
Abstract
Available evidence supports the efficacy of pre-exposure prophylaxis (PrEP) in decreasing the incidence of human immunodeficiency virus (HIV) infection among high-risk individuals, especially when used in combination with other behavioural preventive methods. Safety concerns about PrEP present challenges in the implementation and use of PrEP. The aim of this review is to discuss safety concerns observed in completed clinical trials on the use of PrEP. We performed a literature search on PrEP in PubMed, global advocacy for HIV prevention (Aids Vaccine Advocacy Coalition) database, clinical trials registry “http://www.clinicaltrials.gov” and scholar.google, using combination search terms ‘pre-exposure prophylaxis’, ‘safety concerns in the use of pre-exposure prophylaxis’, ‘truvada use as PrEP’, ‘guidelines for PrEP use’, ‘HIV pre-exposure prophylaxis’ and ‘tenofovir’ to identify clinical trials and literature on PrEP. We present findings associated with safety issues on the use of PrEP based on a review of 11 clinical trials on PrEP with results on safety and efficacy as at April 2016. We also reviewed findings from routine real-life practice reports. The pharmacological intervention for PrEP was tenofovir disoproxil fumarate/emtricitabine in a combined form as Truvada® or tenofovir as a single entity. Both products are efficacious for PrEP and seem to have a good safety profile. Regular monitoring is recommended to prevent long-term toxic effects. The main adverse effects observed with PrEP are gastrointestinal related; basically mild to moderate nausea, vomiting and diarrhea. Other adverse drug effects worth monitoring are liver enzymes, renal function and bone mineral density. PrEP as an intervention to reduce HIV transmission appears to have a safe benefit-risk profile in clinical trials. It is recommended for widespread use but adherence monitoring and real-world safety surveillance are critical in the post-marketing phase to ensure that the benefits observed in clinical trials are maintained in real-world use.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Safety concerns about pre-exposure prophylaxis pose challenges in use that should not be overlooked. |
Behavioural counselling and assurance of safety and efficacy are important components of pre-exposure prophylaxis. |
Real-world safety surveillance is critical in the post-marketing phase to ensure that the benefits observed in clinical trials are maintained. |
1 Introduction
At the end of 2015, the World Health Organization established that 36.7 million people were living with human immunodeficiency virus (HIV) with about 2.1 million becoming newly infected in the year [1]. With this high prevalence of HIV/acquired immune deficiency syndrome in the world, the World Health Organization related the urgency and importance of novel, effective and safe interventions in the prevention of HIV infection. This became necessary in that preventive behavioural messages on abstinence, faithfulness and condom use presented useful but limited impact as primary prevention on the spread of HIV. This challenge is observed especially among people at high risk because these protective measures were not applied consistently [2].
Human immunodeficiency virus continues to be a major public health problem and it has claimed more than 35 million lives so far. In 2015 alone, 1.1 million died from HIV-related causes worldwide [1]. The various management options for HIV including treatment, post-exposure prophylaxis and prevention of mother-to-child transmission have been integral in lowering HIV incidence, but reaching out to individuals at substantial risk owing to lifestyle practices required newer specific preventive approaches. Pre-exposure prophylaxis (PrEP) is a powerful tool in curbing the transmission of HIV infection [3], and it involves taking an antiretroviral (ARV) pill daily in addition to other preventive behavioural measures to prevent HIV infection. This is a protective mechanism used for individuals not diagnosed with HIV but who may be at substantial risk of becoming infected because of their lifestyle or as a partner in a sero-discordant relationship.
Results from clinical trials demonstrate the efficacy of PrEP, either used alone or in combination with other behavioural preventive methods, where it has been shown that PrEP can reduce the incidence of HIV by up to 86% [4, 5] or even more with strict adherence. Based on results and evidence from PrEP trials, the US Food and Drug Administration (FDA) on 16 July, 2012 approved Truvada® [tenofovir (TDF) 300 mg/emtricitabine (FTC) 200 mg] (Gilead Sciences Inc., Foster City, CA, USA) as an effective medication for the prevention of HIV that could be sexually acquired [6, 7] and in all other types of possible HIV infection including injectable drug use. This was followed with guidelines for the provision of PrEP in clinical settings issued by the US Centers for Disease Control (CDC) and recently the World Health Organization also issued similar guidelines recommending PrEP as a prevention option for individuals at substantial risk for acquiring HIV [8, 9].
