
Abstract
Background
Through Patient-Focused Drug Development, the US Food and Drug Administration (FDA) documents the perspective of patients and caregivers and are currently conducting 20 public meetings on a limited number of disease areas. Parent Project Muscular Dystrophy (PPMD), an advocacy organization for Duchenne muscular dystrophy (DMD), has demonstrated a community-engaged program of preference research that would complement the FDA’s approach.
Objective
Our objective was to compare two stated-preference methods, best-worst scaling (BWS) and conjoint analysis, within a study measuring caregivers’ DMD-treatment preferences.
Methods
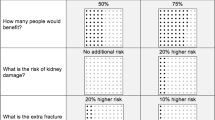
Within one survey, two preference-elicitation methods were applied to 18 potential treatments incorporating six attributes and three levels. For each treatment profile, caregivers identified the best and worst feature and intention to use the treatment. We conducted three analyses to compare the elicitation methods using parameter estimates, conditional attribute importance and policy simulations focused on the 18 treatment profiles. For each, concordance between the results was compared using Spearman’s rho.
Results
BWS and conjoint analysis produced similar parameter estimates (p < 0.01); conditional attribute importance (p < 0.01); and policy simulations (p < 0.01). Greatest concordance was observed for the benefit and risk parameters, with differences observed for nausea and knowledge about the drug—where a lack of monotonicity was observed when using conjoint analysis.
Conclusions
The observed concordance between approaches demonstrates the reliability of the stated-preference methods. Given the simplicity of combining BWS and conjoint analysis on single profiles, a combination approach is easily adopted. Minor irregularities for the conjoint-analysis results could not be explained by additional analyses and needs to be the focus of future research.


Similar content being viewed by others

References
Bushby K, Finkel R, Birnkrant DJ, Case LE, Clemens PR, Cripe L, et al. Diagnosis and management of Duchenne muscular dystrophy, part 1: diagnosis, and pharmacological and psychosocial management. Lancet Neurol. 2010;9(1):77–93.
Eagle M, Baudouin SV, Chandler C, Giddings DR, Bullock R, Bushby K. Survival in Duchenne muscular dystrophy: improvements in life expectancy since 1967 and the impact of home nocturnal ventilation. Neuromuscul Disord. 2002;12(10):926–9.
Center for Disease Control and Prevention (CDC). Prevalence of Duchenne/Becker muscular dystrophy among males aged 5–24 years—Four states, 2007. MMWR Morb Wkly Rep. 2009; 58:1119–22.
Emery AE. Population frequencies of inherited neuromuscular diseases—a world survey. Neuromuscul Disord. 1991;1(1):19–29.
Pangalila RF, van den Bos GA, Stam HJ, van Exel NJA, Brouwer WB, Roebroeck ME. Subjective caregiver burden of parents of adults with Duchenne muscular dystrophy. Disabil Rehabil. 2012;34(12):988–96.
Kenneson A, Bobo JK. The effect of caregiving on women in families with Duchenne/Becker muscular dystrophy. Health Soc Care Commun. 2010;18(5):520–8.
Larkindale J, Yang W, Hogan PF, Simon CJ, Zhang Y, Jain A, et al. Cost of illness for neuromuscular diseases in the United States. Muscle Nerve. 2014;49(3):431–8.
Ouyang L, Grosse SD, Kenneson A. Health care utilization and expenditures for children and young adults with muscular dystrophy in a privately insured population. J Child Neurol. 2008;23(8):883-8.
Ouyang L, Grosse SD, Fox MH, Bolen J. A national profile of health care and family impacts of children with muscular dystrophy and special health care needs in the United States. J Child Neurol. 2012;27(5):569–76.
Angelini C. The role of corticosteroids in muscular dystrophy: a critical appraisal. Muscle Nerve. 2007;36(4):424–35.
Bushby K, Muntoni F, Urtizberea A, Hughes R, Griggs R. Report on the 124th ENMC International Workshop. Treatment of Duchenne muscular dystrophy; defining the gold standards of management in the use of corticosteroids 2–4 April 2004, Naarden, The Netherlands. Neuromuscul Disord. 2004;14(8):526–34.
