
Abstract
Purpose
To study the relationship between the tooth-brushing habits during the preschool ages and caries prevalence at the age of 5 years and to investigate a possible association with the mode of delivery.
Methods
The study population consisted of 336 children that were orally examined at 2, 3 and 5 years. All stages of caries were scored on tooth and surface level. Data on tooth brushing behaviour were collected through semi-structured interviews.
Results
At 5 years, the attrition rate was 13.1%. The total caries prevalence (cavitated and non-cavitated lesions) was 18.9%. The vast majority of the parents assisted their child with the brushing and 98% used fluoride toothpaste. The relative risk (RR) for caries was significantly (p < 0.05) increased for “tooth brushing less than twice daily” at two (RR 2.1, 95% CI 1.3–3.3, p < 0.01) and 3 years (RR 3.6, 95% CI 2.0–6.7; p < 0.001). Likewise, reporting “major/minor difficulties to perform tooth brushing” at 2 and 3 years was significantly related to caries development at the age of five (RR 1.5, 95% CI 1.0–2.4, p < 0.05 and RR 2.5, 95% CI 1.4–4.3; p < 0.01). We found no significant association between the tooth brushing habits and the mode of delivery.
Conclusions
Less than twice daily tooth-brushing and difficulties to perform the procedure during the first preschool years were significant determinants of caries prevalence at the age of 5 years. Health professionals should, therefore, give special attention and assist parents to improve and optimize their tooth brushing behaviour during the preschool years.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
There is strong evidence from systematic reviews that daily tooth brushing with fluoride toothpaste is effective in the prevention of early childhood caries (Mejàre et al. 2015; Twetman and Dhar 2015). The prevented fraction is estimated to 31% in the primary when tooth brushing with fluoride at concentrations of at least 1000 ppm F is compared with no fluoride (dos Santos et al. 2013; Santos et al. 2013). The timing seems to be of importance and it is suggested that tooth brushing should be commenced not later than at 1 year-of age (Kumar et al. 2016). The best evidence comes from randomized controlled trials and from prospective observational studies; recent data from a Norwegian birth cohort have confirmed the importance of an early start and twice daily brushing with fluoride toothpaste to reduce the development of dental caries from 2 to 5 years of age (Wigen and Wang 2015, 2017; Wigen et al. 2018). We have previously described the influence of birth-related and family factors on early childhood caries development up to the age of 5 years in a birth cohort that was monitored prospectively (Boustedt et al. 2018). Among the factors significantly associated with caries, the mode of delivery, parental smoking and siblings with caries were most influential. In this communication, we describe the relationship between tooth brushing behaviour during preschool years and caries prevalence at the age of 5 years. A second aim was to investigate a possible association between the mode of delivery and the tooth brushing habits at the age of 2 and 3 years.
Materials and methods
Study group
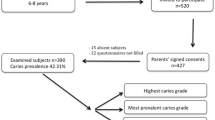
The original population-based birth cohort, born between 2007 and 2009, comprised 2666 infants that were enrolled in a prospective study with focus on growth and overweight (Roswall et al. 2016). From this group, 395 randomly selected children were invited to a dental study and the parents of 346 infants (52% boys, 48% girls) accepted the invitation. At the age of 2-years, 336 children showed up for a baseline examination at the Maxillofacial Unit, Halland hospital, Halmstad, Sweden. At the ages of 3 and 5 years, 302 and 292 children, respectively, were re-examined with respect to caries. The main reason for the attrition was family relocation but a few families claimed lack of interest or time. All children were born and citizens of the Halland region, located in south-western Sweden. The study was approved by the Regional Ethical Review Board in Lund and a written informed consent was obtained from the custodians. All the children had parallel access to regular preventive-oriented dental care during the entire project, provided free of charge by the regional Public Dental Care. The fluoride level in the piped drinking water was < 0.3 ppm in the part of the region from which the participants were recruited.
Clinical examination and data collection
The children were examined in a fully equipped paediatric dental office by one of two experienced and calibrated examiners at the age of 2, 3 and 5 years. The occurrence of manifest caries (cavitated lesions) was scored on tooth and surface level according to the WHO-criteria (2013). In addition, early non-cavitated early lesions were defined as a carious opacity or visual colour change (white to brown) of the enamel along the gingival margin with a rough surface but with no evidence of enamel breakdown. The caries prevalence was expressed as the proportion of children with a sum of non-cavitated and cavitated, missed and filled teeth (dmft > 0). Radiographs were exposed on the 5-year-olds based on the individual need. At the implementation of the project, the two examiners scored 10 preschool children independently and any discrepancies were discussed and solved through consensus. The inter-examiner agreement was 90%. Information on tooth brushing habits was captured through a standard questionnaire at baseline and at the recall examinations. The answers were reviewed by the examiner and discussed with the parents to give feedback, unveil possible problems and empower good tooth brushing behaviour. The parents were asked to categorise their child’s compliance with tooth brushing into three levels; score 0 (no problem) = the child co-operates well; score 1 (minor problems) = tooth brushing is performed with difficulty; the child seeks to avoid the procedure, and, score 2 (major problems) = parent is more or less unable to brush, the child averts the procedure.
