
Abstract
Introduction
The aim of the present study was to document the role of ultrasound in the diagnosis and management of symptomatic hydronephrosis during pregnancy.
Methods
In this study, we reviewed 36 consecutive cases of pregnant women whose pregnancy was complicated by symptomatic hydronephrosis. In all patients, management was initially conservative (analgesics and fluids) after hospitalization. The following criteria were used to indicate double-J stent placement under US guidance rather than a conservative treatment: persistent pain with no improvement after conservative treatment, progressive hydronephrosis (>2 cm dilatation of the renal pelvis) or presence of uterine contractions.
Results
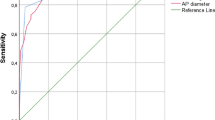
The mean patient’s age was 25 years (17–35) and gestational age at clinical presentation was 24 weeks (13–37). 81 % of cases had a renal pelvis dilatation >2 cm, while in only 19 % of cases there was a hydronephrosis between 1 and 2 cm in diameter; however, calculi were confirmed only in 25 patients. 28 patients required an invasive management with double-J stent insertion under US guidance. The sensitivity and specificity of US in the etiological diagnosis of hydronephrosis during pregnancy was 83 and 91 %, respectively.
Conclusion
Conservative management with medical therapy and observation should be the first-line treatment approach. In our opinion a rapid ureteral decompression with the insertion of a ureteral double-J stent, under US visualization, is the safest method in the treatment of pregnant women with obstructed renal systems.
Riassunto
Introduzione
Lo scopo del presente studio è stato quello di analizzare il ruolo dell’ecografia nella diagnosi e gestione durante la gravidanza di pazienti affette da idronefrosi sintomatica.
Metodi
In questo studio abbiamo preso in esame 36 casi di donne in gravidanza complicata dall’insorgenza di un’idronefrosi sintomatica. In tutti i pazienti fu adottato dopo il ricovero in un primo momento un trattamento conservativo (con idratazione e analgesici). I criteri utilizzati per porre indicazione nel posizionamento di uno stent doppio J sotto guida ecografica al posto di un trattamento conservativo sono stati: dolore al fianco persistente senza alcun miglioramento dopo terapia medica, progressivo incremento del quadro idronefrotico (diametro della pelvi renale >2 cm) o comparsa di contrazioni uterine.
Risultati
L’età media delle pazienti è stata di 25 anni (range 17–35), mentre l’età gestazionale al momento della presentazione del quadro clinico è stata di circa 24 settimane (range 13-37). L’81 % delle pazienti aveva una dilatazione della pelvi renale >2 cm, mentre solo nel 19 % c’è stata un idronefrosi compresa tra 1 e 2 cm di diametro; tuttavia la presenza di calcolosi è stata confermata in sole 25 pazienti. In ventotto pazienti è stata necessaria una gestione invasiva con posizionamento di stent doppio J sotto guida ecografica. La sensibilità e la specificità dell’ecografia nella diagnosi eziologica d’idronefrosi è stata dell’ 83 % e del 91 % rispettivamente.
Conclusioni
Secondo il nostro parere un trattamento conservativo con terapia medica ed osservazionale dovrebbe essere l’approccio di prima linea; una rapida decompressione ureterale con l’inserimento di un stent ureterale doppio J sotto guida ecografica è il metodo più sicuro nel trattamento di donne in stato di gravidanza che presentano ostruzione delle vie escretrici superiori.

Similar content being viewed by others


References
Biyani CS, Joyce AD (2002) Urolithiasis in pregnancy: pathophysiology, fetal consideration and diagnosis. BJU Iint 89:811–818
Hoscan MB, Ekinci M, Tunckiran A, Oksay T, Ozorak A, Ozkardes H (2012) Management of Symptomatic ureteral calculi complicating pregnancy. Urology 80(5):1011–1014
Kilpatrick CC, Monga M (2007) Approach to the acute abdomen in pregnancy. Obstet Gynecol Clin North Am 34(3):389–402
Oto A, Ernst RD et al (2009) MR imaging in the triage of pregnant patients with acute abdominal and pelvic pain. Abdom Imaging 34(2):243–250
Elgamasy A, Elsherif A (2009) Use of Doppler ultrasonography and rigid ureteroscopy for managing symptomatic ureteric stones during pregnancy. BJU International 106:262–266
Evans HJ, Wollin TA (2001) The management of urinary calculi in pregnancy. Curr Opin Urol 11:379–384
Stothers L, Lee LM (1992) Renal colic in pregnancy. J Urol 148:1383–1387
McAleer SJ, Loughlin KR (2004) Nepphrolithiasis and pregnancy. Curr Opin Urol 14:123–127
Fabrizio MD, Gray DS, Feld RI, Bagley DH (1996) Placement of ureteral stents in pregnancy using ultrasound guidance. Tech Urol 2:121–125
Brent RL (1989) The effect of embryonic and fetal exposure to X-ray, microwaves and ultrasound: counselling the pregnant and non pregnant patient about these risks. Semin Oncol 16:347–368
Watterson JD, Girvan AR, Beiko DT et al (2002) Ureteroscopy and holmium: YAG laser lithotripsy: an emerging definitive management strategy for symptomatic ureteral calculi in pregnancy. Urology 60:383–387
Turk C, Knoll T, Petrik A et al: Guidelines on Urolithiasis. European Association of Urology 2013: 55
Denstedt JD, Razvi H (1992) Management of urinary calculi during pregnancy. J Urol 148:1072–1074
Charalambous S, Fotas A, Rizk DE (2009) Urolithiasis in pregnancy. Int Urogynecol J Pelvic Floor Dysfunct 9:1133–1136
White WM, Zite NB, Gash J et al (2007) Low-dose computed tomography for evaluation of flank pain in the pregnant population. J Endourol 21:1255–1260
Patel SJ, Reede DL, Katz DS et al (2007) Imaging the pregnant patient for nonobstetric conditions: algorithms and radiation dose considerations. Radiographics 27:1705–1722
McNeily AE, Goldenberg SL, Allen GJ, Cooperberg PL (1991) Sonographic visualization of the ureter in pregnancy. J Urol 146:289–301
Mitterberger M, Pinggera GM, Maier E et al (2007) Value of 3-dimensional transrectal/transvaginalsonography in diagnosis of distal ureteral calculi. J Ultrasound Med 26:19–27
Rana AM, Aquil S, Khawaja AM (2009) Semirigidureteroscopy and pneumatic lithotripsy as definitive management of obstructive ureteral calculi during pregnancy. Urology 73:964–967
Akpinar H, Tufek I, Alici B, Kural AR (2006) Ureteroscopy and holmium laser lithotripsy in pregnancy: stents must be used postoperatively. J Endourol 20:107–110
Delakas D, Karyotis I, Loumbakis P et al (2000) Ureteral drainage by double-J-catheters during pregnancy. Clin Exp Obstet Gynecol 27:200–202
Conflict of interest
Lucio Dell’Atti declares that I have no conflict of interest.
Informed consent
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000 (5). All patients provided written informed consent to enrollment in the study and to the inclusion in this article of information that could potentially lead to their identification.
Human and animal studies
The study was conducted in accordance with all institutional and national guidelines for the care and use of laboratory animals
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Dell’Atti, L. Our ultrasonographic experience in the management of symptomatic hydronephrosis during pregnancy. J Ultrasound 19, 1–5 (2016). https://doi.org/10.1007/s40477-014-0109-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40477-014-0109-2