In the 2014 CDC guidelines, TDF alone based on positive results of substantial efficacy and safety in clinical trials with injectable drug use and heterosexual active adults was recommended as an alternative regimen for these populations, but not for men who have sex with men (MSM) because no efficacy studies were concluded as yet in the group. Again, the use of other antiretroviral medications for PrEP, either in place of or in addition to TDF/FTC or TDF alone is not recommended and finally the use of oral PrEP for sex activity-timed or noncontinuous daily use is also not recommended [8]. The CDC also recommend in addition to regular follow-up testing for changes in HIV-negative status and adverse drug monitoring including renal function before the initiation of PrEP and regularly while on preventive therapy. Routine bone mineral density (BMD) monitoring was not recommended by the CDC [8].
There are several challenges in the implementation and use of PrEP. These concerns include high costs, safety screening, toxicity arising from continuous use, adverse drug reactions, poor adherence, possible abuse and the fear of decreased condom use as an additional protective method [10, 11]. Poor adherence during PrEP is especially an important factor that may reduce effectiveness and lead to an increase in HIV infection rate with a possible development of HIV-resistant strains and subsequent transfer among the population. Factors that can affect adherence include adverse drug reactions (at regular doses) or toxicity (adverse drug reactions at probable high, intolerant doses or long-term use).
The ARV drugs presently recommended for oral PrEP are TDF or a combination of TDF/FTC. These medications have proven to be potent [12–14], have a favourable resistance profile and are claimed to have limited adverse effects, thus rendering them efficacious and safe for PrEP [14–17]. Some studies have also assessed the efficacy of a 1% vaginal gel formulation of TDF and found it to be effective in reducing HIV transmission by 39% [18]. Essential factors to be considered before using PrEP include a confirmed HIV-negative status with a normal renal function, a negative hepatitis B status, and absence of reduced BMD or a history of bone fractures, bone loss and osteoporosis [19, 20]. Recipients of PrEP also need to be tested on a minimum of a quarterly basis during follow-up to ensure they remain HIV negative, do not present with decreased estimated creatinine clearance levels or reductions in BMD [21]. The aim of this review is to describe and discuss safety concerns on the use of PrEP in the literature. Results from this review will contribute to the growing knowledge on the safety profile or use of PrEP.
2 Methods
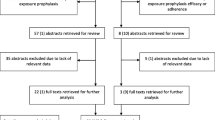
We performed a search of the literature on PrEP in PubMed (search date: 10 May, 2016), scholar.google (search date: 11 May, 2016), global advocacy for HIV prevention (Aids Vaccine Advocacy Coalition) database (search date: 12 May, 2016) and the clinical trials, “http://www.clinicaltrials.gov” (search date: 13 May, 2016), using combination search terms ‘pre-exposure prophylaxis’, ‘safety concerns in the use of pre-exposure prophylaxis’, ‘truvada use as PrEP’, ‘guidelines for PrEP use’, ‘HIV pre-exposure prophylaxis’ and ‘tenofovir’ to identify literature on PrEP safety trials and issues. The coverage dates were from January 2001 to April 2016. We limited the search to articles in English, which were completed with results available and based on the safety or efficacy of TDF, FTC and TDF/FTC. We profiled our findings on safety concerns of PrEP. Information on clinical trials was extracted from PubMed, Aids Vaccine Advocacy Coalition and clinicaltrials.gov based on completed studies (Fig. 1).

Chart of search strategy for clinical trials on pre-exposure prophylaxis based on tenofovir (TDF), emtricitabine (FTC) and a TDF/FTC combination. AVAC Aids Vaccine Advocacy Coalition
In the clinical trials database, studies that were enrolling or incomplete at the time of this review were excluded. Seventy-two cases were retrieved. We modified the search for closed and completed studies and reduced the number to 42. Further modification with emphasis on the drugs of interest reduced the trials to 23. We then isolated nine studies that were complete with results and enough data for our review (Fig. 1).
In PubMed, we obtained 938 articles after the initial search. We then limited the search to only clinical trials and obtained 79. We then modified to include only trials involving TDF/FTC and TDF and got 35 articles. From here, we isolated 29 articles that were completed and had results. We then focused on efficacy and safety, and retrieved nine articles.
