
Abstract
Background
Cytomegalovirus (CMV) infection is a frequent event in patients undergoing allogeneic haematopoietic cell transplantation (HCT) and is associated with increased morbidity and mortality due to eventual progress to end-organ disease. Letermovir prophylaxis for CMV infections has become a standard of care in adult HCT recipients due to its efficacy and high tolerability. However, it is not yet approved for paediatric patients.
Objective
In a retrospective single-centre observational study we evaluated the use of letermovir for prophylaxis or pre-emptive treatment of cytomegalovirus (CMV) infection in seropositive paediatric HCT recipients receiving the compound outside of clinical trials. The primary endpoint was CMV reactivation requiring a change of medication.
Methods
A total of 17 patients (seven female/ten male; median age 12.2 [range 3.5–19] years, median body weight 39.5 [range 15–63] kg; median follow-up time 463.7 [range 41–1022] days) were identified who were started on oral (14) or intravenous (3) followed by oral (2) letermovir shortly after neutrophil engraftment at doses determined on the basis of age, weight, and concomitant cyclosporine use.
Results
Five patients had no evidence of viral replication (prophylactic use), while 12 patients had varying extents of viral replication (pre-emptive therapy). A change of therapy was required in one patient due to a sustained increase in CMV viral load, and in two patients, letermovir was stopped without later reactivation after initiation of palliative care for recurrent leukaemia. Of the 14 patients who completed treatment, 3 had evidence of transient viral replication after end of treatment that required no further antiviral treatment. No patients (of 17) discontinued letermovir due to an adverse event.
Conclusion
Letermovir was effective in controlling CMV infection in seropositive paediatric allogeneic HCT recipients and was overall well tolerated. Pending completion of the still ongoing paediatric investigation plans, letermovir will be an important adjunct to our options for control of infectious complications in this special population.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Letermovir was effective in controlling CMV infection in seropositive paediatric HCT recipients. |
Letermovir was well tolerated in paediatric patients. |
1 Introduction
Cytomegalovirus (CMV) infection with evidence of viral replication in blood by polymerase chain reaction (PCR) assays is a frequent event in patients undergoing allogeneic hematopoietic cell transplantation (HCT) [1, 2]. It is associated with increased morbidity and mortality due to eventual progress to end-organ disease, including chorioretinitis, pneumonia, and gastrointestinal disease [3,4,5,6,7]. Cytomegalovirus-seropositivity of the recipient and/or the donor is the most important risk factor for CMV infection in adults [8, 9] and is similarly associated with increased CMV infection rates in paediatric patients [7, 10].
Letermovir is an antiviral compound targeting the viral terminase complex of the cytomegalovirus [11]. Randomised controlled clinical trials in adults have demonstrated that letermovir is well tolerated and significantly reduces CMV infection and mortality in high-risk allogeneic HCT recipients receiving the compound in prophylactic intent when started within 28 days after transplant [12,13,14]. Since FDA approval for prophylaxis against CMV infections in CMV-seropositive adult HCT recipients in 2017, letermovir prophylaxis has become a standard of care in adult allogeneic HCT recipients who are seropositive and/or have a seropositive donor [13, 15]. Additionally, there is an increased interest in using letermovir in off-label indications, including prophylaxis of CMV-reactivation or pre-emptive therapy in paediatric patients [16]. Pre-emptive treatment with ganciclovir, foscavir or cidofovir has long been the therapy of choice for paediatric patients with CMV infection, but is associated with critically unfavourable and treatment-limiting safety profiles [17]. Therefore, there is an urgent need for the investigation of safer CMV-directed antiviral agents in paediatric patients.
A Phase IIb dose-finding study for prophylactic letermovir use in children and adolescents is ongoing but has not yet been completed or published (NCT03940586) [18]. In this single-centre retrospective study, we assess the effectiveness, safety and tolerance of prophylactic and pre-emptive off-label use of letermovir in paediatric allogeneic HCT patients who were at increased risk of CMV-infection and disease and who were not included in the ongoing clinical trial.
2 Patients and Methods
The study was a single-centre, retrospective, observational cohort study including all CMV-seropositive children, adolescents and young adults aged < 20 years who underwent allogeneic HCT between July 2019 and March 2022 and received letermovir and were not included in the ongoing dose-finding trial of the manufacturer. During that period, a total of 72 children and young adults received allogeneic HCT at our centre, 38 of whom were CMV-seropositive. Written informed consent for off-label drug use, data collection and analysis was obtained within the consent procedure for cancer treatment, HCT and specialised medical care approved by the local institutional review board.
