
Abstract
The inability to use powerful antituberculosis drugs in an increasing number of patients seems to be the biggest threat towards global tuberculosis (TB) elimination. Simplified, shorter and preferably less toxic drug regimens are being investigated for pulmonary TB to counteract emergence of drug resistance. Intensified regimens with high-dose anti-TB drugs during the first weeks of treatment are being investigated for TB meningitis to increase the survival rate among these patients. Moxifloxacin, gatifloxacin and levofloxacin are seen as core agents in case of resistance or intolerance against first-line anti-TB drugs. However, based on their pharmacokinetics (PK) and pharmacodynamics (PD), these drugs are also promising for TB meningitis and might perhaps have the potential to shorten pulmonary TB treatment if dosing could be optimized. We prepared a comprehensive summary of clinical trials investigating the outcome of TB regimens based on moxifloxacin, gatifloxacin and levofloxacin in recent years. In the majority of clinical trials, treatment success was not in favour of these drugs compared to standard regimens. By discussing these results, we propose that incorporation of extended PK/PD analysis into the armamentarium of drug-development tools is needed to clarify the role of moxifloxacin, gatifloxacin and levofloxacin for TB, using the right dose. In addition, to prevent failure of treatment or emergence of drug-resistance, PK and PD variability advocates for concentration-guided dosing in patients at risk for too low a drug-exposure.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
The optimal fluoroquinolone dose should be investigated for tuberculosis treatment. |
Patients at risk for a too low drug exposure should be selected and monitored. |
1 Introduction
To end tuberculosis (TB) by 2035, as mentioned in the United Nations Sustainable Development Goals, may be an over-ambitious target as evidence is emerging that the TB incidence is not declining at all [1, 2]. Optimization of drug-resistant TB prevention and treatment is a known challenge of global TB elimination [3]. According to the latest annual WHO report (2018), 558,000 new TB patients were infected with rifampicin-resistant (RR) M. tuberculosis (MTB) isolates, resistant against the most important first-line anti-TB agent [4], and in Italy, Iran and India, notation has been made of TB cases resistant against (almost) all second-line anti-TB drugs [5,6,7]. The biggest threat towards TB elimination could therefore well be the increase of resistance against powerful anti-TB agents.
Fluoroquinolones, i.e. moxifloxacin, gatifloxacin and levofloxacin, are the most valuable second-line anti-TB agents according to the current WHO guidelines (update October 2016) [8]. These recommendations were consistent with our forecasts on particularly moxifloxacin and gatifloxacin based on a review on pharmacokinetics (PK) and pharmacodynamics (PD) of 14 fluoroquinolones for TB [9]. Although moxifloxacin was not recommended until the WHO guidelines were updated in 2011, our main finding was that the role of moxifloxacin for drug-resistant TB, possibly at a dose of 600 or 800 mg once daily, was underestimated. This conclusion was based on excellent penetration of moxifloxacin in alveolar macrophages, epithelial lining fluid, bone and cerebrospinal fluid; the highest bactericidal and sterilizing activity; and bactericidal activity against ofloxacin-resistant strains [9]. For moxifloxacin, gatifloxacin and levofloxacin, and for the four high-potential fluoroquinolones for TB as defined in 2011 [9], the current marketing and clinical development status is described in Table 1. The four high potentials have never been under clinical development for TB, and the general marketing status of all seven fluoroquinolones has not changed compared to 2011 [9].
Since rifampicin was authorised for treatment of TB more than half a century ago, the US Food and Drug Administration (FDA) and/or European Medicines Agency (EMA) have only approved bedaquiline (2012) and delamanid (2014) for TB as a last remedy in the case of extensive drug resistance [10, 11]. Currently, the TB pipeline is working on simplification of regimens (shorter, less toxic, oral) to counteract drug resistance by promoting drug adherence [12]. Unfortunately, the results of a short-course drug-susceptible TB regimen based on moxifloxacin were disappointing [13, 14]. However, in 2016, the WHO adopted a shorter regimen—still 9–12 months—for selected patients with multidrug-resistant TB (MDR-TB) [8]. Moxifloxacin or gatifloxacin are preferred components of this shorter regimen, which is restricted to TB patients with no history of second-line drugs and no resistance against pyrazinamide, fluoroquinones or aminoglycosides [8]. From 2011 onwards, in TB research and WHO guidelines, fluoroquinolones (moxifloxacin, gatifloxcin, levofloxacin) have been given an important share in regimens for drug-susceptible and drug-resistant TB. This role seems justified based on its PK and PD [9]. The aim of this review was to update, summarize and discuss the treatment outcome of regimens based on moxifloxacin, gatifloxacin or levofloxacin for TB.