For AVAC, the initial search on PrEP and then clinical trials and product development yielded 38 articles; we then selected completed studies and obtained 14 articles. We then modified to focus on efficacy and safety and isolated eight articles. We then isolated 11 studies that appeared in all three search engines that satisfied our review requirements and used these for our review and discussion (Fig. 1).
3 Results
3.1 Clinical Trials Supporting the Use of PrEP
Numerous trials involving both humans and animals have tested oral and vaginal routes of administration of PrEP and have been found efficacious in preventing HIV. The basis for PrEP stems from results of clinical and epidemiological research [22–25]. We reviewed 11 clinical trials on PrEP among different risk groups conducted from 2005 to 2015. These trials had results at the time of our study and allowed for review. Results from literature on PrEP studies are not necessarily universal. The efficacy ranges from lack of protection to protection levels of as high as 96%, attesting to the complex nature of PrEP implementation [26]. Aside from the effectiveness of PrEP in most of the studies cited, the Vaginal and Oral Interventions to Control the Epidemic (VOICE) [27] and Preexposure Prophylaxis Trial for HIV Prevention among African Women (FEM-PrEP) [28] studies were terminated ahead of time because the analysis failed to demonstrate efficacy attributed to poor adherence. Results for the VOICE study differ with findings in three other placebo-controlled vaginal PrEP trials [Partners PrEP [14], TDF2 [17], Iniciativa Profilaxis Pre-Exposicion (iPrEx) and [16] one placebo-controlled vaginal gel trial [Centre for AIDS program of Research in South Africa (CAPRISA 004)] [18]. Partners PrEP [14] studied Truvada® and TDF alone in HIV-discordant committed African couples, TDF2 [17] studied heterosexual African women and men, iPrEx [16] studied gay and bisexual men on four continents and CAPRISA 004 [18] studied South African women. Poor adherence as in FEM-PrEP was the main reason for failure in all three VOICE arms. Among 334 women who became infected with HIV, 22 entered the trial with acute HIV infection. With their exclusion, HIV incidence was 5.7 per 100 person-years, meaning about 6 in every 100 women got infected in every 12 months. HIV incidence rates per 100 person-years were 6.3 and 4.2 for oral TDF vs. placebo, 4.7 and 4.6 for Truvada® vs. placebo, and 5.9 and 6.8 for TDF gel vs. placebo; therefore, none of the three strategies worked as hazard ratios (HRs) was for oral TDF: HR 1.49 [95% confidence interval (CI) 0.97–2.29], oral Truvada®: HR 1.04 (95% CI 0.73–1.49) and TDF gel: HR 0.85 (95% CI 0.6–1.2). In all cases, women reported 90–91% adherence with return data suggesting the same, but TDF concentrations in plasma told another story: 30% or fewer women in all three treatment arms had detectable concentrations in plasma: 30% in oral TDF, 29% in oral Truvada® and 25% using TDF gel. In all three again, 50% or more women never had detectable blood in any sample. Three factors predicted detectable TDF in plasma: first, being married (adjusted odds ratio = 2.24 [95% CI, 1.12–4.49]), the second being older than 25 years (adjusted odds ratio = 1.62 [95% CI, 1.12–2.34]), and the third being multiparous (adjusted odds ratio = 1.84 [95% CI, 1.26–2.69]).
The FEM-PrEP [28] study of 2120 participants reported 56 new HIV infections 14 months after initiation of the study with the infections equally distributed between Truvada® and placebo groups (28 in each arm), clearly indicating the lack of protection in the use of Truvada®. Overall adherence (based on participants self-report) was 95% with no clear difference in adherence between the two arms.
