
Abstract
Background
Relapsing–remitting multiple sclerosis (RRMS) is an incurable disease characterised by relapses (periods of function loss) followed by full or partial recovery, and potential permanent disability over time. Many disease-modifying treatments (DMTs) exist that help reduce relapses and slow disease progression. Most are contraindicated during conception/pregnancy and some require a discontinuation period before trying to conceive. Although around three-quarters of people with RRMS are women, there is limited knowledge about how reproductive issues impact DMT preference.
Objective
The aim of this study was to measure the preferences for DMTs of women with RRMS who are considering pregnancy.
Design
An online discrete choice experiment (DCE).
Methods
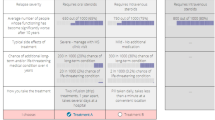
Participants chose between two hypothetical DMTs characterised by a set of attributes, then indicated if they preferred their choice to no treatment. Attributes were identified from interviews and focus groups with people with RRMS and MS professionals, as well as literature reviews, and included the probability of problems with pregnancy, discontinuation of DMTs, and breastfeeding safety. In each DCE task, participants were asked to imagine making decisions in three scenarios: now; when trying to conceive; and when pregnant.
Analysis
Two mixed logit models were estimated, one to assess the statistical significance between scenarios and one in maximum acceptable risk space to allow comparison of the magnitudes of parameters between scenarios.
Sample
Women with RRMS who were considering having a child in the future, recruited from a UK MS patient register.
Results
Sixty respondents completed the survey. Participants preferred no treatment in 12.6% of choices in the ‘now’ scenario, rising significantly to 37.6% in the ‘trying to conceive’ scenario and 60.3% in the ‘pregnant’ scenario (Kruskal–Wallis p < 0.001). This pattern corresponds with results from models that included a no-treatment alternative-specific constant (ASC) capturing differences between taking and not taking a DMT not specified by the attributes. The ASC was lower in the trying to conceive scenario than in the now scenario, and lower still in the pregnant scenario, indicating an intrinsic preference for no treatment. Participants also placed relatively less preference on reducing relapses and avoiding disease progression in the trying to conceive and pregnant scenarios compared with a lower risk of problems with pregnancy. In the trying to conceive scenario, participants’ preference for treatments with shorter washout periods increased.
Conclusion
Women with RRMS considering having a child prefer DMTs with more favourable reproduction-related attributes, even when not trying to conceive. Reproductive issues also influenced preferences for DMT attributes not directly related to pregnancy, with preferences dependent on the life circumstances in which choices were made. The design of the DCE highlights the benefits of considering the scenario in which participants make choices, as they may change over time.



Similar content being viewed by others


Data Availability Statement
Data are not publicly available as consent was not obtained from participants, however, data may be shared on a case-by-case basis if a formal data sharing agreement is entered into, by contacting either the corresponding author or the Leeds Institute of Health Sciences.
Notes
The two attributes were relapse severity and chance of additional long-term and/or life-threatening medical condition over 4 years.
ChoiceMetrics.
Participants who were currently trying to conceive and who were making choices in the now scenario were modelled as being in the trying to conceive scenario.
References
Reich DS, Lucchinetti CF, Calabresi PA. Multiple sclerosis. N Engl J Med. 2018;378:169–80.
Thompson AJ, Banwell BL, Barkhof F, Carroll WM, Coetzee T, Comi G, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018;17:162–73.
Bove RM, Hauser SL. Diagnosing multiple sclerosis: art and science. Lancet Neurol. 2018;17:109–11.
Wallin MT, Culpepper WJ, Nichols E, Bhutta ZA, Gebrehiwot TT, Hay SI, et al. Global, regional, and national burden of multiple sclerosis 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18:269–85.
Kingwell E, Marriott JJ, Jetté N, Pringsheim T, Makhani N, Morrow SA, et al. Incidence and prevalence of multiple sclerosis in Europe: a systematic review. BMC Neurol. 2013;13:128.
World Health Organization. Atlas: multiple sclerosis resources in the world 2008. Geneva: World Health Organization; 2008.
Brownlee WJ, Hardy TA, Fazekas F, Miller DH. Diagnosis of multiple sclerosis: progress and challenges. Lancet. 2017;389:1336–46.
Comi G, Radaelli M, Soelberg Sørensen P. Evolving concepts in the treatment of relapsing multiple sclerosis. Lancet. 2017;389:1347–56.