The Centre for Bone Marrow Transplantation of the Department of Paediatric Haematology and Oncology of the University Children’s Hospital of Muenster is one of the largest paediatric transplant centres in Germany with 25 to 30 allogeneic transplantations per year for standard indications in malignant and non-malignant conditions without restrictions as to the underlying condition [19]. Conditioning regimens follow the recommendations of the relevant registries and study groups [20, 21] with post-transplant immunosuppression consisting of methotrexate and cyclosporine A in the vast majority of patients, and management of acute or chronic graft-vs-host disease (GVHD) follows the recommendations of the European Society for Blood and Marrow Transplantation (EBMT [22]). Therapeutic drug monitoring is regularly performed for cyclosporine, tacrolimus and sirolimus, and for voriconazole and posaconazole if used. Prior to transplant, both recipient and donor are screened for CMV by CMV immunoassays (Elecsys® CMV IgG and IgM, cobas® e 801 system, Roche, Basel, Switzerland) and polymerase-chain reaction (PCR) investigations (artus CMV QS-RGQ Kit; QIAsymphony RGQ System, Qiagen, Hilden, Germany). Post-transplant, quantitative PCR investigations are performed once weekly, and twice weekly once CMV replication is detected. The centre is accredited by the Joint Accreditation Committee of the International Society for Cellular Therapies and the European Society for Blood and Marrow Transplantation [23].
Letermovir was commenced as prophylaxis in PCR-negative patients or as (per definition) pre-emptive therapy in asymptomatic PCR-positive patients at viral copy thresholds left to the discretion of the responsible attending physician. Dosing was based on age, body weight, and use of cyclosporine and in accordance with the preliminary dosing scheme of the ongoing paediatric dose-finding trial [18]. Patients weighing > 30 kg received adult doses of 480 mg letermovir (orally), patients weighing < 30 kg and > 18 kg received 50% reduced adult doses of letermovir (240 mg), and patients weighing < 18 kg received 25% of the adult dose (120 mg). In patients receiving concomitant cyclosporine (but not tacrolimus or sirolimus), letermovir doses were reduced by 50% in each weight cohort. Intravenous doses of letermovir were similar to oral doses, except for patients aged < 12 years and > 30 kg who received 120 mg letermovir (with and without concomitant cyclosporine). Letermovir was continued until discontinuation of immunosuppression and stable recovery of the CD4+ lymphocyte count to at least 200 cells/µL in patients with successful suppression of viral replication, and prematurely discontinued in patients with either lack of response as measured by increasing viral replication without predefined threshold and/or signs of CMV disease, or occurrence of adverse events attributed to letermovir at the discretion of the responsible attending physician.
For analysis, the following characteristics were obtained in each patient: sex, age and weight at the time of transplant, underlying disease, CMV serostatus of donor and recipient, type of donor and transplant, day of neutrophil engraftment, CD4+ lymphocyte counts around Day +50, +100, +180, and +360 post-transplant, occurrence and treatment with steroids of GVHD, and duration of follow up. Start and duration of letermovir treatment and reason for stop of treatment; CMV replication in blood at the start of treatment, while on treatment, and at the end of treatment; occurrence of CMV-disease and reactivation of CMV after discontinuation of letermovir treatment; and adverse events attributed to letermovir were also recorded.
The primary endpoint of the descriptive analysis was defined as increases in CMV-copies/CMV-replication (reactivation) during letermovir treatment that prompted a change of antiviral medication. Adverse events resulting in discontinuation of letermovir; the impact of GVHD treatment on CMV replication under letermovir; and the occurrence of CMV-reactivation and -disease after elective discontinuation of letermovir were secondary endpoints of the study.
3 Results
A total of 17 patients (seven girls / ten boys; median [3.5–19 y] age 12.2 years, median [15–63 kg] body weight 39.5 kg) were identified who received letermovir post-transplant due to their high predicted risk to develop CMV infection and disease as assessed by the individual CMV serostatus constellation of donor and recipient (positive/negative, n = 11; and positive/positive, n = 6). The relevant patient demographics are summarised in Table 1. Nine of the patients underwent allogeneic HCT for high-risk acute leukaemia or non-Hodgkin’s lymphoma, and eight for either bone marrow failure syndrome or inherited haemoglobin disorders. The majority of patients received bone marrow from a matched related or unrelated donor with post-transplant immunosuppression with methotrexate and cyclosporine A. Neutrophil engraftment occurred between Day +11 and +26, and six patients developed transient grade I or II GVHD controlled successfully with systemic steroids (Table 1).