Biggar W, Harris V, Eliasoph L, Alman B. Long-term benefits of deflazacort treatment for boys with Duchenne muscular dystrophy in their second decade. Neuromuscular Disord. 2006;16(4):249–55.
Govoni A, Magri F, Brajkovic S, Zanetta C, Faravelli I, Corti S, et al. Ongoing therapeutic trials and outcome measures for Duchenne muscular dystrophy. Cell Mol Life Sci. 2013;70(23):4585–602.
Parent Project Muscular Dystrophy. Putting Patients First: Recommendations to speed responsible access to new therapies for Duchenne muscular dystrophy and other rare, serious and life-threatening neurologic disorders. Hackensack; 2013.
Parent Project Muscular Dystrophy. Guidance for Industry: Duchenne Muscular Dystrophy Developing Drugs for Treatment over the Spectrum of Disease. Hackensack; 2014.
U.S. Food and Drug Administration. Enhancing Benefit-Risk Assessment in Regulatory Decision-Making. Silver Spring; 2014. http://www.fda.gov/ForIndustry/UserFees/PrescriptionDrugUserFee/ucm326192.htm. Accessed June 26 2014.
Mullard A. Patient-focused drug development programme takes first steps. Nat Rev Drug Discov. 2013;12(9):651–2.
“Prescription Drug User Fee Act Patient-Focused Drug Development; Announcement of Disease Areas for Meetings Conducted in Fiscal Years 2013–2015”. Federal Register 2013; 78:21613–4.
Peay HL, Hollin I, Fischer R, Bridges JF. A community-engaged approach to quantifying caregiver preferences for the benefits and risks of emerging therapies for Duchenne muscular dystrophy. Clin Ther. 2014;36(5):624–37.
Louviere JJ, Flynn TN. Using best-worst scaling choice experiments to measure public perceptions and preferences for healthcare reform in Australia. Patient. 2010;3(4):275–83.
Molassiotis A, Emsley R, Ashcroft D, Caress A, Ellis J, Wagland R, et al. Applying best-worst scaling methodology to establish delivery preferences of a symptom supportive care intervention in patients with lung cancer. Lung Cancer. 2012;77(1):199–204.
Marti J. A best-worst scaling survey of adolescents’ level of concern for health and non-health consequences of smoking. Soc Sci Med. 2012;75(1):87–97.
Flynn TN, Louviere JJ, Peters TJ, Coast J. Estimating preferences for a dermatology consultation using best-worst scaling: comparison of various methods of analysis. BMC Med Res Methodol. 2008;8(1):76.
Swancutt DR, Greenfield SM, Wilson S. Women’s colposcopy experience and preferences: a mixed methods study. BMC Womens Health. 2008;8(1):2.
Coast J, Salisbury C, De Berker D, Noble A, Horrocks S, Peters T, et al. Preferences for aspects of a dermatology consultation. Br J Dermatol. 2006;155(2):387–92.
Gallego G, Bridges JFP, Flynn T, Blauvelt BM, Niessen LW. Using best-worst scaling in horizon scanning for hepatocellular carcinoma technologies. Int J Technol Assess Health Care. 2012;28(03):339–46. doi:10.1017/S026646231200027X.
Finn A, Louviere JJ. Determining the appropriate response to evidence of public concern: the case of food safety. J Public Policy Market. 1992:12–25.
Marley AA, Louviere JJ. Some probabilistic models of best, worst, and best-worst choices. J Math Psychol. 2005;49(6):464–80.
Bridges J, Kinter E, Kidane L, Heinzen R, McCormick C. Things are looking up since we started listening to patients: recent trends in the application of conjoint analysis in health 1970–2007. Patient. 2008;1(4):273–82.
Flynn TN. Valuing citizen and patient preferences in health: recent developments in three types of best-worst scaling. Expert Rev Pharmacoecon Outcomes Res. 2010;10(3):259–67.
Ryan M, Watson V, Amaya-Amaya M. Methodological issues in the monetary valuation of benefits in healthcare. Expert Rev Pharmacoecon Outcomes Res. 2003;3(6):717–27.
Louviere JJ, Islam T. A comparison of importance weights and willingness-to-pay measures derived from choice-based conjoint, constant sum scales and best-worst scaling. J Bus Res. 2008;61(9):903–11.