Castro-Borrero W, Graves D, Frohman TC, Flores AB, Hardeman P, Logan D, et al. Current and emerging therapies in multiple sclerosis: a systematic review. Ther Adv Neurol Disord. 2012;5:205–20.
Rae-Grant A, Day GS, Marrie RA, Rabinstein A, Cree BA, Gronseth GS, et al. Comprehensive systematic review summary: disease-modifying therapies for adults with multiple sclerosis: report of the guideline development, dissemination, and implementation subcommittee of the American Academy of Neurology. Neurology. 2018;90:789–800.
Torkildsen Ø, Myhr KM, Bø L. Disease-modifying treatments for multiple sclerosis: a review of approved medications. Eur J Neurol. 2016;23:18–27.
Eskyte I, Manzano A, Pepper G, Pavitt S, Ford H, Bekker H, et al. Understanding treatment decisions from the perspective of people with relapsing remitting multiple sclerosis: a critical interpretive synthesis. Mult Scler Relat Disord. 2019;27:370–7.
Coyle PK. Management of women with multiple sclerosis through pregnancy and after childbirth. Ther Adv Neurol Disord. 2016;9:198–21010.
Payne D, McPherson KM. Becoming mothers. Multiple sclerosis and motherhood: a qualitative study. Disabil Rehabil. 2010;32:629–38.
Sandberg-Wollheim M, Neudorfer O, Grinspan A, Weinstock-Guttman B, Haas J, Izquierdo G, et al. Pregnancy outcomes from the branded glatiramer acetate pregnancy database. Int J MS Care. 2018;20:9–14.
Lu E, Wang BW, Guimond C, Synnes A, Sadovnick D, Tremlett H. Disease-modifying drugs for multiple sclerosis in pregnancy: a systematic review. Neurology. 2012;79:1130–5.
Coyle PK, Sinclair S, Scheuerle A, Thorp J, Albano J, Rametta M. Final results from the Betaseron (interferon β-1b) Pregnancy Registry: a prospective observational study of birth defects and pregnancy-related adverse events. BMJ Open. 2014;4:e004536.
Fares J, Nassar AH, Gebeily S, Kobeissy F, Fares Y. Pregnancy outcomes in Lebanese women with multiple sclerosis (the LeMS study): a prospective multicentre study. BMJ Open. 2016;6:e011210.
Alroughani R, Altintas A, Al Jumah M, Sahraian M, Alsharoqi I, Al Tahan A, et al. Pregnancy and the use of disease-modifying therapies in patients with multiple sclerosis: benefits versus risks. Mult Scler Int. 2016;2016:1034912.
Dobson R, Dassan P, Roberts M, Giovannoni G, Nelson-Piercy C, Brex PA. UK consensus on pregnancy in multiple sclerosis: ‘Association of British Neurologists’ guidelines. Pract Neurol. 2019;19:106–14.
Hughes SE, Spelman T, Gray OM, Boz C, Trojano M, Lugaresi A, et al. Predictors and dynamics of postpartum relapses in women with multiple sclerosis. Mult Scler J. 2014;20:739–46.
Confavreux C, Hutchinson M, Hours MM, Cortinovis-Tourniaire P, Moreau T. Pregnancy in Multiple Sclerosis Group. Rate of pregnancy-related relapse in multiple sclerosis. N Engl J Med. 1998;339:285–91.
AL Phillips, MK Houtchens, NC Edwards. Multiple sclerosis relapse rates, before, during, and after pregnancy: a US retrospective claims database analysis (P1. 361). Neurology. 2017;88(16 Suppl).
Vukusic S, Marignier R. Multiple sclerosis and pregnancy in the'treatment era'. Nat Rev Neurol. 2015;11:280.
Langer-Gould A, Smith JB, Albers KB, Xiang AH, Wu J, Kerezsi EH, et al. Pregnancy-related relapses and breastfeeding in a contemporary multiple sclerosis cohort. Neurology. 2020;94:e1939–e19491949.
Pakenham KI, Tilling J, Cretchley J. Parenting difficulties and resources: the perspectives of parents with multiple sclerosis and their partners. Rehabil Psychol. 2012;57:52.
Kosmala-Anderson J, Wallace LM. A qualitative study of the childbearing experience of women living with multiple sclerosis. Disabil Rehabil. 2013;35:976–81.
Wundes A, Pebdani RN, Amtmann D. What do healthcare providers advise women with multiple sclerosis regarding pregnancy? Mult Scler Int. 2014;2014:819216.