2 Methods
A PubMed search was preformed using the keywords “moxifloxacin” OR “levofloxacin” OR “gatifloxacin” AND “tuberculosis”. The limitations “human”, “English” and a publication date of the last “5 years”, and article types “clinical trial”, “randomized controlled trial”, “controlled clinical trial” and “comparative study” were added to the searches. We included articles reporting bacteriological and/or clinical treatment outcome. Publications reporting only pharmacokinetic outcome and/or early bactericidal results were excluded. Trials were included regardless of the extent of drug-resistance and regardless of the localization of TB. All searches were conducted in June 2017. Searches up to and including December 2018 revealed no new articles.
3 Results
3.1 Pulmonary Tuberculosis
Five clinical trials investigated the treatment outcome of moxifloxacin, gatifloxacin and/or levofloxacin for pulmonary TB (Tables 2, 3). In one clinical trial [15], moxifloxacin was compared with levofloxacin as part of an MDR-TB regimen. In the remaining four clinical trials [13, 14, 16, 17], results of seven fluorquinolone-based regimens (moxifloxacin: five, gatifloxacin: two) compared to a standard WHO-recommended daily (five times) or thrice-weekly (two times, moxifloxacin: one, gatifloxacin: one) drug-susceptible (DS) TB treatment, were published. A thrice-weekly DS-TB regimen is no longer recommended in the WHO guidelines [18].
3.1.1 Four-month Fluoroquinolone-Containing Regimens
A 2-month shorter regimen was investigated in six out of seven fluoroquinolone regimens for DS-TB, but none of these regimens demonstrated a favourable outcome after a follow-up period of at least 6 months, compared to the standard DS-TB regimen (Tables 2, 3, S). A remarkably higher TB recurrence rate was observed in the experimental compared to the control arms [13, 14, 17], leading to premature termination of both the moxifloxacin- and gatifloxacin-containing arm in one clinical trial [17]. Additionally, in one of the other clinical trials, non-inferiority was not observed after 12 months of follow-up, but was observed at the end of treatment for two moxifloxacin-containing regimens [13]. Moreover, in the preliminary terminated study [17], with the only thrice-weekly control and experimental regimens, a higher TB recurrence rate was observed for gatifloxacin (16%) compared to moxifloxacin (10%), and almost all recurrences occurred before the sixth month post-treatment. A minimal increase in unfavourable outcome was observed at the end of treatment [17]. Finally, one clinical trial suggested that standard DS-TB treatment might even benefit specific patient populations, like DS-TB patients with an HIV-negative status, if a daily 4-month gatifloxacin regimen is the alternative treatment option [16].
3.1.2 Moxifloxacin
The treatment-shortening potential of moxifloxacin has been the most studied subject in recent years with regard to fluoroquinolones for pulmonary TB (Tables 2, 3). Contrary to the results of these 4-month regimens, the efficacy, including the relapse rate after treatment, of a 6-month course that included 4 months of once-a-week dosing of moxifloxacin and rifapentine was similar to that of the standard DS-TB regimen [14]. For MDR-TB treatment success, moxifloxacin and levofloxacin (750 mg/day) were equally effective in one clinical trial [15].
3.2 Tuberculosis Meningitis
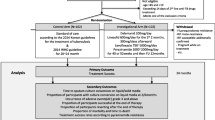
Three clinical trials investigated the survival benefit of a fluoroquinolone added to, or replacing, a drug from the standard regimen for the treatment of TB meningitis (TBM) (Table 4). A significant survival benefit (hazard ratio: 2.13, 95% CI 1.04–4.34, P = 0.04) was observed for TBM patients, regardless of stage of TBM, treated with levofloxacin (10 mg/kg/day, maximum 500 mg/day) instead of rifampicin, next to isoniazid, pyrazinamide and ethambutol. Although the proportion of patients with an unfavourable outcome did not change in the per-protocol analysis (excluding patients with serious adverse events) for both treatment groups, it was striking that levofloxacin had to be discontinued in 16 of 60 patients mainly due to seizures [19]. In the remaining two clinical trials [20, 21], intensified TBM regimens for DS-TB were investigated that included high-dose fluoroquinolone (levofloxacin or moxifloxacin) and/or high-dose rifampicin during the first weeks of treatment. Adding levofloxacin (20 mg/kg/day) plus rifampicin (5 mg/kg/day) to the standard drug combination during the first 8 weeks of treatment did not contribute to reducing death after 9 months of treatment [20]. Although the sample size was small and the study was exploratory, replacing ethambutol with moxifloxacin (400 or 800 mg) in the first 2 weeks of standard DS-TB treatment was also not associated with any survival benefit [21]. On the other hand, in this study high-dose rifampicin (600 mg intravenously) in the first 2 weeks of treatment was associated with a lower 6-month mortality compared to the standard rifampicin dose (450 mg orally) [21].
4 Discussion
4.1 Pulmonary Tuberculosis
The main finding of this review is that the 4-month moxifloxacin- or gatifloxacin-containing regimens successfully treated 75–90% of pulmonary TB patients, but none of them demonstrated a favourable outcome after a follow-up period of at least 6 months, compared to the standard DS-TB regimen (Tables 2, 3). Particularly, the TB relapse rate after treatment was remarkable.