Details of treatment with letermovir of the 17 patients are listed in Table 2. A diagram of the descriptive results is depicted in Fig. 2. In most of the patients (n = 13), letermovir was started post-neutrophil engraftment at a median of 27.8 days post-transplant. Five patients had no evidence of viral replication, while 12 patients had varying extents of viral replication. Letermovir was administered orally in 14 patients, intravenously in one patient, and intravenously followed by oral administration in the remaining two patients at doses selected on the basis of age, weight, and concomitant cyclosporine use.
In one of the patients (pt. 13), letermovir was prematurely discontinued on Day 10 of treatment due to a sustained increase in the viral load and antiviral therapy was changed to ganciclovir; resistance testing was initiated with inconclusive results due to technical problems with the assay. In two patients (pts 5 and 14), letermovir was stopped without later reactivation on Days 107 and 10 of treatment, respectively, due to recurrent disease and initiation of palliative care. The remaining 14 patients (pts. 1–4, 6–13 and 15–17) received letermovir until recovery of the CD4+ lymphocyte count to >200 cells/µL and durable absence of viral replication, for a median duration of 139.7 days (Table 2). On average, a CD4+ lymphocyte count above 200 cells/µL was reached at Day +180 post-HCT, with a median CD4+ count of 352.3 cell/µL [81–1056 cells/µL].
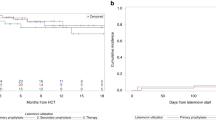
Figure 1 depicts the course over time of the CMV viral load in plasma in the 17 patients receiving letermovir. In the five patients who were started without prior evidence of replication, only one patient had transient increases in the viral load up to a maximum of 1498 IU/mL. At end of treatment, all of the five patients had no detectable viral load (Fig. 1a). Of the 12 patients with evidence for CMV replication at start of treatment, eight patients experienced a transient increase in CMV-viral load. Ten of the 12 patients had an undetectable viral load at the end of letermovir treatment; one patient was changed to ganciclovir due to absent response to letermovir, and in one patient, letermovir was discontinued due to lymphoma relapse and palliative care (Fig. 1b). Of note, of the six patients who developed grade I/II GVHD and received short-term steroid treatment, three had a transient increase in the viral load to a maximum of 1040, 940 and 1498, IU/mL, respectively, and one had an increase to up to 366,000 IU/mL in the course of 10 days.

Course of CMV viral load in plasma over time in 17 patients receiving letermovir between July 2019 and March 2022 off-label for prophylaxis or pre-emptive treatment. In each plot, CMV viral replication at transplant day ± 5 days, at the start of letermovir treatment, at the end of letermovir treatment and in between, the maximum observed value while on letermovir therapy with letermovir is depicted. Each line represents one individual patient. (a) CMV viral load in plasma in IU/mL over time in five patients with no evidence of viral replication at the time of start of treatment. * Patient (5) died before end of treatment. (b) CMV viral load in plasma in IU/mL over time in 12 patients with evidence of viral replication at the time of start of treatment. * Patient (14) died before end of treatment. ∆ Patient (13) was changed to ganciclovir treatment. CMV cytomegalovirus, LTV letermovir
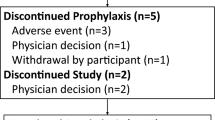
There was no discontinuation of letermovir due to an adverse event in the 17 patients, and no patient developed CMV disease. Of the 14 patients who completed treatment, after a median follow-up time of 362.6 days after discontinuation, three had evidence of transient viral replication after the end of letermovir treatment that was followed clinically and did not require further antiviral treatment (Fig. 2, Table 2).

Diagram depicting the descriptive results concerning viral replication status and LTV treatment status. CMV cytomegalovirus, LTV letermovir
4 Discussion
In this single-centre, retrospective, observational cohort study including all paediatric patients at high risk for CMV reactivation who received letermovir outside of the ongoing dose-finding trial as primary prophylaxis (n = 5) or early pre-emptive therapy (n = 12), letermovir was discontinued prematurely due to a persistently high viral load in one patient who was salvaged with ganciclovir and in two further patients who were transitioned to palliative care for recurrent disease. In 14 patients who completed treatment, transient reactivations after the end of treatment without need for intervention occurred in three patients. Letermovir was overall well-tolerated, and no patients developed treatment-limiting adverse events.