Borisow N, Döring A, Pfueller CF, Paul F, Dörr J, Hellwig K. Expert recommendations to personalization of medical approaches in treatment of multiple sclerosis: an overview of family planning and pregnancy. EPMA J. 2012;3:9.
Borisow N, Paul F, Ohlraun S, Pach D, Fischer F, Dörr J. Pregnancy in multiple sclerosis: a questionnaire study. PLoS ONE. 2014;9:e99106.
Lee M, O’Brien P. Pregnancy and multiple sclerosis. J Neurol Neurosurg Psychiatry. 2008;79:1308–11.
Soekhai V, de Bekker-Grob EW, Ellis AR, Vass CM. Discrete choice experiments in health economics: past, present and future. PharmacoEconomics. 2019;37:201–26.
Clark MD, Determann D, Petrou S, Moro D, de Bekker-Grob EW. Discrete choice experiments in health economics: a review of the literature. PharmacoEconomics. 2014;32:883–902.
Webb EJ, Meads D, Eskyte I, King N, Dracup N, Chataway J, et al. A systematic review of discrete-choice experiments and conjoint analysis studies in people with multiple sclerosis. Patient. 2018;11:391–402.
Manzano A, Eskytė I, Ford HL, Bekker H, Potrata B, Chataway J, et al. Impact of communication on first treatment decisions in people with relapsing-remitting multiple sclerosis. Patient Educ Couns. 2020. https://doi.org/10.1016/j.pec.2020.05.014.
Sepucha KR, Abhyankar P, Hoffman AS, Bekker HL, LeBlanc A, Levin CA, et al. Standards for UNiversal reporting of patient Decision Aid Evaluation studies: the development of SUNDAE Checklist. BMJ Qual Saf. 2018;27:380–8.
A Manzano, HL Ford, B Potrata, I Eskyte, D Meads, E Webb, et al. Treatment Decision Making and Relapsing Remitting Multiple Sclerosis. The CRIMSON Project Decision Aid Booklet. Leeds: University of Leeds; 2019. Available at: https://crimson.leeds.ac.uk/wp-content/uploads/sites/51/2019/12/UOL169_CRIMSON-A4-Brochure_WEB.pdf.
Poulos C, Kinter E, van Beek J, Christensen K, Posner J. Preferences of patients with multiple sclerosis for attributes of injectable multiple sclerosis treatments in the United Kingdom and France. Int J Technol Assess Health Care. 2018;34:425–33.
Bottomley C, Lloyd A, Bennett G, Adlard N. A discrete choice experiment to determine UK patient preference for attributes of disease modifying treatments in Multiple Sclerosis. J Med Econ. 2017;20:863–70.
Johnson FR, Van Houtven G, Ozdemir S, Hass S, White J, Francis G, et al. Multiple sclerosis patients' benefit-risk preferences: serious adverse event risks versus treatment efficacy. J Neurol. 2009;256:554–62.
Wicks P, Brandes D, Park J, Liakhovitski D, Koudinova T, Sasane R. Preferred features of oral treatments and predictors of non-adherence: two web-based choice experiments in multiple sclerosis patients. Interact J Med Res. 2015;4:e6.
Coast J, Al-Janabi H, Sutton EJ, Horrocks SA, Vosper AJ, Swancutt DR, et al. Using qualitative methods for attribute development for discrete choice experiments: issues and recommendations. Health Econ. 2012;21:730–41.
Kløjgaard ME, Bech M, Søgaard R. Designing a stated choice experiment: the value of a qualitative process. J Choice Model. 2012;5:1–18.
Janssen EM, Segal JB, Bridges JFP. A framework for instrument development of a choice experiment: an application to type 2 diabetes. Patient. 2016;9:465–79.
Bridges JF, Hauber AB, Marshall D, Lloyd A, Prosser LA, Regier DA, et al. Conjoint analysis applications in health—a checklist: a report of the ISPOR Good Research Practices for Conjoint Analysis Task Force. Value Health. 2011;14:403–13.
Hollin IL, Craig BM, Coast J, Beusterien K, Vass C, DiSantostefano R, et al. Reporting formative qualitative research to support the development of quantitative preference study protocols and corresponding survey instruments: guidelines for authors and reviewers. Patient. 2020;13:121–36.
Trevena LJ, Zikmund-Fisher BJ, Edwards A, Gaissmaier W, Galesic M, Han PK, et al. Presenting quantitative information about decision outcomes: a risk communication primer for patient decision aid developers. BMC Med Inform Decis Mak. 2013;13:S7.