These two results revealed that “products that are long acting and require minimum daily adherence may be more suitable for the population under study” contrary to positive results posted by the other findings, which suggest that young, sexually active, single people can be motivated to take oral Truvada® or TDF gel regularly enough to protect themselves from HIV. However, the CAPRISA 004 trial [18] differed from the FEM-PrEP [28] and VOICE [27] studies by determining a 65% protection against HIV at a TDF concentration of >100 ng/mL and up to 76% with a TDF concentration of >1000 ng/mL. Results from Pre-exposure Prophylaxis to Prevent the Acquisition of HIV-1 Infection (PROUD) [29] in the UK and Intervention Preventive de l’Exposition aux Risques avec Risques avec et pour les Gays (Ipergay) [5] in France both showed that PrEP reduced infections among gay men by 86%. None of the participants on PrEP involved in these studies acquired HIV. PrEP was also found to be effective for heterosexual men and women: a study in East Africa (Partners) [14] reduced possible HIV infection within couples in which one partner was positive by 75%. The iPrEx study also found that the HIV infection rate in HIV-negative gay men who were given a daily pill containing Truvada® was reduced by 44%, compared with men given placebo. Those who confirmed adherence at 90% had a reduction rate of up to 73%. The TDF2 trial in Botswana gave a reduction rate of 63% against placebo and 77.9% after secondary analysis; therefore, confirming the obvious benefit in the use of PrEP. The Bangkok Tenofovir Study [30] focused on men and women who inject drugs and found that the risk of acquiring HIV reduced by 49% and up to 79% in those who adhered consistently to their medication. The study also found that participants taking TDF were more likely to experience nausea and or/vomiting than those in the placebo group. No indication of elevated creatinine or renal impairment in the TDF group was reported.
The PrEP study in USA with 373 participants with 186 taking TDF and 187 taking placebo was successful with [31] only four on placebo and three among the delayed-arm participants seroconverting. Estimated adherence by pill load was 92% and by medication event monitoring system was 77%. Oral TDF was well tolerated with no significant renal concerns, while adverse drug events reported did not differ significantly between TDF and placebo arms.
Sensitivity analysis on oral PrEP demonstrated that both TDF/FTC and TDF are efficacious in the prevention of HIV infection for a variety of high-risk populations irrespective of country [32, 33]. Both daily and intermittent dosing of PrEP have proven effective and safe [15]. Pharmacokinetic modelling of the pre-exposure prophylaxis initiative (iPrEx) data revealed that a PrEP dose regimen of 7 days in the week dosing could achieve as high as 99% efficacy in the prevention of HIV infection among MSM. Additionally, an intermittent dosing of 4 days in the week could result in 96% efficacy [15]. In a laboratory analysis, detectable blood concentrations of medications used for PrEP were consistently associated with a protective effect against HIV acquisition [16].
3.2 Safety Concerns
Adverse reactions to medications used for any intervention are undoubtedly a primary safety concern irrespective of the duration of use. A qualitative study of gay and bisexual sero-discordant male couples assessed the concerns for adoption of PrEP and revealed that the main concerns and probable barriers to adoption of PrEP were short- and long-term side effects or adverse effects due to intermittent dosing or early termination of drug use aside from cost and accessibility of the drugs [34]. In this review, we acknowledge that the trials discussed are short term and do not give the opportunity to assess the long-term, real-world safety profile of the products used for PrEP. Pre-exposure prophylaxis is premised on ARV medications that have been used by people living with HIV and AIDS for quite some time now, since the inception of ARVs. We would expect based on current evidence that the long-term safety profile will be within acceptable limits with favourable benefit-risk profiles, considering the impact of PrEP on HIV prevention. Nonetheless, established adverse drug events such as renal impairment, reduction in BMD, and gastrointestinal (GI) disturbances captured in scientific literature concerning the use of TDF should be considered and monitoring is recommended in PrEP use. An earlier study by the same authors on the association between the occurrence of adverse drug events and the modification of first-line highly active antiretroviral therapy in Ghanaian patients established that adverse drug events play a major role in treatment modification and could be used as a predictor for possible therapy modification [35].
Other concerns on the use and implementation of PrEP include resistance to PrEP medications, feasibility, acceptability and very importantly adherence to PrEP regimens. Because of the importance of PrEP in reducing the spread of HIV, it is critical that these concerns are addressed and fears alleviated to allow for the promising potential of PrEP. The US Public Health Service recommended guidelines for the use of PrEP in 2014 [21] and the CDC has interim guidelines for clinicians on the use of PrEP [36]. Essential factors to be considered before using PrEP include a confirmed HIV-negative status with a normal renal function and a negative hepatitis B status [19, 20]. Recipients of PrEP should be at high risk for HIV infection, receive behavioural and adherence counselling, and need to be tested on a minimum of a quarterly basis during follow-up to ensure they remain HIV negative [21, 36].