Transient increases in the CMV viral load in plasma were not infrequent while on treatment with letermovir and were observed in 5 of 11 patients (45%) without and in 3 of 6 patients (50%) with acute GVHD receiving steroid treatment. While the occurrence of GVHD is a well-described risk factor for the development of CMV reactivation [13, 24,25,26,27], the latter appeared not to have been influenced by the presence of GVHD during letermovir exposure. Supporting the efficacy of letermovir in our study, no breakthrough CMV infections were reported by others in children with off-label prophylactic letermovir treatment [16, 27]. Styczynski et al, in an EBMT-initiated multicentre, retrospective observational study, reported an incidence of CMV breakthrough infections in patients (adults and children) with letermovir prophylaxis of approximately 10% [16]. However, transient increases in the CMV viral load were not captured in that study. Most patients included in this study (70%) received letermovir per definition as pre-emptive treatment following documented CMV reactivation, and most responded very well to letermovir treatment. There are only few reports for letermovir pre-emptive therapy or secondary prophylaxis in children, which show, however, overall high viral clearance rates [16, 28, 29]. In adult patients, a Phase 2a study was conducted for pre-emptive letermovir treatment in kidney transplant recipients [30] and experiences with letermovir secondary prophylaxis in HSCT recipients have been previously published [16, 31]. However, at the time of the writing of this article, letermovir is approved for prophylaxis of CMV reactivation only [13, 16] and approval of this indication in paediatric patients is pending until completion of the ongoing paediatric dose-finding trial.
We found that letermovir was overall very well tolerated: there were no treatment discontinuations due to adverse events thought to be related to letermovir treatment. This observation is in line with previous reports of letermovir use in paediatric patients, where letermovir provoked common adverse events such as nausea and vomiting [16, 27] or mild liver function impairment [27, 29] but did not result in letermovir discontinuation. With a median treatment duration of 132.6 days, even long-term use of letermovir was well tolerated in our cohort. In one patient, letermovir had to be discontinued due to absent response to letermovir pre-emptive therapy. While resistance testing in our patient was prompted but was unsuccessful due to technical problems with the assay, resistance to letermovir has been linked to mutations in a gene for the viral terminase subunit (UL56) that does not affect susceptibility to ganciclovir treatment [32, 33]. In line with these findings, breakthrough CMV-viremia in our patient could be cleared with ganciclovir treatment.
A limitation of our study is the lack of a comparator group receiving alternative CMV prophylaxis or pre-emptive treatment. Therefore, no statistical analyses regarding efficacy and safety can be derived from the study. To date, there are limited reports of letermovir use in children [16, 27,28,29, 34, 35] with overall very small sample sizes, underlining the need for more analysis of letermovir prophylaxis or pre-emptive treatment in children.
5 conclusions
In conclusion, the results of this necessarily limited analysis suggest that letermovir is well tolerated even for long-term use and effective in CMV prophylaxis and pre-emptive treatment in paediatric patients with high-risk CMV constellations undergoing allogeneic HCT. The demonstration of effective prevention of CMV infection and disease without haematological or renal adverse events with letermovir [13] is a breakthrough in infectious disease supportive care in allogeneic HCT recipients, which needs to be made available to children and adolescents by appropriate dose-findings studies. In addition, further studies are required to investigate the role of letermovir for pre-emptive treatment of CMV infections.
Change history
08 February 2023
Missing Open Access funding information has been added in the Funding Note
References
Ljungman P, de la Camara R, Robin C, Crocchiolo R, Einsele H, Hill JA, Hubacek P, Navarro D, Cordonnier C, Ward KN. Guidelines for the management of cytomegalovirus infection in patients with haematological malignancies and after stem cell transplantation from the 2017 European Conference on Infections in Leukaemia (ECIL 7). Lancet Infect Dis. 2019;19:e260–72. https://doi.org/10.1016/s1473-3099(19)30107-0.