Zipkin DA, Umscheid CA, Keating NL, Allen E, Aung K, Beyth R, et al. Evidence-based risk communication: a systematic review. Ann Intern Med. 2014;161:270–80.
Lancsar E, Fiebig DG, Hole AR. Discrete choice experiments: a guide to model specification, estimation and software. Pharmacoeconomics. 2017;35:697–716.
Hess S, Rose JM. Can scale and coefficient heterogeneity be separated in random coefficients models? Transportation. 2012;39:1225–399.
Amato M, Portaccio E, Ghezzi A, Hakiki B, Zipoli V, Martinelli V, et al. Pregnancy and fetal outcomes after interferon-β exposure in multiple sclerosis. Neurology. 2010;75:1794–802.
Boskovic R, Wide R, Wolpin J, Bauer D, Koren G. The reproductive effects of beta interferon therapy in pregnancy: a longitudinal cohort. Neurology. 2005;65:807–11.
Train K, Weeks M. Discrete choice models in preference space and willingness-to-pay space. In: Scarpa R, Alberini A, editors. Applications of simulation methods in environmental and resource economics. Springer; 2005. p. 1–16.
Hole AR, Kolstad JR. Mixed logit estimation of willingness to pay distributions: a comparison of models in preference and WTP space using data from a health-related choice experiment. Empir Econ. 2012;42:445–69.
Hess S, Palma D. Apollo: a flexible, powerful and customisable freeware package for choice model estimation and application. J Choice Model. 2019;32:100170.
Garcia-Dominguez JM, Munoz D, Comellas M, Gonzalbo I, Lizan L, Polanco Sanchez C. Patient preferences for treatment of multiple sclerosis with disease-modifying therapies: a discrete choice experiment. Patient Prefer Adherence. 2016;10:1945–56.
Lynd LD, Traboulsee A, Marra CA, Mittmann N, Evans C, Li KH, et al. Quantitative analysis of multiple sclerosis patients' preferences for drug treatment: a best-worst scaling study. Ther Adv Neurol Disord. 2016;9:287–96.
Wilson LS, Loucks A, Gipson G, Zhong L, Bui C, Miller E, et al. Patient preferences for attributes of multiple sclerosis disease-modifying therapies: development and results of a ratings-based conjoint analysis. Int J MS Care. 2015;17:74–82.
Wilson L, Loucks A, Bui C, Gipson G, Zhong L, Schwartzburg A, et al. Patient centered decision making: use of conjoint analysis to determine risk-benefit trade-offs for preference sensitive treatment choices. J Neurol Sci. 2014;344:80–7.
A Manzano, HL Ford, G Pepper, J Chataway, K Schmierer, D Meads, et al. CRIMSON—Considering Risk and benefits In Multiple Sclerosis treatment selectiON. 2019.
Henshaw SK. Unintended pregnancy in the United States. Fam Plann Perspect. 1998;30(24–9):46.
Spinks J, Janda M, Soyer HP, Whitty JA. Consumer preferences for teledermoscopy screening to detect melanoma early. J Telemed Telecare. 2016;22:39–46.
Schmier JK, Halpern MT. Patient recall and recall bias of health state and health status. Expert Rev Pharmacoecon Outcomes Res. 2004;4:159–63.
Pecori C, Giannini M, Portaccio E, Ghezzi A, Hakiki B, Pastò L, et al. Paternal therapy with disease modifying drugs in multiple sclerosis and pregnancy outcomes: a prospective observational multicentric study. BMC Neurol. 2014;14:114.
Hardy JR, Leaderer BP, Holford TR, Hall GC, Bracken MB. Safety of medications prescribed before and during early pregnancy in a cohort of 81,975 mothers from the UK General Practice Research Database. Pharmacoepidemiol Drug Saf. 2006;15:555–64.
Van Den Wijngaard L, Van Wely M, Dancet EA, Van Mello NM, Koks CA, Van Der Veen F, et al. Patients' preferences for gonadotrophin-releasing hormone analogs in in vitro fertilization. Gynecol Obstetr Investig. 2014;78:16–211.
Landfeldt E, Jablonowska B, Norlander E, Persdotter-Eberg K, Thurin-Kjellberg A, Wramsby M, et al. Patient preferences for characteristics differentiating ovarian stimulation treatments. Hum Reprod. 2012;27:760–9.
van Empel IW, Dancet EA, Koolman XH, Nelen WL, Stolk EA, Sermeus W, et al. Physicians underestimate the importance of patient-centredness to patients: a discrete choice experiment in fertility care. Hum Reprod. 2011;26:584–93.