MTB has the capacity to survive in a hypoxic environment by switching to a low-replicating and low-metabolic rate, resulting in a difficult-to-treat sub-population of persistent TB bacilli in pulmonary TB lesions [22], and thus several months of treatment are needed to attain sterilising treatment. The indication that moxifloxacin or gatifloxacin had the potential to shorten DS-TB treatment was based on the in vitro bactericidal activity of moxifloxacin and gatifloxacin against anaerobic, non-replicating TB bacilli. Also, a stable cure in BALB/c mice was reached after 4 instead of 6 months of treatment with isoniazid replaced by moxifloxacin and a similar or higher proportion of TB patients with negative sputum culture after 8 weeks of treatment was reached with moxifloxacin or gatifloxacin instead of isoniazid or ethambutol [23,24,25,26,27,28]. A poor predictive value of the pre-clinical study designs used and a sub-optimal exposure of anti-TB drugs at the site of infection might explain the unfavourable results of these shorter-course regimens.
First, the standard BALB/c mouse does not exhibit the TB lesion heterogeneity as seen in humans, making this mouse model possibly unsuitable to study in vivo activity of drugs against non-replicating TB bacilli [29]. The C3HeB/FeJ mouse, on the other hand, may be more suitable [29]. In addition, the two 4-month moxifloxacin-containing regimens of the REMoxTB Phase III study were retrospectively evaluated in a pre-clinical model with C3HeB/FeJ mice [30]. In accordance with the results of the Phase III trial, a stable cure was also not expected after 4 months of treatment based on this murine model [30]. Second, using in vitro PK/PD modelling and Monte Carlo simulations, it has been suggested that a daily dose of 800 mg of moxifloxacin or more is needed for optimal kill of MTB and to suppress drug-resistant mutants in log-phase growth [31, 32]. The optimal sterilizing dose is thus unknown, but 400 mg/day is likely not the optimal dosage of moxifloxacin for TB. In addition, combination therapy with rifampicin might be synergistic for suppression of drug resistance (MTB in log-phase growth), but antagonistic for the time needed to kill the non-growing mycobacterial population [32]. Given the possible paradoxical effect of rifampicin on moxifloxacin, the predictive performance for sterilizing activity of Phase IIB studies, investigating culture conversion at 2 months of moxifloxacin substituted for isoniazid or ethambutol in a standard DS-TB regimen, is at least questionable. Also, PD interactions (synergistic, antagonistic or additive) might be concentration dependent. An in vitro hollow fibre system (HFS) has the ability to study both the bactericidal and sterilizing effects for drug combinations using a variety of concentrations over time [29, 33]. Therefore, the HFS might be a useful model to study potentially sterilizing drugs like moxifloxacin and gatifloxacin, as part of a standard or new TB regimen. Recently, the HFS was used to select the optimal sterilizing dose of both linezolid and ertapenem-clavulanate for TB [34, 35].
Furthermore, in our TB patients treated under direct observation (DOT), moxifloxacin PK variability in plasma was found to be ninefold on 400 mg/day [36]. The PK of all anti-tuberculosis drugs could be affected by TB disease activity (wasting, loss of lean body mass, fat and serum proteins), HIV, diabetes or drug–drug interactions [37, 38]. The PK interaction between rifampicin and moxifloxacin is well known [39, 40]. Also male gender might be a risk factor for reduced moxifloxacin exposure in the early phase of treatment, which is probably due to disease-related intestinal dysfunction (publication submitted). In healthy volunteers, moxifloxacin has a high penetration into alveolar macrophages and epithelial lining fluid [9]. However, based on MALDI mass spectrometry imaging, the penetration of moxifloxacin into the hypoxic sites of pulmonary lesions of TB patients is marginal compared to the oxygen-rich sites, and compared to rifampicin [41]. All together, the optimal sterilizing dose appears to differ from one patient to another, probably due to PK variability, and this advocates for sub-group analyses in pre-clinical animal models (e.g. extent of cavitation) and clinical trials (e.g. low body mass index (BMI)), and also for drug-concentration monitoring in patients at risk for low drug exposure during treatment. Despite limited data on gatifloxacin PK, in one of the Phase III trials (OFLOTUB), the 4-month gatifloxacin-containing regimen was not associated with treatment success for the total group of patients, but was in favour of treatment success for patients without cavitation, for patients with HIV co-infection, and for patients with a low BMI, compared to the standard DS-TB regimen [16].