3.3 Adverse Effects
The TDF/FTC (Truvada®) combination or TDF alone used for PrEP generally shows a tolerable profile. In most studies, the experienced side effects did not differ significantly from rates among participants taking placebo. The side effects or adverse events are basically of GIT origin and more prevalent at the start of use, but subside within a month of use. The GIT disturbances are generally upset abdominal pain, nausea, vomiting or diarrhoea. Other reported adverses events not of GIT origin are dizziness, headache, fatigue, weight loss, shortness of breath, cough, anxiety, fever or joint and muscle pain. In most studies, these side effects or adverse events did not differ significantly from rates among participants taking placebo.
Risk factors in long-term use include age, duration of treatment with TDF, elevated baseline creatinine levels, and treatment with a protease inhibitor boosted with ritonavir combinations and among persons with African descent as against Caucasians [37]. Side effects considered potentially serious in the daily use of Truvada® or TDF for PrEP are liver function problems, kidney damage, hypophosphatamia, proteinaemia or glucosuria, pancreatitis, bone thinning and lactic acidosis. Flu-like symptoms, hypertriglyceridemia, increased creatinine phosphokinase, unusual dreams and hyperpigmentation are associated with the use of FTC. The Partners PrEP safety trial [14], the iPrEx [16] and the Bangkok Tenofovir studies [30] all recorded increased serum creatinine levels but analyses indicated that they were statistically insignificant compared with placebo. However, changes in estimated glomerular filtration rate were associated with a small but statistically significant decline in the estimated glomerular filtration rate, which was non-progressive and resolved with TDF discontinuation. The use of TDF alone is also associated with liver and pancreatic problems as well as depression [38]. The iPrEx study found a modest effect on BMD reduction in men who participated in the study. The study compared changes in BMD between placebo group and study participants with blood concentrations of tenofovir diphosphate associated with 90% efficacy and use of two to three tablets per week. There was a decline of 1% in the hip and 1.8% in the spine by the end of the study in those with optimal TDF diphosphate concentrations but this reduced to normal levels after 1.5 years of stopping PrEP [16]. The loss of BMD could lead to potential bone fractures and is a problem for TDF-based PrEP. This could be because of phosphate wasting. TDF/FTC was well tolerated with some nausea but little difference was observed between participants and those taking placebo (9 vs. 5%). No differences in severe (grade 3) or life-threatening (grade 4) adverse laboratory events were observed between the active and placebo groups [8].
In the CAPRISA 004 study [18], hepatic flare (defined as an event with an abrupt rise of alanine aminotransferase levels to more than five times the upper limit of normal) during chronic hepatitis B virus infection and considered to be the result of a human leukocyte antigen-1 restricted, cytotoxic T lymphocyte-mediated immune response against hepatitis B virus [39] was observed for two hepatitis B carriers but this did not result in drug discontinuation. In the Partners-PrEP study [14], there were no significant differences across the study arms with respect to serious adverse effects including the total of 1% deaths per arm.
The US MSM safety trial [31] presented no marked difference in the overall frequency of adverse events between TDF and placebo groups, but in a subset of men at a San Francisco site (n = 184), the use of TDF was associated with a small but statistically significant decrease in BMD at the femoral neck (1.1%) and total hip (0.8% decrease) but no bone fractures were detected. Rates of nausea and vomiting were higher among the TDF than among placebo recipients in the first 2 months in the Bangkok Tenofovir Study [30] but not thereafter. The rates of adverse drug events, deaths or elevated creatinine were not different between the TDF and the placebo groups [30].
Concerning the trials with questionable efficacy, the FEM-PrEP trial [28] presented adverse drug events of nausea and vomiting, which were transient, and a mild elevation of liver enzymes was much more common with the TDF/FTC group than that of placebo group. No change in renal function was reported in either group. In the VOICE study [27], a confirmed increase in creatinine levels was observed in the oral TDF/FTC group than in the oral placebo group. There were no significant differences between the active products and placebo groups for other safety outcomes [27].