Statistical methods
All data were processed with the IBM SPSS software (version 25.0; Chicago, USA). The influence of tooth brushing habits on the presence of caries (non-cavitated + cavitated lesions) at 5 years of age was analysed with Chi-square tests and expressed as relative risk with 95% confidence intervals. Chi-square tests were used for the comparison of two proportions, expressed as a percentage. We considered p values less than 0.05 as statistically significant.
Results
Over 93% of the parents were born in Sweden and 68.3% of the mothers and 45.4% of the fathers reported education on university level. At the age of 5 years, the total caries prevalence was 18.9% with 6.5% having cavitated lesions. Data on the tooth brushing habits are presented in Table 1. The vast majority (98%) used fluoride toothpaste and most 2-year-olds (78%) had their teeth brushed by an adult twice a day. This figure increased to 90% at the age of 5 years. Less than 5% reported non-daily tooth brushing at the age of 2 years and almost 31% experienced major or minor difficulties to perform the procedure in an acceptable way. In Table 2, the relationship between the reported tooth brushing behaviour at the age of 2 and 3 years and caries prevalence at 5 years is shown. The relative risk for caries was significantly (p < 0.05) increased for “tooth brushing less than twice daily” and “major/minor difficulties to perform tooth brushing” both at 2 and 3 years. The variables “brushing always performed by an adult (yes/no)” and “fluoride toothpaste (yes/no)” failed to reach statistical significance. In the children with caries at 5 years, tooth brushing was commenced somewhat later (mean age 8.7 months, SD 3.6) than among those that remained caries-free (mean age 7.9 months, SD 3.3) but the difference was not statistically significant.
The tooth brushing habits at 2 and 3 years in relation to the mode of delivery are shown in Table 3. The proportion of children with less than twice daily tooth brushing was slightly higher among children delivered with caesarean section but the difference compared to those with vaginally birth was not statistically significant.
Discussion
Dental caries is a complex non-communicable disease with a high prevalence across the life span (Pitts et al. 2017). While some determining factors are not readily modifiable, such as genetics and socioeconomic status, sugar reduction and oral hygiene are lifestyle and behavioural factors that can be addressed early in life. In this cohort of Swedish-born children to relatively well-educated parents, tooth brushing was introduced at an early age; 95% of the parents had started to brush their children teeth at the age of 1 year (Boustedt et al. 2018). Furthermore, the use of 1000 ppm fluoride-containing toothpastes was practically mandatory as very few non-fluoride, or low-fluoride products, were available in Sweden at the time of the study. In this context, our main finding of tooth brushing frequency and the cooperation with its performance during early childhood as discriminating factors for future caries development was interesting. The results confirmed findings from previous studies in Scandinavia (Wigen and Wang 2015, 2017). Although a regular mechanical disruption of the oral biofilm is a key event for the maintenance of oral health (Twetman 2018) it should be underlined that tooth brushing in the absence of fluorides has failed to show a benefit in terms of reducing the incidence of dental caries (Hujoel et al. 2018). The toothbrush is probably the most convenient and accepted tool to bring fluoride into the oral cavity (Marinho et al 2009) and, needless to say, when brushing is infrequent or associated with problems, the child will not benefit from the topical mechanisms of fluoride action. Our results suggest that the oral biofilm should be exposed to fluoride ions more often than once per day to maximize its caries-preventive effect and this knowledge must be emphasized to parents. Likewise, parents encountering difficulties to perform the tooth brushing should be offered empowerment and hands-on training by oral health personnel. Such preventive measures have the potential to be cost-effective; toothpaste with fluoride is close to an ideal public health method that is convenient, inexpensive, culturally approved and widespread (Burt 2008) and improved brushing skills can spill over to siblings and relatives. Moreover, it has been shown that a favourable oral health behaviour established early in life is stable through the preschool years (Wigen and Wang 2014). The rational to analyse the tooth brushing behaviour in relation to the mode of delivery was our recent finding that the 5-year-olds delivered with caesarean section displayed a 2-time elevated risk of having caries (Boustedt et al. 2018). We found, however, no significant differences in the tooth brushing habits that could help to explain the elevated caries prevalence compared to those that were delivered vaginally.
