
Abstract
Introduction
Traditional nonselective, nonsteroidal anti-inflammatory drugs (NSAIDs) are known to cause salt and fluid retention and should thus be used cautiously in patients with documented heart failure. Recent studies have found that some NSAIDs, including cyclooxygenase (COX)-2 inhibitors, are associated with an increased risk of incident heart failure regardless of the related medical history of the patient.
Objective
This study aimed to investigate the potential link between NSAIDs (both COX-2 inhibitors and traditional nonselective NSAIDs) and heart failure in patients without a history of heart failure.
Methods
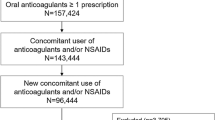
We conducted a case-crossover study using the National Health Insurance Research Database (NHIRD) in Taiwan. A total of 5615 subjects with a first hospitalization for heart failure between 2005 and 2013 were identified from the NHIRD. Exposure to individual NSAIDs between the case period (1–30 days before the index date) and control period (121–150 days before the index date) were retrieved. Multivariable conditional logistic regression models were used to estimate the adjusted odds ratios (aORs) of the incident heart failure associated with NSAID use after adjustments for potential confounders. Multiple sensitivity analyses, including the case-time-control analysis, were performed to test the robustness of the study results.
Results
Overall, NSAID use was associated with a 1.58-fold risk [aOR 1.58; 95% confidence interval (CI) 1.40–1.79] of heart failure leading to hospitalization in the main analysis, and similar results were obtained in the case-time-control analysis [aOR 1.40 (95% CI 1.18–1.67)]. The increased risks of heart failure were comparable between traditional NSAIDs [aOR 1.53 (95% CI 1.35–1.74)] and COX-2 inhibitors [aOR 1.74 (95% CI 1.25–2.44)]. Among all NSAIDs, ketorolac was associated with the highest risk of heart failure [aOR 1.98 (95% CI 1.37–2.86)].
Conclusion
Both traditional NSAIDs and COX-2 inhibitors were associated with an increased risk of heart failure leading to hospitalization in patients without a related history of heart failure.

Similar content being viewed by others


References
Sostres C, Gargallo CJ, Arroyo MT, Lanas A. Adverse effects of non-steroidal anti-inflammatory drugs (NSAIDs, aspirin and coxibs) on upper gastrointestinal tract. Best Pract Res Clin Gastroenterol. 2010;24(2):121–32.
Harirforoosh S, Asghar W, Jamali F. Adverse effects of nonsteroidal antiinflammatory drugs: an update of gastrointestinal, cardiovascular and renal complications. J Pharm Pharm Sci. 2013;16(5):821–47.
McGettigan P, Henry D. Cardiovascular risk and inhibition of cyclooxygenase: a systematic review of the observational studies of selective and nonselective inhibitors of cyclooxygenase 2. JAMA. 2006;296(13):1633–44.
Solomon SD, McMurray JJ, Pfeffer MA, Wittes J, Fowler R, Finn P, et al. Cardiovascular risk associated with celecoxib in a clinical trial for colorectal adenoma prevention. N Engl J Med. 2005;352(11):1071–80.
Bhala N, Emberson J, Merhi A, Abramson S, Arber N, Baron JA, et al. Vascular and upper gastrointestinal effects of non-steroidal anti-inflammatory drugs: meta-analyses of individual participant data from randomised trials. Lancet. 2013;382(9894):769–79.
Nissen SE, Yeomans ND, Solomon DH, Luscher TF, Libby P, Husni ME, et al. Cardiovascular safety of celecoxib, naproxen, or ibuprofen for arthritis. N Engl J Med. 2016;375(26):2519–29.
Ungprasert P, Srivali N, Kittanamongkolchai W. Non-steroidal anti-inflammatory drugs and risk of heart failure exacerbation: a systematic review and meta-analysis. Eur J Intern Med. 2015;26(9):685–90.
Gislason GH, Rasmussen JN, Abildstrom SZ, Schramm TK, Hansen ML, Fosbol EL, et al. Increased mortality and cardiovascular morbidity associated with use of nonsteroidal anti-inflammatory drugs in chronic heart failure. Arch Intern Med. 2009;169(2):141–9.
Arfe A, Scotti L, Varas-Lorenzo C, Nicotra F, Zambon A, Kollhorst B, et al. Non-steroidal anti-inflammatory drugs and risk of heart failure in four European countries: nested case-control study. BMJ. 2016;354:i4857.
Page J, Henry D. Consumption of NSAIDs and the development of congestive heart failure in elderly patients: an underrecognized public health problem. Arch Intern Med. 2000;160(6):777–84.
Feenstra J, Heerdink ER, Grobbee DE, Stricker BH. Association of nonsteroidal anti-inflammatory drugs with first occurrence of heart failure and with relapsing heart failure: the Rotterdam Study. Arch Intern Med. 2002;162(3):265–70.
Garcia Rodriguez LA, Hernandez-Diaz S. Nonsteroidal antiinflammatory drugs as a trigger of clinical heart failure. Epidemiology. 2003;14(2):240–6.
Mamdani M, Juurlink DN, Lee DS, Rochon PA, Kopp A, Naglie G, et al. Cyclo-oxygenase-2 inhibitors versus non-selective non-steroidal anti-inflammatory drugs and congestive heart failure outcomes in elderly patients: a population-based cohort study. Lancet. 2004;363(9423):1751–6.
Hudson M, Richard H, Pilote L. Differences in outcomes of patients with congestive heart failure prescribed celecoxib, rofecoxib, or non-steroidal anti-inflammatory drugs: population based study. BMJ. 2005;330(7504):1370.