Klose T. The contingent valuation method in health care. Health Policy. 1999;47(2):97–123.
Srinivasan V. A conjunctive-compensatory approach to the self-explication of multiattributed preferences. Dec Sci. 1988;19(2):295–305.
Jaeger SR, Jørgensen AS, Aaslyng MD, Bredie WL. Best–worst scaling: an introduction and initial comparison with monadic rating for preference elicitation with food products. Food Qual Prefer. 2008;19(6):579–88.
Cohen S, Orme B. What’s your preference? Market Res. 2004;16(2):32–7.
Cohen S, editor. Maximum difference scaling: improved measures of importance and preference for segmentation. Sawtooth Software Conference Proceedings, Sawtooth Software, Inc; 2003.
Potoglou D, Burge P, Flynn T, Netten A, Malley J, Forder J, et al. Best–worst scaling vs. discrete choice experiments: an empirical comparison using social care data. Soc Sci Med. 2011;72(10):1717–27.
Flynn TN, Louviere JJ, Peters TJ, Coast J. Best–worst scaling: what it can do for health care research and how to do it. J Health Econ. 2007;26(1):171–89.
Bridges JF, Kinter ET, Schmeding A, Rudolph I, Mühlbacher A. Can patients diagnosed with schizophrenia complete choice-based conjoint analysis tasks? Patient. 2011;4(4):267–75.
Kuhfeld W. Orthogonal arrays [TS-723]. Cary: SAS [online]. 2010.
Kinter ET, Prior TJ, Carswell CI, Bridges JF. A comparison of two experimental design approaches in applying conjoint analysis in patient-centered outcomes research. Patient. 2012;5(4):279–94.
Bridges JF, Kinter ET, Kidane L, Heinzen RR, McCormick C. Things are looking up since we started listening to patients. Patient. 2008;1(4):273–82.
Reed Johnson F, Lancsar E, Marshall D, Kilambi V, Mühlbacher A, Regier DA et al. Constructing experimental designs for discrete-choice experiments: report of the ISPOR conjoint analysis experimental design good research practices task force. Value Health. 2013;16(1):3–13.
Carson RT, Hanemann WM, Kopp RJ, Jon AK, Robert Cameron M, Presser S et al. Referendum design and contingent valuation: the NOAA panel’s no-vote recommendation. Rev Econ Stat. 1998;80(2):335–8.
Groothuis PA, Whitehead JC. Does don’t know mean no? Analysis of “don’t know” responses in dichotomous choice contingent valuation questions. Appl Econ. 2002;34(15):1935–40.
McFadden D. Conditional logit analysis of qualitative choice behavior. In: Zarembka P, editor. Frontiers in econometrics. New York: Academic Press; 1974. p. 105–42.
Acknowledgments
The authors appreciate the leadership and commitment of the Parent Project Muscular Dystrophy oversight committee: Pat Furlong, Brian Denger, Sharon Hesterlee, and Kathi Kinnett. We are indebted to the stakeholder informants, parents who participated in the cognitive interviews, and caregivers who completed the survey. This paper was presented at the first meeting of the International Academy for Health Preference Research (IAHPR), 8 November 2014. We are grateful for the feedback we received from the participants of this meeting and of the peer reviewers of this manuscript. This study was conducted with the support from PPMD. Dr. Bridges also acknowledges support from the Patient-Centered Outcomes Research Institute (PCORI) Methods Program Award (ME-1303-5946). ILH conducted data analyses and wrote the manuscript. JFPB and HP conceived and designed the study, analysis plan, and assisted in the writing and reviewing of the manuscript. All authors reviewed and approved the final draft of this manuscript. JFPB acts as the overall guarantor of this article.
Conflict of interest
Holly Peay is an employee of PPMD and John Bridges was hired as a consultant by PPMD to provide methodological expertise. The authors have no conflicts to disclose.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Hollin, I.L., Peay, H.L. & Bridges, J.F.P. Caregiver Preferences for Emerging Duchenne Muscular Dystrophy Treatments: A Comparison of Best-Worst Scaling and Conjoint Analysis. Patient 8, 19–27 (2015). https://doi.org/10.1007/s40271-014-0104-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40271-014-0104-x