In recent years, one clinical trial compared two conventional MDR-TB regimens (Tables 2, 3). In accordance with the results of this study [15], a recent individual patient data meta-analysis showed that incorporation of moxifloxacin or levofloxacin in a MDR/RR-TB regimen is associated with treatment success [42]. The current WHO guidelines (October 2016) proposed a shorter-course—still 9–12 months—regimen for RR/MDR-TB patients [8]. This largely standardized gatifloxacin- (or moxifloxacin-) containing regimen is based on three observational studies of cohorts from Bangladesh, Niger and Cameroon, supplemented with individual patient data [8, 43,44,45]. Although the number of patients in follow-up was limited, MDR/RR-TB patients without previous use of second-line drugs, and without resistance against fluoroquinolones and injectable agents, were found likely enough to benefit from this shorter regimen [8]. An important note is that the short-course Bangladesh regimen included high-dose gatifloxacin (600 mg for a bodyweight of 33–50 kg, 800 mg for > 50 kg) [43, 45]. In the prospective evaluation of the shorter-course regimen for MDR/RR-TB, gatifloxacin was replaced by moxifloxacin because of market withdrawal of gatifloxacin due to dysglycaemia. Although patients with a bodyweight > 50 kg are also treated with 800 mg of moxifloxacin once daily in this STREAM stage 1 trial [46], it is still questionable if this weight-band dosing is optimal for a sterilizing and bactericidal effect. In August 2018, the WHO published a rapid communication regarding reclassification of core anti-TB drugs. Moxifloxacin or levofloxacin have remained core agents in the conventional and shorter course MDR/RR-TB regimen [47]. As earlier suggested for DS-TB, and as was proposed for ertapenem-clavulanate [35], we propose a combination of studies in HFS and Monte Carlo simulations, using RR/MDR-TB patient data, to select the sterilizing fluoroquinolone dose most suitable to be tested in controlled Phase III trials as part of RR/MDR-TB regimens.
4.2 Tuberculosis Meningitis
A significant survival benefit for TBM patients treated with a fluoroquinolone-containing regimen was observed in one of the three published clinical trials (Table 4). The idea to use moxifloxacin and levofloxacin for improvement of TBM survival is based on favourable penetration into cerebrospinal fluid (CSF) [9]. Because an evidence-based regimen is lacking, TBM patients are often treated (for a pragmatic longer period) with the standardized pulmonary TB regimen, as recommended by the WHO despite the fact that rifampicin only marginally penetrates into CSF [18, 48]. In the only RCT with favourable results for the patients treated with a fluoroquinolone [19], levofloxacin was compared to rifampicin, both using a standard dose, next to isonazid, pyrazinamide and ethambutol. The improved outcome for TBM patients treated with levofloxacin might be explained by the much better penetration of levofloxacin into CSF compared to rifampicin [9, 48].
As adequate early-phase treatment is important to prevent patients suffering from TBM to deteriorate, the two remaining clinical studies investigated intensified, high-dose therapies during the early phase of TBM treatment [20, 21]. Although the trial with moxifloxacin was not powered for survival analysis, instead of the high-dose moxifloxacin (800 mg) treatment, the ‘high-dose’ rifampicin (600 mg iv) treatment in the first 2 weeks, given in an attempt to increase CSF drug-exposure, was associated with survival benefit [21]. In this study, the moxifloxacin dose was escalated because of the well-known drug-drug interaction with rifampicin. An additional PK/PD analysis was done to investigate the extent to which exposure was related to outcome [49]. Despite the small sample size, moxifloxacin AUC was not, but the AUC of rifampicin was related to TBM survival, and therefore the authors concluded that increasing the rifampicin dose above 600 mg might be the way forward to further optimize TBM treatment. However, there was a trend to a higher moxifloxacin peak-plasma concentration for patients who survived at least 2 weeks. We therefore agree with the authors that an extended cumulative PK/PD analysis of the TBM regimen is needed to clarify the (long-term) role of moxifloxacin for TBM [50, 51]. The same might be true for the third study [20], including high dosages of levofloxacin and rifampicin in the first 8 weeks added to isoniazid, rifampicin, pyrazinamide and ethambutol, which did not result in a cumulative survival benefit. Remarkably, the head-to-head comparison of standard dosages of levofloxacin and rifampicin in the first study was in favour of levofloxacin [19], which might support further investigating the relationship between drug-exposure and outcome in a multiple drug-regimen. Also, in other bacteria quinolones have a concentration-dependent killing with a post-antibiotic effect. However, it is at least questionable if the half-life of levofloxacin is long enough to fullfill the criteria for once-daily dosing in TB, i.e. to prevent drug-resistant mutant selection [9]. Further research of the optimal dosing interval of levofloxacin for TB is therefore also important.
