW, Yu X, Chen HC et al (2020) Dialysis Care and Dialysis Funding in Asia. Am J Kidney Dis 75:772–781
Li PK, Chow KM (2013) Peritoneal dialysis-first policy made successful: perspectives and actions. Am J Kidney Dis 62:993–1005
Changsirikulchai S, Sriprach S, Thokanit NS et al (2018) Survival analysis and associated factors in Thai patients on peritoneal dialysis under the PD-first policy. Perit Dial Int 38:172–178
Lai KN, Lo WK (1999) Optimal peritoneal dialysis for patients from Hong Kong. Perit Dial Int 19(Suppl 3):S26–S31
Diaz-Buxo JA, Lowrie EG, Lew NL et al (1999) Associates of mortality among peritoneal dialysis patients with special reference to peritoneal transport rates and solute clearance. Am J Kidney Dis 33:523–534
Boonpheng B, Thongprayoon C, Cheungpasitporn W (2018) The comparison of risk of stroke in patients with peritoneal dialysis and hemodialysis: a systematic review and meta-analysis. J Evid Based Med 11:158–168
Lin M, Chan GC, Chan KW et al (2020) Vascular age is associated with the risk of dialysis or death in chronic kidney disease. Nephrol (Carlton) 25:314–322
Bargman JM, Thorpe KE, Churchill DN (2001) Relative contribution of residual renal function and peritoneal clearance to adequacy of dialysis: a reanalysis of the CANUSA study. J Am Soc Nephrol 12:2158–2162
Choy AS, Li PK (2015) Sustainability of the peritoneal dialysis-first policy in Hong Kong. Blood Purif 40:320–325
Weinhandl ED, Foley RN, Gilbertson DT et al (2010) Propensity-matched mortality comparison of incident hemodialysis and peritoneal dialysis patients. J Am Soc Nephrol 21:499–506
McDonald SP, Marshall MR, Johnson DW et al (2009) Relationship between dialysis modality and mortality. J Am Soc Nephrol 20:155–163
Liem YS, Wong JB, Hunink MG et al (2007) Comparison of hemodialysis and peritoneal dialysis survival in The Netherlands. Kidney Int 71:153–158
Sanabria M, Muñoz J, Trillos C et al (2008) Dialysis outcomes in Colombia (DOC) study: a comparison of patient survival on peritoneal dialysis vs hemodialysis in Colombia. Kidney Int Suppl 108:S165–S172
Choi SJ, Obi Y, Ko GJ et al (2020) Comparing patient survival of home hemodialysis and peritoneal dialysis patients. Am J Nephrol 51:192–200
Couchoud C, Bolignano D, Nistor I et al (2015) Dialysis modality choice in diabetic patients with end-stage kidney disease: a systematic review of the available evidence. Nephrol Dial Transplant 30:310–320
Elsayed ME, Morris AD, Li X et al (2020) Propensity score matched mortality comparisons of peritoneal and in-centre haemodialysis: systematic review and meta-analysis. Nephrol Dial Transplant [published online ahead of print, 2020 Jan 25]
Cho Y, Johnson DW (2014) Peritoneal dialysis-related peritonitis: towards improving evidence, practices, and outcomes. Am J Kidney Dis 64:278–289
Perl J, Fuller DS, Bieber BA et al (2020) Peritoneal Dialysis-Related Infection Rates and Outcomes: Results From the Peritoneal Dialysis Outcomes and Practice Patterns Study (PDOPPS). Am J Kidney Dis 76:42–53
Aslam N, Bernardini J, Fried L et al (2006) Comparison of infectious complications between incident hemodialysis and peritoneal dialysis patients. Clin J Am Soc Nephrol 1:1226–1233
Lo WK, Lui SL, Chan TM et al (2005) Minimal and optimal peritoneal Kt/V targets: results of an anuric peritoneal dialysis patient's survival analysis. Kidney Int 67:2032–2038
Cameron JI, Whiteside C, Katz J et al (2000) Differences in quality of life across renal replacement therapies: a meta-analytic comparison. Am J Kidney Dis 35:629–637
Rubin HR, Fink NE, Plantinga LC et al (2004) Patient ratings of dialysis care with peritoneal dialysis vs. hemodialysis. JAMA 291:697–703
Domenici A, Comunian MC, Fazzari L et al (2011) Incremental peritoneal dialysis favourably compares with hemodialysis as a bridge to renal transplantation. Int J Nephrol 2011:204216
Garofalo C, Borrelli S, De Stefano T et al (2019) Incremental dialysis in ESRD: systematic review and meta-analysis. J Nephrol 32:823–836
Prasad N, Vardhan H, Baburaj VP et al (2014) Do the outcomes of living donor renal allograft recipients differ with peritoneal dialysis and hemodialysis as a bridge renal replacement therapy? Saudi J Kidney Dis Transpl 25:1202–1209
Joachim E, Gardezi AI, Chan MR et al (2017) Association of pre-transplant dialysis modality and post-transplant outcomes: a meta-analysis. Perit Dial Int 37:259–265
Javaid MM, Khan BA, Subramanian S (2019) Peritoneal dialysis as initial dialysis modality: a viable option for late-presenting end-stage renal disease. J Nephrol 32:51–56
Chou CY, Wang SM, Liang CC et al (2016) Peritoneal dialysis is associated with a better survival in cirrhotic patients with chronic kidney disease. Med (Baltimore) 95:e2465
Jones RE, Liang Y, MacConmara M et al (2018) Peritoneal dialysis is feasible as a bridge to combined liver-kidney transplant. Perit Dial Int 38:63–65
Ikizler TA, Kliger AS (2020) Minimizing the risk of COVID-19 among patients on dialysis. Nat Rev Nephrol 16:311–313
Chan KW, Wong VT, Tang SCW (2020) COVID-19: An Update on the Epidemiological, Clinical, Preventive and Therapeutic Evidence and Guidelines of Integrative Chinese-Western Medicine forthe Management of 2019 Novel Coronavirus Disease. Am J Chin Med 48:737–762
Tang SC, Ho YW, Tang AW et al (2007) Delaying initiation of dialysis till symptomatic uraemia–is it too late? Nephrol Dial Transplant 22:1926–1932
Lo WK, Ho YW, Li CS et al (2003) Effect of Kt/V on survival and clinical outcome in CAPD patients in a randomized prospective study. Kidney Int 64:649–656
Acknowledgements
This study was supported by a philanthropic donation from Mrs. Rita T. Liu SBS of L & T Charitable Foundation Ltd. & Indo Café. Part of the results from this study was presented at the 60th National Congress of the Italian Society of, 2–5 Oct, 2019, Rimini, Italy.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Ethical approval
This article doesn’t contain any studies with human participants or animals performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Tang, S.C.W., Lai, K.N. Peritoneal dialysis: the ideal bridge from conservative therapy to kidney transplant. J Nephrol 33, 1189–1194 (2020). https://doi.org/10.1007/s40620-020-00787-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40620-020-00787-0