Pavlova M, Hendrix M, Nouwens E, Nijhuis J, van Merode G. The choice of obstetric care by low-risk pregnant women in the Netherlands: implications for policy and management. Health Policy. 2009;93:27–34.
Ride J, Lancsar E. Women’s preferences for treatment of perinatal depression and anxiety: a discrete choice experiment. PLoS ONE. 2016;11:e0156629.
Morgan H, Hoddinott P, Thomson G, Crossland N, Farrar S, Yi D, et al. Benefits of Incentives for Breastfeeding and Smoking cessation in pregnancy (BIBS): a mixed-methods study to inform trial design. Health Technol Assess. 2015;19:1–522, vii–viii.
Beulen L, Grutters JP, Faas BH, Feenstra I, Groenewoud H, van Vugt JM, et al. Women's and healthcare professionals' preferences for prenatal testing: a discrete choice experiment. Prenat Diagn. 2015;35:549–57.
Carroll FE, Al-Janabi H, Flynn T, Montgomery AA. Women and their partners' preferences for Down's syndrome screening tests: a discrete choice experiment. Prenat Diagn. 2013;33:449–56.
Hill M, Fisher J, Chitty LS, Morris S. Women’s and health professionals’ preferences for prenatal tests for Down syndrome: a discrete choice experiment to contrast noninvasive prenatal diagnosis with current invasive tests. Genet Med. 2012;14:905–13.
Chan YM, Sahota DS, Leung TY, Choy KW, Chan OK, Lau TK. Chinese women's preferences for prenatal diagnostic procedure and their willingness to trade between procedures. Prenat Diagn. 2009;29:1270–6.
Author information
Authors and Affiliations
Contributions
All authors conceived the study, defined the study aims and contributed to the survey design. EW and DM collected the data. EW conducted the statistical analysis and wrote the first draft of the manuscript, and all authors contributed to and approved the final version.
Corresponding author
Ethics declarations
Funding
This study was funded by the UK Multiple Sclerosis Society (grant no. 30). The research is supported by the National Institute for Health Research (NIHR) infrastructure at Leeds. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care. YO acknowledges support from a Population Research Fellowship awarded by Cancer Research UK (reference C57775/A22182). JC is supported in part by the National Institute for Health Research, University College London Hospitals, Biomedical Research Centre, London, UK.
Conflict of interest
Jeremy Chataway has received support from the Efficacy and Mechanism Evaluation Programme and Health Technology Assessment Programme (NIHR); UK Multiple Sclerosis Society and National Multiple Sclerosis Society; and the Rosetrees Trust. In the last 3 years, he has been a local principal investigator for trials in MS funded by Receptos, Novartis and Biogen Idec, and has received an investigator grant from Novartis outside this work. He has taken part in Advisory Boards/consultancy for Roche, Merck, MedDay, Biogen and Celgene. Klaus Schmierer has received consulting fees from Biogen, Merck, Novartis and Roche, and has received payments for lecturing activities from Biogen, Merck, Novartis, Roche and Teva. Hilary L. Bekker provides guidance, based on her academic expertise in medical decision making, to health policy organisations, patient advocacy groups, health professionals and health scientists on research methods and techniques to develop and evaluate patient decision aids and shared decision making interventions. Her time and expenses in attending meetings, carrying out evaluations and collaborating with other projects are remunerated. She does not gain financially from the outcomes or outputs of these collaborations. Helen Ford has received support from the Health Technology Assessment Programme (NIHR) and the UK MS Society. In the past 3 years, Helen Ford has been a local principal investigator for trials in MS funded by Novartis, Roche, and Biogen Idec and has taken part in advisory boards and consultancy for Merck, Teva, Biogen, and Novartis. Edward Webb, David Meads, Ieva Eskytė, George Pepper, Joachim Marti, Yasmina Okan, Sue Pavitt, and Ana Manzano have no conflicts of interest to declare.
Informed consent
All participants gave informed consent before completing the survey, as well as consent to merge their responses with data from the UK MS Register.
Ethics Approval
Approval for this study was given by a National Health Service (NHS) Research Ethics Committee.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Webb, E.J.D., Meads, D., Eskytė, I. et al. The Impact of Reproductive Issues on Preferences of Women with Relapsing Multiple Sclerosis for Disease-Modifying Treatments. Patient 13, 583–597 (2020). https://doi.org/10.1007/s40271-020-00429-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40271-020-00429-4