Finally, considering that the (protein-unbound) drug-exposure in plasma is closely linked to drug-exposure in CSF, as for plasma, CSF PK variability might play an important role. Therefore, the identification of sub-groups at risk for inadequate CSF exposure might be important for clinical research and clinical practice. Inadequate drug-exposure may result in drug resistance and high drug exposure in toxicity, and, as CSF penetration has to be sufficiently high, second-line treatment options are even more limited for TBM compared to the second-line drug options for pulmonary TB. Aminoglycosides belong to the core RR/MDR-TB agents; however, these drugs have marginal penetration into CSF [48]. In addition, a recent sub-group analysis showed that in isoniazid-monoresistant TB, an intensified combination of levofloxacin and rifampicin in the early phase of treatment was associated with a lower 9-month mortality, although an overall survival benefit was not observed. Levofloxacin combined with rifampicin might therefore provide a survival benefit for isoniazid-resistant TBM patients [20, 52]. With regard to the safety of high-dose fluoroquinolones, data are limited, but no increase of serious adverse events was reported for levofloxacin or moxifloxacin in TBM patients [20, 21, 53]. However, high-dose moxifloxacin was always combined with rifampicin in these studies and a high incidence of seizures was observed by using the standard dose of levofloxacin [19, 21, 53]. The authors of the standard-dose levofloxacin study suggested that there could have been a relatively high seizure potential amongst their patients due to inter alia severe meningitis [19]. Also, recently a ‘black box’ warning was launched by the FDA on potential neurotoxicity and low blood sugar levels after administration of fluoroquinolones [54]. However, as long as there is no drug-exposure breakpoint for safety, ECG monitoring is still recommended for high-dose moxifloxacin, especially when combined with bedaquiline in the newest WHO prioritized MDR/RR-TB regimen [47, 55], and one should be aware of seizures when using (high-dose) levofloxacin.
5 Conclusion
We provide a comprehensive summary of clinical trials investigating the outcome of fluoroquinolone-containing regimens for TB in the recent years. In general, the results of these trials were not in favour of fluoroquinolones for TB. Moxifloxacin, levofloxacin and gatifloxacin are important second-line anti-TB agents, but we advise extended PK/PD analysis to measure drug exposure, and identify suitable dosing, for clarification of the role of fluoroquinolones as sterilizing agents for pulmonary TB and as first-line agent for TBM. PK variability calls for sub-group analysis or strict inclusion criteria in clinical trials, and for therapeutic drug monitoring in patients at risk for inadequately low exposure. Therefore, to prevent failure of treatment and emergence of drug resistance, a strategy for concentration-guided dosing, including point-of-care tools, is the proposed way forward [56, 57].
References
Murray CJ, Ortblad KF, Guinovart C, et al. Global, regional, and national incidence and mortality for HIV, tuberculosis, and malaria during 1990–2013: a systemic analysis for the Global Burden of Disease study 2013. Lancet. 2014;384(9947):1005–70.
World Health Organization (WHO) (ed.). The end TB strategy: Global strategy and targets for tuberculosis prevention, care, and control after 2015. World Health Organization, Geneva, Switzerland; 2014.
Lönnroth K, Migliori GB, Abubakar I, et al. Towards tuberculosis elimination: an action framework for low-incidence countries. Eur Respir J. 2015;45(4):928–52.
World Health Organization (WHO) (ed.). Global tuberculosis report 2018. World Health Organization, Geneva, Switzerland; 2018.
Migliori GB, De Laco G, Besozzi G, Centis R, Cirillo DM. First tuberculosis cases in Italy resistant to all tested drugs. Eurosurveillance. 2007;12(5):E070517.1.
Velyati AA, Masjedi MR, Farnia P, Tabarsi P, Ghanavi J, Ziazarifi AH, Hoffner SE. Emergence of new forms of totally drug-resistant tuberculosis bacilli: super extensively drug-resistant tuberculosis or totally drug-resistant strains in iran. Chest. 2009;136(2):420–5.
Udwadia ZF, Amale RA, Ajbani KK, Rodrigues C. Totally drug-resistant tuberculosis in India. Clin Infect Dis. 2012;54(4):579–81.
Falzon D, Schűnemann HJ, Harausz E, González-Angulo L, Lienhardt C, Jaramillo E, Weyer K. World Health Organization treatment guidelines for drug-resistant tuberculosis, 2016 update. Eur Respir J. 2017;49(3):1602308.
Pranger AD, Alffenaar JW, Aarnoutse RE. Fluoroquinolones, the cornerstone of treatment of drug-resistant tuberculosis: a pharmacokinetic and pharmacodynamics approach. Curr Pharm Des. 2011;17(27):2900–30.
U.S. Food & Drug Administration (FDA) (ed.). Drugs@FDA: FDA Approved Drug Products. U.S. Department of Health and Human Services, Washington D.C., United States of America. http://www.fda.gov. Accessed 17 Mar 2018, 3 Dec 2018.
European Medicines Agency (EMA) (ed.). European public assessment reports. European Union, London, United Kingdom. http://www.ema.europe.eu. Accessed 17 Mar 2018.
Working Group on New Drugs (ed.). Clinical pipeline. Stop TB Partnership. http://www.newtbdrugs.org. Accessed 17 Mar 2018, 3 Dec 2018.
Gillespie SH, Crook AM, McHugh TD, Mendel CM, Meredith SK, Murray SR, Pappas F, Phillips PP, Nunn AJ, REMoxTB Consortium. Four-month moxifloxacin-based regimens for drug-sensitive tuberculosis. N Engl J Med. 2014;371(17):1577–87.