Solano C, Vázquez L, Giménez E, de la Cámara R, Albert E, Rovira M, Espigado I, Calvo CM, López-Jiménez J, Suárez-Lledó M, et al. Cytomegalovirus DNAemia and risk of mortality in allogeneic hematopoietic stem cell transplantation: analysis from the Spanish hematopoietic transplantation and cell therapy group. Am J Transplant. 2021;21:258–71. https://doi.org/10.1111/ajt.16147.
Teira P, Battiwalla M, Ramanathan M, Barrett AJ, Ahn KW, Chen M, Green JS, Saad A, Antin JH, Savani BN, et al. Early cytomegalovirus reactivation remains associated with increased transplant-related mortality in the current era: a CIBMTR analysis. Blood. 2016;127:2427–38. https://doi.org/10.1182/blood-2015-11-679639.
Jang JE, Hyun SY, Kim YD, Yoon SH, Hwang DY, Kim SJ, Kim Y, Kim JS, Cheong JW, Min YH. Risk factors for progression from cytomegalovirus viremia to cytomegalovirus disease after allogeneic hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2012;18:881–6. https://doi.org/10.1016/j.bbmt.2011.10.037.
Green ML, Leisenring W, Xie H, Mast TC, Cui Y, Sandmaier BM, Sorror ML, Goyal S, Özkök S, Yi J, et al. Cytomegalovirus viral load and mortality after haemopoietic stem cell transplantation in the era of pre-emptive therapy: a retrospective cohort study. Lancet Haematol. 2016;3:e119-127. https://doi.org/10.1016/s2352-3026(15)00289-6.
Ariza-Heredia EJ, Nesher L, Chemaly RF. Cytomegalovirus diseases after hematopoietic stem cell transplantation: a mini-review. Cancer Lett. 2014;342:1–8. https://doi.org/10.1016/j.canlet.2013.09.004.
Zöllner SK, Herbrüggen H, Kolve H, Mihailovic N, Schubert F, Reicherts C, Rössig C, Groll AH. Cytomegalovirus retinitis in children and adolescents with acute leukemia following allogeneic hematopoietic stem cell transplantation. Transpl Infect Dis. 2019;21: e13089. https://doi.org/10.1111/tid.13089.
George B, Pati N, Gilroy N, Ratnamohan M, Huang G, Kerridge I, Hertzberg M, Gottlieb D, Bradstock K. Pre-transplant cytomegalovirus (CMV) serostatus remains the most important determinant of CMV reactivation after allogeneic hematopoietic stem cell transplantation in the era of surveillance and pre-emptive therapy. Transpl Infect Dis. 2010;12:322–9. https://doi.org/10.1111/j.1399-3062.2010.00504.x.
Schmidt-Hieber M, Tridello G, Ljungman P, Mikulska M, Knelange N, Blaise D, Socié G, Volin L, Blijlevens N, Fegueux N, et al. The prognostic impact of the cytomegalovirus serostatus in patients with chronic hematological malignancies after allogeneic hematopoietic stem cell transplantation: a report from the Infectious Diseases Working Party of EBMT. Ann Hematol. 2019;98:1755–63. https://doi.org/10.1007/s00277-019-03669-z.
Heston SM, Young RR, Tanaka JS, Jenkins K, Vinesett R, Saccoccio FM, Martin PL, Chao NJ, Kelly MS. Risk factors for CMV viremia and treatment-associated adverse events among pediatric hematopoietic stem cell transplant recipients. Open Forum Infect Dis. 2022;9:639. https://doi.org/10.1093/ofid/ofab639.
Goldner T, Hewlett G, Ettischer N, Ruebsamen-Schaeff H, Zimmermann H, Lischka P. The novel anticytomegalovirus compound AIC246 (Letermovir) inhibits human cytomegalovirus replication through a specific antiviral mechanism that involves the viral terminase. J Virol. 2011;85:10884–93. https://doi.org/10.1128/jvi.05265-11.
Ljungman P, Schmitt M, Marty FM, Maertens J, Chemaly RF, Kartsonis NA, Butterton JR, Wan H, Teal VL, Sarratt K, et al. A mortality analysis of letermovir prophylaxis for cytomegalovirus (CMV) in CMV-seropositive recipients of allogeneic hematopoietic cell transplantation. Clin Infect Dis. 2020;70:1525–33. https://doi.org/10.1093/cid/ciz490.
Marty FM, Ljungman P, Chemaly RF, Maertens J, Dadwal SS, Duarte RF, Haider S, Ullmann AJ, Katayama Y, Brown J, et al. Letermovir prophylaxis for cytomegalovirus in hematopoietic-cell transplantation. N Engl J Med. 2017;377:2433–44. https://doi.org/10.1056/NEJMoa1706640.