Huerta C, Varas-Lorenzo C, Castellsague J, Garcia Rodriguez LA. Non-steroidal anti-inflammatory drugs and risk of first hospital admission for heart failure in the general population. Heart. 2006;92(11):1610–5.
Hudson M, Rahme E, Richard H, Pilote L. Risk of congestive heart failure with nonsteroidal antiinflammatory drugs and selective cyclooxygenase 2 inhibitors: a class effect? Arthritis Rheum. 2007;57(3):516–23.
Schneeweiss S, Sturmer T, Maclure M. Case-crossover and case-time-control designs as alternatives in pharmacoepidemiologic research. Pharmacoepidemiol Drug Saf. 1997;6(Suppl 3):S51–9.
Maclure M, Mittleman MA. Should we use a case-crossover design? Annu Rev Public Health. 2000;21:193–221.
Maclure M. The case-crossover design: a method for studying transient effects on the risk of acute events. Am J Epidemiol. 1991;133(2):144–53.
Corrao G, Ghirardi A, Ibrahim B, Merlino L, Maggioni AP. Burden of new hospitalization for heart failure: a population-based investigation from Italy. Eur J Heart Fail. 2014;16(7):729–36.
Yang HY, Chiu WC, Huang JH, Hsu CY, Lin YK, Chen YJ. Analysis of 10-year nationwide population-based data on sex differences in hospitalization for heart failure. Heart Vessels. 2013;28(6):721–7.
Arfe A, Corrao G. The lag-time approach improved drug-outcome association estimates in presence of protopathic bias. J Clin Epidemiol. 2016;78:101–7.
Suissa S. The case-time-control design. Epidemiology. 1995;6(3):248–53.
Suissa S. The case-time-control design: further assumptions and conditions. Epidemiology. 1998;9(4):441–5.
Hallas J, Pottegard A, Wang S, Schneeweiss S, Gagne JJ. Persistent user bias in case-crossover studies in pharmacoepidemiology. Am J Epidemiol. 2016;184(10):761–9.
US Food and Drug Administration. Public Health Advisory—FDA announces important changes and additional warnings for COX-2 selective and non-selective non-steroidal anti-inflammatory drugs (NSAIDs). 2005. https://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm150314.htm. Accessed 22 May 2017.
Oliveri L, Jerzewski K, Kulik A. Black box warning: is ketorolac safe for use after cardiac surgery? J Cardiothorac Vasc Anesth. 2014;28(2):274–9.
Kimmel SE, Berlin JA, Kinman JL, Hennessy S, Feldman H, Carson JL, et al. Parenteral ketorolac and risk of myocardial infarction. Pharmacoepidemiol Drug Saf. 2002;11(2):113–9.
Combe B, Swergold G, McLay J, McCarthy T, Zerbini C, Emery P, et al. Cardiovascular safety and gastrointestinal tolerability of etoricoxib vs diclofenac in a randomized controlled clinical trial (The MEDAL study). Rheumatology (Oxford). 2009;48(4):425–32.
De Vecchis R, Baldi C, Di Biase G, Ariano C, Cioppa C, Giasi A, et al. Cardiovascular risk associated with celecoxib or etoricoxib: a meta-analysis of randomized controlled trials which adopted comparison with placebo or naproxen. Minerva Cardioangiol. 2014;62(6):437–48.
Patrono C, Baigent C. Nonsteroidal anti-inflammatory drugs and the heart. Circulation. 2014;129(8):907–16.
Anwar A, Anwar IJ, Delafontaine P. Elevation of cardiovascular risk by non-steroidal anti-inflammatory drugs. Trends Cardiovasc Med. 2015;25(8):726–35.
Cheng CL, Kao YH, Lin SJ, Lee CH, Lai ML. Validation of the National Health Insurance Research Database with ischemic stroke cases in Taiwan. Pharmacoepidemiol Drug Saf. 2011;20(3):236–42.
Cheng CL, Lee CH, Chen PS, Li YH, Lin SJ, Yang YH. Validation of acute myocardial infarction cases in the national health insurance research database in taiwan. J Epidemiol. 2014;24(6):500–7.
Cheng CL, Chien HC, Lee CH, Lin SJ, Yang YH. Validity of in-hospital mortality data among patients with acute myocardial infarction or stroke in National Health Insurance Research Database in Taiwan. Int J Cardiol. 2015;201:96–101.
Acknowledgements
We thank the National Health Insurance Administration (NHIA) and National Health Research Institutes (NHRI) for making the databases used in this study available. However, the content of this article does not represent any official position of the NHIA or NHRI. The authors had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This work was supported by the Ministry of Science and Technology, Taiwan (Grant No. MOST104-2410-H-002-225-MY3). The funding source had no role in conducting this study, including the study design, data collection and analysis, manuscript preparation and review, or decision to submit the manuscript for publication.
Ethical Approval
The identification numbers for all of the entries in the NHIRD are encrypted to ensure privacy. The study protocol was approved by the Research Ethics Committee of the National Taiwan University Hospital (NTUH-REC-201403069 W).
Conflicts of Interest
Sung-Po Huang, Yao-Chun Wen, Shih-Tsung Huang, Chih-Wan Lin, Tzung-Dau Wang, and Fei-Yuan Hsiao have no conflicts of interest that are directly relevant to the content of this study.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Huang, SP., Wen, YC., Huang, ST. et al. Nonsteroidal Anti-Inflammatory Drugs and Risk of First Hospitalization for Heart Failure in Patients with No History of Heart Failure: A Population-Based Case-Crossover Study. Drug Saf 42, 67–75 (2019). https://doi.org/10.1007/s40264-018-0720-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40264-018-0720-9