Jindani A, Harrison TS, Nunn AJ, Phillips PP, Churchyard GJ, Charalambous S, Hatherill M, Geldenhuys H, Mcllleron HM, Zvada SP, Mungofa S, Shah NA, Zizhou S, Magweta L, Shepard J, Nyirenda S, van Dijk JH, Clouting HE, Coleman D, Bateson AL, McHugh TD, Butcher PD, Mitchison DA, RIFAQUIN Trial Team. High-dose rifapentine with moxifloxacin for pulmonary tuberculosis. N Engl J Med. 2014;371(17):1599–608.
Kang YA, Shim TS, Koh WJ, Lee SH, Lee CH, Choi JC, Lee JH, Jang SH, Yoo KH, Jung KH, Kim KU, Choi SB, Ryu YJ, Kim KC, Um S, Kwon YS, Kim YH, Choi WI, Jeon K, Hwang YI, Kim SJ, Lee HK, Heo E, Yim JJ. Choice between levofloxacin and moxifloxacin and multidrug-resistant tuberculosis treatment outcomes. Ann Am Thorac Soc. 2016;13(3):364–70.
Merle CS, Fielding K, Sow OB, Gninafon M, Lo MB, Mthiyane T, Odhiambo J, Amukoye E, Bah B, Kassa F, N’Diaye A, Rustomjee R, de Jong BC, Horton J, Perronne C, Sismanidis C, Lapujade O, Olliaro PL, Lienhardt C, OFLOTUB/Gatifloxacin for Tuberculosis Project. A four-month gatifloxacin-containing regimen for treating tuberculosis. N Engl J Med. 2014;371(17):1588–98.
Jawahar MS, Banurekha VV, Paramasivan CN, Rahman F, Ramachandran R, Venkatesan P, Balasubramanian R, Selvakumar N, Ponnuraja C, Iliayas AS, Gangadevi NP, Raman B, Baskaran D, Kumar SR, Kumar MM, Mohan V, Ganapathy S, Kumar V, Shanmugam G, Charles N, Sakthivel MR, Jaqannath K, Chandrasekar C, Parthasarathy RT, Narayanan PR. Randomized clinical trial of thrice-weekly 4-month moxifloxacin or gatifloxacin containing regimens in the treatment of new sputum positive pulmonary tuberculosis patients. PLoS One. 2013;8(7):e67030.
World Health Organization (WHO) (ed.). Guidelines for treatment of drug-susceptible tuberculosis and patient care (2017 update). World Health Organization, Geneva, Switzerland; 2017.
Kalita J, Misra UK, Prasad S, Bhoi SK. Safety and efficacy of levofloxacin versus rifampicin in tuberculosis meningitis: an open-label randomized controlled trial. J Antimicrob Chemother. 2014;69(8):2246–51.
Heemskerk AD, Bang ND, Mai NT, Chau TT, Phu NH, Loc PP, Chau NV, Hien TT, Dung NH, Lan NT, Lan NH, Lan NN, le Phong T, Vien NN, Hien NQ, Yen NT, Ha DT, Day JN, Caws M, Merson L, Thinh TT, Wolbers M, Thwaites GE, Farrar JJ. Intensified antituberculosis therapy in adults with tuberculous meningitis. N Engl J Med. 2016;374(2):124–34.
Ruslami R, Ganiem AR, Dian S, Apriani L, Achmad TH, van der Ven AJ, Borm G, Aarnoutse RE, van Crevel R. Intensified regimen containing rifampicin and moxifloxacin for tuberculous meningitis: an open-label randomised controlled phase 2 trial. Lancet Infect Dis. 2013;13(1):27–35.
Boon C, Dick T. How Mycobacterium tuberculosis goes to sleep: the dormancy survival regulator DosR a decade later. Future Microbiol. 2012;7(4):513–8.
Lakshminarayana SB, Huat TB, Ho PC, Manjunatha UH, Dartois V, Dick T, Rao SP. Comprehensive physiochemical, pharmacokinetic and activity profiling of anti-TB agents. J Antimicrob Chemother. 2015;70(3):857–67.
Nuermberger EL, Yoshimatsu T, Tyagi S, Williams K, Rosenthal I, O’Brien RJ, Vernon AA, Chaisson RE, Bishai WR, Grosset JH. Moxifloxacin-containing regimen of reduced duration produce a stable cure in murine tuberculosis. Am J Respir Crit Care Med. 2004;170(10):1131–4.
Dorman SE, Johnson JL, Goldberg S, Muzanye G, Padayatchi N, Bozeman L, Heilig CM, Bernardo J, Choudhri S, Grosset JH, Guy E, Guyadeen P, Leus MC, Maltas G, Menzies D, Nuermberger EL, Villarino M, Vernon A, Chaisson RE, Tuberculosis Trials Consortium. Substitution of moxifloxacin for isoniazid during intensive phase treatment of pulmonary tuberculosis. Am J Respir Crit Care Med. 2009;180(3):273–80.