Marty FM, Ljungman PT, Chemaly RF, Wan H, Teal VL, Butterton JR, Yeh WW, Leavitt RY, Badshah CS. Outcomes of patients with detectable CMV DNA at randomization in the phase III trial of letermovir for the prevention of CMV infection in allogeneic hematopoietic cell transplantation. Am J Transplant. 2020;20:1703–11. https://doi.org/10.1111/ajt.15764.
Jakharia N, Howard D, Riedel DJ. CMV infection in hematopoietic stem cell transplantation: prevention and treatment strategies. Curr Treat Options Infect Dis. 2021;13:123–40. https://doi.org/10.1007/s40506-021-00253-w.
Styczynski J, Tridello G, Xhaard A, Medinger M, Mielke S, Taskinen M, Blijlevens N, Rodriguez MAB, Solano C, Nikolousis E, et al. Use of letermovir in off-label indications: infectious diseases working party of European society of blood and marrow transplantation retrospective study. Bone Marrow Transplant. 2021;56:1171–9. https://doi.org/10.1038/s41409-020-01166-w.
Wattles BA, Kim AJ, Cheerva AC, Lucas KG, Elder JJ. Cytomegalovirus treatment in pediatric hematopoietic stem cell transplant patients. J Pediatr Hematol Oncol. 2017;39:241–8. https://doi.org/10.1097/mph.0000000000000730.
Merck Sharp & Dohme LLC: Letermovir treatment in pediatric participants following allogeneic haematopoietic stem cell transplantation (HSCT) (MK-8228-030). Availabe online: https://clinicaltrials.gov/ct2/show/NCT****03940586?term=NCT****03940586&draw=2&rank=1 (accessed on 03/11/2022).
Medizinische Klinik A / Klinik für Kinder- und Jugendmedizin - Pädiatrische Hämatologie und Onkologie: UKM Knochenmarktransplantationszentrum. Availabe online: https://www.ukm.de/zentren/knochenmarktransplantationszentrum (accessed on 2022/08/27).
Reinken K., GrünEberg I.: Kinderkrebsinfo. Availabe online: https://www.gpoh.de/kinderkrebsinfo/content/diseases/index_eng.html (accessed on 03/11/2022).
Dobke J., Grüneberg I.. Kinderblutkrankheiten. Availabe online: https://www.kinderblutkrankheiten.de (accessed on 03/11/2022).
The EBMT Handbook: Hematopoietic Stem Cell Transplantation and Cellular Therapies [Internet]. 7th edition., 7th ed.; Enric Carreras, C.D., Mohamad Mohty, Nicolaus Kröger, Ed. Springer Nature, pp. 702. https://doi.org/10.1007/978-3-030-02278-5.
Joint Accreditation Committee of the International Society for Cell & Gene Therapies; JACIE. Availabe online: https://www.ebmt.org/jacie-accreditation (accessed on 2022/10/27).
Meyers JD, Flournoy N, Thomas ED. Risk factors for cytomegalovirus infection after human marrow transplantation. J Infect Dis. 1986;153:478–88. https://doi.org/10.1093/infdis/153.3.478.
Jaing TH, Chang TY, Chen SH, Wen YC, Yu TJ, Lee CF, Yang CP, Tsay PK. Factors associated with cytomegalovirus infection in children undergoing allogeneic hematopoietic stem-cell transplantation. Medicine (Baltimore). 2019;98: e14172. https://doi.org/10.1097/md.0000000000014172.
Marty FM, Bryar J, Browne SK, Schwarzberg T, Ho VT, Bassett IV, Koreth J, Alyea EP, Soiffer RJ, Cutler CS, et al. Sirolimus-based graft-versus-host disease prophylaxis protects against cytomegalovirus reactivation after allogeneic hematopoietic stem cell transplantation: a cohort analysis. Blood. 2007;110:490–500. https://doi.org/10.1182/blood-2007-01-069294.
Cheng CN, Li SS, Yeh YH, Shen CF, Chen JS. Letermovir prophylaxis for cytomegalovirus reactivation in children who underwent hematopoietic stem cell transplantation: a single-institute experience in Taiwan. J Microbiol Immunol Infect. 2022. https://doi.org/10.1016/j.jmii.2022.01.002.