The prevalence of caries in this cohort was low from an international perspective with a mean dmft value of 0.44 (SD 1.20). It is, however, likely that the true prevalence was somewhat underestimated as bite-wing radiographs were used on individual indications only when caries was suspected. Most importantly, preschool children with manifest caries in their primary dentition display an increased risk to develop caries in the permanent dentition (Mejàre et al. 2014). Thus, preventive measures should be intensified prior to the eruption of the first permanent molar and the present study highlights the importance of emphasizing twice daily assisted brushing with fluoride toothpaste. In particular, problems to perform brushing must be addressed in a systematic and practical way. We believe that an improved brushing behaviour is achievable in most families with preschool children and clearly a less demanding behaviour change than sugar reduction. This does not mean that diet counselling should be overlooked but may be delivered as a second step when optimal tooth brushing with fluoride toothpaste, based on high quality evidence, is secured.
In conclusion, this prospective study showed that caries prevalence at 5 years was significantly related to tooth brushing less than twice daily during the preschool years as well as to difficulties to perform the procedure. Health professionals should, therefore, give special attention and assist parents to improve and optimize their tooth brushing behaviour during the preschool years.
References
Boustedt K, Roswall J, Twetman S, Dahlgren J. Influence of mode of delivery, family and nursing determinants on early childhood caries development: a prospective cohort study. Acta Odontol Scand. 2018;28:1–5.
Burt BA. Prevention policies in the light of the changed distribution of dental caries. Acta Odontol Scand. 2008;195:7–63.
dos Santos AP, Nadanovsky P, de Oliveira BH. A systematic review and meta-analysis of the effects of fluoride toothpastes on the prevention of dental caries in the primary dentition of preschool children. Commun Dent Oral Epidemiol. 2013;41:1–12.
Hujoel PP, Hujoel MLA, Kotsakis GA. Personal oral hygiene and dental caries: a systematic review of randomised controlled trials. Gerodontology. 2018;35(4):282–9.
Kumar S, Tadakamadla J, Johnson NW. Effect of toothbrushing frequency on incidence and increment of dental caries: a systematic review and meta-analysis. J Dent Res. 2016;95:1230–6.
Marinho VC. Cochrane reviews of randomized trials of fluoride therapies for preventing dental caries. Eur Arch Paediatr Dent. 2009;10:183–91.
Mejàre I, Axelsson S, Dahlén G, Espelid I, Norlund A, Tranæus S, Twetman S. Caries risk assessment. A systematic review. Acta Odontol Scand. 2014;72:81–91.
Mejàre IA, Klingberg G, Mowafi FK, Stecksén-Blicks C, Twetman SH, Tranæus SH. A systematic map of systematic reviews in pediatric dentistry–what do we really know? PLoS One. 2015;10(2):e0117537.
Pitts NB, Zero DT, Marsh PD, Ekstrand K, Weintraub JA, Ramos-Gomez F, Tagami J, Twetman S, Tsakos G, Ismail A. Dental caries. Nat Rev Dis Primers. 2017;3:17030.
Roswall J, Almqvist-Tangen G, Holmén A, Alm B, Bergman S, Dahlgren J, et al. Overweight at four years of age in a Swedish birth cohort: influence of neighbourhood-level purchasing power. BMC Public Health. 2016;16:546.
Santos AP, Oliveira BH, Nadanovsky P. Effects of low and standard fluoride toothpastes on caries and fluorosis: systematic review and meta-analysis. Caries Res. 2013;47:382–90.
Twetman S. Prevention of dental caries as a non-communicable disease. Eur J Oral Sci. 2018;126(Suppl 1):19–25.
Twetman S, Dhar V. Evidence of effectiveness of current therapies to prevent and treat early childhood caries. Pediatr Dent. 2015;37:246–53.
Wigen TI, Wang NJ. Tooth brushing frequency and use of fluoride lozenges in children from 1.5 to 5 years of age: a longitudinal study. Commun Dent Oral Epidemiol. 2014;42:395–403.
Wigen TI, Wang NJ. Does early establishment of favorable oral health behavior influence caries experience at age 5 years? Acta Odontol Scand. 2015;73:182–7.
Wigen TI, Wang NJ. Referral of young children to dental personnel by primary care nurses. Int J Dent Hyg. 2017;15(3):249–55.
Wigen TI, Baumgartner CS, Wang NJ. Identification of caries risk in 2-year-olds. Commun Dent Oral Epidemiol. 2018;46:297–302.
World Health Organization. Oral health surveys: basic methods. 5th ed. Geneva: World Health Organization; 2013.
Acknowledgements
Open access funding provided by University of Gothenburg. All parents and their children are thanked for their kind willingness to invest time and take part in the present project.
Funding
The project was funded by Grants from Region Halland, Sweden.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
No conflicts of interest were reported by the authors.
Ethical approval
The study was approved by the Regional Ethical Review Board in Lund.
Informed consent
Written informed consent was obtained from the custodians.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Boustedt, K., Dahlgren, J., Twetman, S. et al. Tooth brushing habits and prevalence of early childhood caries: a prospective cohort study. Eur Arch Paediatr Dent 21, 155–159 (2020). https://doi.org/10.1007/s40368-019-00463-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40368-019-00463-3