Burman WJ, Goldberg S, Johnson JL, Muzanye G, Engle M, Mosher AW, Choudhri S, Daley CL, Munsiff SS, Zhao Z, Vernon A, Chaisson RE. Moxifloxacin versus ethambutol in the first 2 months of treatment for pulmonary tuberculosis. Am J Respir Crit Care Med. 2006;174(3):331–8.
Conde MB, Efron A, Loredo C, De Souza GR, Graca NP, Cezar MC, Ram M, Chaudhary MA, Bishai WR, Kritski AL, Chaisson RE. Moxifloxacin versus ethambutol in the initial treatment of tuberculosis: a double-blind, randomised, controlled phase II trial. Lancet. 2009;373(9670):1183–9.
Rustomjee R, Lienhardt C, Kanyok T, Davies GR, Levin J, Mthiyane T, Reddy C, Sturm AW, Sirgel FA, Allen J, Coleman DJ, Fourie B, Mitchison DA, Gatifloxacin for TB (OFLOTUB) Study Team. A phase II study of the sterilising activities of ofloxacin, gatifloxacin and moxifloxacin in pulmonary tuberculosis. Int J Tuberc Lung Dis. 2008;12(2):128–38.
Gumbo T, Lenaerts AJ, Hanna D, Romero K, Nuermberger E. Nonclinical models for antituberculosis drug development: a landscape analysis. J Infect Dis. 2015;211(Suppl 3):S83–95.
Li SY, Irwin SM, Converse PJ, Mdluli KE, Lenaerts AJ, Nuermberger EL. Evaluation of moxifloxacin-containing regimens in pathologically distinct murine tuberculosis models. Antimicrob Agents Chemother. 2015;59(7):4026–30.
Gumbo T, Louie A, Deziel MR, Parsons LM, Salfinger M, Drusano GL. Selection of a moxifloxacin dose that suppresses drug resistance in Mycobacterium tuberculosis, by use of an in vitro pharmacodynamic infection model and mathematical modelling. J Infect Dis. 2004;190(9):1642–51.
Drusano GL, Sqambati N, Eichas A, Brown DL, Kulawy R, Louie A. The combination of rifampin plus moxifloxacin is synergistic for suppression of resistance but antagonistic for cell kill of Mycobacterium tuberculosis as determined in a hollow-fiber infection model. MBio. 2010;1(3):e00139-10.
Gumbo T, Angulo-Barturen I, Ferrer-Bazaga S. Pharmacokinetic-pharmacodynamic and dose-response relationships of antituberculosis drugs: recommendations and standards for industry and academia. J Infect Dis. 2015;211(Suppl 3):S96–106.
Srivastava S, Magombedze G, Koeuth T, Sherman C, Pasipanodya JG, Raj P, Wakeland E, Deshpande D, Gumbo T. Linezolid dose that maximizes sterilizing effect while minimizing toxicity and resistance emergence for tuberculosis. Antimicrob Agents Chemother. 2017. https://doi.org/10.1128/AAC.00751-17.
Van Rijn SP, Srivastava S, Wessels MA, van Soolingen D, Alffenaar JC, Gumbo T. The sterilizing effect of ertapenem-clavulanate in a hollow fiber model of tuberculosis and implications on clinical dosing. Antimicrob Agents Chemother. 2017. https://doi.org/10.1128/AAC.02039-16.
Pranger AD, van Altena R, Aarnoutse RE, van Soolingen D, Uges DR, Kosterink JG, van der Werf TS, Alffenaar JW. Evaluation of moxifloxacin for the treatment of tuberculosis: 3 years of experience. Eur Respir J. 2011;38(4):888–94.
Macallan DC. Malnutrition in tuberculosis. Diagn Microbiol Infect Dis. 1999;34(2):153–7.
Devaleenal Daniel B, Ramachandran G, Swaminathan S. The challenges of pharmacokinetic variability of first-line anti-TB drugs. Expert Rev Clin Pharmacol. 2017;10(1):47–58.
Nijland HM, Ruslami R, Suroto AJ, Burger DM, Alisjahbana B, van Crevel R, Aarnoutse RE. Rifampicin reduces plasma concentrations of moxifloxacin in patients with tuberculosis. Clin Infect Dis. 2007;45(8):1001–7.
Weiner M, Burman W, Luo CC, Peloquin CA, Engle M, Goldberg S, Agarwal V, Vernon A. Effect of rifampin and multidrug resistance gene polymorphism on concentrations of moxifloxacin. Antimicrob Agents Chemother. 2007;51(8):2861–6.
Prideaux B, Via LE, Zimmerman MD, Eum S, Sarathy J, O’Brien P, Chen C, Kaya F, Weiner DM, Chen PY, Song T, Lee M, Shim TS, Cho JS, Kim W, Cho SN, Olivier KN, Barry CE 3rd, Dartois V. The association between sterilizing activity and drug distribution into tuberculosis lesions. Nat Med. 2015;21(10):1223–7.