Chiereghin A, Belotti T, Borgatti EC, Fraccascia N, Piccirilli G, Fois M, Borghi M, Turello G, Gabrielli L, Masetti R, et al. Off-label use of letermovir as pre-emptive anti-cytomegalovirus therapy in a pediatric allogeneic peripheral blood stem cell transplant. Infect Drug Resist. 2021;14:1185–90. https://doi.org/10.2147/idr.S296927.
Strenger V, Sperl D, Kubesch K, Donnerer J, Schwinger W, Zach K, Lackner H, Benesch M. Letermovir in paediatric HSCT recipients. J Antimicrob Chemother. 2019;74:2820–1. https://doi.org/10.1093/jac/dkz218.
Stoelben S, Arns W, Renders L, Hummel J, Mühlfeld A, Stangl M, Fischereder M, Gwinner W, Suwelack B, Witzke O, et al. Pre-emptive treatment of Cytomegalovirus infection in kidney transplant recipients with letermovir: results of a Phase 2a study. Transpl Int. 2014;27:77–86. https://doi.org/10.1111/tri.12225.
Lin A, Maloy M, Su Y, Bhatt V, DeRespiris L, Griffin M, Lau C, Proli A, Barker J, Shaffer B, et al. Letermovir for primary and secondary cytomegalovirus prevention in allogeneic hematopoietic cell transplant recipients: real-world experience. Transpl Infect Dis. 2019;21: e13187. https://doi.org/10.1111/tid.13187.
Chou S. Rapid in vitro evolution of human cytomegalovirus UL56 mutations that confer letermovir resistance. Antimicrob Agents Chemother. 2015;59:6588–93. https://doi.org/10.1128/aac.01623-15.
Lischka P, Michel D, Zimmermann H. Characterization of cytomegalovirus breakthrough events in a phase 2 prophylaxis trial of letermovir (AIC246, MK 8228). J Infect Dis. 2016;213:23–30. https://doi.org/10.1093/infdis/jiv352.
Kilgore JT, Becken B, Varga MG, Parikh S, Prasad V, Lugo D, Chang YC. Use of letermovir for salvage therapy for resistant cytomegalovirus in a pediatric hematopoietic stem cell transplant recipient. J Pediatr Infect Dis Soc. 2020;9:486–9. https://doi.org/10.1093/jpids/piz050.
Pérez Marín M, Decosterd LA, Andre P, Buclin T, Mercier T, Murray K, Rizzi M, Meylan P, Jaton-Ogay K, Opota O, et al. Compassionate use of letermovir in a 2-year-old immunocompromised child with resistant cytomegalovirus disease. J Pediatric Infect Dis Soc. 2020;9:96–9. https://doi.org/10.1093/jpids/piz033.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Financial support
Open Access funding enabled and organized by Projekt DEAL.
Conflicts of interest
AHG has received grants from Gilead, Merck, Sharp & Dohme and Pfizer and has served as consultant to Amplyx, Astellas, Basilea, F2G, Gilead. Merck, Sharp & Dohme, Pfizer, Scynexis, and Mundipharma. KFK, MAF, MTH, MH, SAH, MA, HT and BB have no conflicts to declare.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Consent to participate
Written informed consent for off label drug use, data collection and analysis was obtained within the consent procedure for cancer treatment, HCT and specialized medical care approved by the local institutional review board. Informed consent to be included in this analysis was waived as the study did not involve additional procedures to the standardized clinical protocols and all data were treated in an anonymous fashion.
Consent for publication
All authors give the publisher the permission to publish the work.
Subjects signed informed consent
Not applicable.
Data availability statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Code availability
Not applicable.
Author contribution statement
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Miriam A. Füller, Katharina F. Körholz, and Marc Hennies. Malcolm Holterhus, Susanne Hagedorn, Martina Ahlmann, Heike Thorer and Birgit Burkhardt were in charge of patients treatment and patient data collection. The first draft of the manuscript was written by Katharina F. Körholz and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Körholz, K.F., Füller, M.A., Hennies, M. et al. Letermovir for Prophylaxis and Pre-emptive Therapy of Cytomegalovirus Infection in Paediatric Allogeneic Haematopoietic Cell Transplant Patients. Pediatr Drugs 25, 225–232 (2023). https://doi.org/10.1007/s40272-022-00547-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40272-022-00547-6