3.4 Resistance
Generally, resistance to PrEP is rarely observed in seroconverters who are infected with HIV after randomisation. Participants who show resistance are more likely to be the result of circulating resistance and not necessarily, PrEP induced. In the PROUD trial, no one acquired resistance to TDF [29]. Resistant virus reported in studies include one with TDF-resistant virus (K65R mutation) in a participant randomised to TDF and one with FTC-resistant virus (M184V mutation) in a participant randomised to FTC/TDF from the Partners-PrEP trial [14]. They were found to be infected at randomisation. A rare TDF resistance mutation (K65N) was however reported in the TDF arm of the Partners-PrEP study after randomisation [14]. In the TDF2 study, K65R, M184V and A62V resistance mutations occurred in one participant in the TDF/FTC group. The participant was later found to have had HIV infection at enrolment. The iPrEx study presented two of two men in the active group and one of eight in the placebo group with FTC-resistant virus. TDF/FTC resistant virus was detected in five women (one in the placebo group and four in the TDF/FTC group) in the FEM-PrEP study [28]. Two women from the TDF/FTC group who were determined after enrolment to have had acute HIV infection at baseline had the virus with the M1841/V mutation associated with FTC resistance. One other woman also had the M1841/V mutation but acquired the HIV infection after enrolment. The development of a resistant mutation seems to be more common with FTC than TDF. Additional care must be deployed to ensure that PrEP use is not approved during the acute infection stage to prevent the development of resistance strains. An abstract authored by Knox et al. presented at the CROI 2016 conference in Boston, MA, USA titled “HIV-1 infection with multiclass resistance despite PrEP” provided evidence of breakthrough HIV infection irrespective of long-term adherence to FTC/TDF (monitored via clinical and pharmacokinetic data) and described a resistant strain irrespective of long-term adherence [40]. It is described as the first such report and more efforts would be deployed to closely monitor the use of PrEP following this report.
The other area of concern is sexual and reproductive health because women of childbearing age are prone to HIV infection and the use of PrEP in discordant relationships could be useful. The Partners PrEP and the FEM-PrEP studies showed that TDF based PrEP does not affect the effectiveness of hormonal contraception and neither does hormonal contraception affect PrEP efficacy [14, 28]. There were not significant differences in pregnancy related and infant adverse reaction including premature births, congenital anomalies and growth throughout the early years of life for infants born to women who received PrEP as against placebo in the Partners PrEP study. Therefore, PrEP is relatively safe to be used by women of child-bearing age [14] though, like all medicines, its benefits should be weighed against any risks that it may pose in specific individuals.
3.5 Feasibility and Acceptability
Some research on behavioural tendencies has helped to determine adherence to PrEP, but few studies have assessed the acceptability and use of PrEP. Factors associated with intentions to use PrEP in a sample of men who have sex with men (MSM) in USA included the efficacy, costs and potential side effects of PrEP [41]. Preliminary findings from the PrEP Safety trial showed that MSM attending the STD clinic in San Francisco had a high interest in taking PrEP. This trial also demonstrated feasibility of including PrEP in busy clinical settings, indicating that PrEP can be accessed at clinics providing HIV care management [42]. Project PrEP, a study on the acceptability and feasibility of PrEP among young men who have sex with men, reported of high feasibility and acceptability of PrEP [43]. The PROUD study also affirmed the feasibility of incorporating PrEP in routine activities of clinical settings [29]. Acceptability of PrEP as demonstrated in a study among MSM and female sex workers in Nairobi and Mtwapa, Kenya, was also rated as high [44]. Suggestions proposed in this study included how best to improve the pill characteristics to make it easy to take, how to reduce stigma and discrimination from other family members, certain barriers and facilitators to adhering to PrEP regimens such as lifestyles, dosing regimen and side effects were identified. Enhanced counselling and commitment to using the products also improved their ability to adhere to the regimens despite the challenges.
Participants in all the listed studies were receptive to monthly HIV testing and counselling, risk reduction counselling, physical examinations and group-based intervention sessions. Participants were more likely to accept a daily pill compared with multiple daily pills administration, especially if they knew their partner was not infected [43]. The Ipergay trial demonstrated that high-risk MSM who do not use condoms consistently, accepted on demand PrEP as a practical alternative to daily PrEP if its effective [5]. A substudy of The Alternative Dosing to Augment Pre-Exposure Prophylaxis Pill Taking [45] study involving 37 men in Harlem revealed scepticism and distrust by male partners and sometimes resulted in unwillingness of partners to engage in sex after learning about their PrEP use, thus pointing out how stigma and social barriers may impede adherence and therefore acceptability.