Ahmad N, Ahuja SD, Akkerman OW, et al. Collaborative group for the meta-analysis of individual patient data in MDR-TB treatment-2017. Treatment correlates of successful outcomes in pulmonary multidrug-resistant tuberculosis: an individual patient data meta-analysis. Lancet. 2018;392(10150):821–34.
Van Deun A, Maug AK, Salim MA, Das PK, Sarker MR, Daru P, Rieder HL. Short, highly effective, and inexpensive standardized treatment of multidrug-resistant tuberculosis. Am J Respir Crit Care Med. 2010;182(5):684–92.
Kuaban C, Noeske J, Rieder HL, Ait-Khaled N, Abena Foe JL, Trebucq A. High effectiveness of a 12-month regimen for MDR-TB patients in Cameroon. Int J Tuberc Lung Dis. 2015;19(5):517–24.
Piubello A, Harouna SH, Souleymane MB, Boukary I, Morou S, Daouda M, Hanki Y, van Deun A. High cure rate with standardised short-course multidrug-resistant tuberculosis treatment in Niger: no relapses. Int J Tuberc Lung Dis. 2014;18(10):1188–94.
Moodley R, Godec TR, STREAM Trial Team. Short-course treatment for multidrug-resistant tuberculosis: the STREAM trials. Eur Respir Rev. 2016;25(139):29–35.
World Health Organization (WHO) (ed.). Rapid Communication: key changes to treatment of multidrug- and rifampicin-resistant tuberculosis (MDR/RR-TB). World Health Organization, Geneva, Switzerland; 2018.
Thwaites GE, van Toorn R, Schoeman J. Tuberculosis meningitis: more questions, still too few answers. Lancet Neurol. 2013;12(10):999–1010.
Te Brake L, Dian S, Ganiem AR, Ruesen C, Burger D, Donders R, Ruslami R, van Crevel R, Aarnoutse R. Pharmacokinetic/pharmacodynamic analysis of an intensified regimen containing rifampicin and moxifloxacin for tuberculosis meningitis. Int J Antimicrob Agents. 2015;45(5):496–503.
Ruslami R, Ganiem AR, Aarnoutse RE, van Crevel R, Study Team. Rifampicin and moxifloxacin for tuberculous meningitis—authors’ reply. Lancet Infect Dis. 2013;13(7):570.
Akkerman O, Pranger A, van Altena R, van der Werf T, Alffenaar JW. Rifampicin and moxifloxacin for tuberculous meningitis. Lancet Infect Dis. 2013;13(7):568–9.
Heemskerk AD, Nguyen MTH, Dang HTM, Vinh Nguyen CV, Nguyen LH, Do TDA, Nguyen TTT, Wolbers M, Day J, Le TTP, Nguyen BD, Caws M, Thwaites GE. Clinical outcomes of patients with drug-resistant tuberculous meningitis treated with an intensified antituberculosis regimen. Clin Infect Dis. 2017. https://doi.org/10.1093/cid/cix230 (Epub ahead of print).
Alffenaar JW, van Altena R, Bokkerink HJ, Luijckx GJ, van Soolingen D, Aarnoutse RE, van der Werf TS. Pharmacokinetics of moxifloxacin in cerebrospinal fluid and plasma in patients with tuberculous meningitis. Clin Infect Dis. 2009;49(7):1080–2.
U.S. Food & Drug Administration (FDA) (ed.). FDA reinforces safety information about serious low blood sugar levels and mental health side effects with fluoroquinolone antibiotics; requires label changes (7/10/2018). U.S. Department of Health and Human Services, Washington D.C., United States of America. http://www.fda.gov. Accessed 3 Dec 2018.
Borisov SE, Dheda K, Enwerem M, et al. Effectiveness and safety of bedaquiline-containing regimens in the treatment of MDR- and XDR-TB: a multicentre study. Eur Respir J. 2017;49(5):1700387.
Ghimire S, Bolhuis MS, Sturkenboom MG, Akkerman OW, de Lange WC, van der Werf TS, Alffenaar JW. Incorporating therapeutic drug monitoring into the World Health Organization hierarchy of tuberculosis diagnostics. Eur Respir J. 2016;47(6):1867–9.
Forsman LD, Bruchfeld J, Alffenaar JC. Therapeutic drug monitoring to prevent acquired drug resistance of fluoroquinolones in the treatment of tuberculosis. Eur Respir J. 2017;49(4):1700173.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Data availability
All data generated or analysed during this literature review are included in this article.
Funding
No funding was received to conduct the literature review described in this manuscript or to assist with preparation of the manuscript.
Conflict of interest
The authors A.D. Pranger, T.S van der Werf, J.G.W. Kosterink, and J.W.C.Alffenaar, declare that they have no conflicts of interest.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Pranger, A.D., van der Werf, T.S., Kosterink, J.G.W. et al. The Role of Fluoroquinolones in the Treatment of Tuberculosis in 2019. Drugs 79, 161–171 (2019). https://doi.org/10.1007/s40265-018-1043-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40265-018-1043-y