3.6 Adherence
Six clinical trials yielded PrEP efficacy estimates of 0–75% mostly because of differences in adherence among the studies [14, 16, 17]. Self-reported adherence to PrEP is unreliable as the initial clinical trials quickly established that blood drug concentrations sharply differ from perceived adherence claims. Effective counselling and other support measures are required in all persons who desire to use PrEP for HIV prevention.
The iPrEx study [16] clearly illustrated how adherence produced different outcomes in HIV-negative gay men who were given a daily pill of TDF and FDC and achieved a reduction rate of 44% as against men given a placebo. It was realised that subjects who by self-report and pill count took the drugs more than 90% of the time reduced the infection rate by 73% [16]. Meanwhile, another interesting finding of the trial indicated that while 93% of trial subjects reported complete compliance, only 51% actually complied effectively when drug concentrations in blood were determined [16]. The investigators concluded through calculations that a reduction in the risk of HIV infection could have been as much as 92% compared with placebo if the study subjects had complied totally [16]. This confirms the importance of adherence as a major tool to be deployed in PrEP. The FEM-PrEP trial [28], which was halted for futility, reported adherence by self-report and pill count as high, but plasma drug concentrations showed that only 15–26% of samples from HIV seroconverters had detectable concentrations of serum TDF and only 26–38% of non-seroconverting controls. This low level of adherence was recorded as 37% (Table 1) by the researchers and this may have resulted in the inability to assess the protective effect of Truvada® in FEM-PrEP trial. This again points to the importance of ensuring adherence in PrEP management.
Liu et al. [42], examined self-reported medication-taking experiences, facilitators and barriers of medication adherence among a geographically diverse online sample of HIV-uninfected MSM in US. Their multivariable analyses showed that age and sex were likely associated with adherence. In this study, 1480 men having sex with other men were surveyed, 806 (54%) of participants indicated regular taking of medicines, 80% of this number reported taking medicines for treatment whilst 55% said they take medicines for preventive purposes. The study also realised that men aged older than 25 years were more likely to report excellent adherence together with those who did not report any adherence barriers. Willingness to use PrEP was also associated with high likelihood of reporting perfect 30-day adherence. They listed factors that improved medication adherence as establishing a routine, keeping medication visible and using a pill-box. Forgetfulness, changes in usual routine, and being busy or away from home were listed as barriers to adherence [42]. Counselling strategies to build pill-taking routines can help improve adherence to PrEP. Daily dosing are much more associated with a high level of adherence than post-coital use of PrEP, which is generally low [15].
Following the approval of the use of PrEP in USA and Europe, reports on adherence have been claimed to be higher in recent trials and open label extensions as compared with the initial clinical trials. Explanations provided include available evidence of PrEP efficacy and individual motivations and reasons for taking PrEP [46].
4 Discussion
The advent of PrEP is a promising turning point in the prevention of HIV among at-risk groups. TDF-based PrEP is recommended to prevent HIV infection in tandem with other preventive measures. From the trials reviewed, it is evident that PrEP is highly effective against HIV infection when taken as required. Most importantly, PrEP seems to be characterised by low adverse effects. Our current review shows a favourable pattern of adverse events for PrEP among eligible populations. Side effects can lead to a lack of compliance, resulting in low levels of adherence (frequency of medicine intake) to pill use. Some reported symptoms associated with the start of PrEP gradually resolve. Generally, even for some side effects listed as serious, such as kidney dysfunction, observed increases in the serum creatinine level return to normal after the discontinuation of PrEP. Tubular renal toxicity from PrEP is rare and active screening is not recommended. The same applies to the reduction of BMD after cessation in the use of TDF and therefore current evidence does not support constant X-ray monitoring at baseline before initiating PrEP and while taking TDF/FTC.
Liver toxicity mentioned earlier in the findings was reported by the D.A.D. study, which looked at the use of antiretroviral therapy and the risk of end-stage liver disease and hepatocellular carcinoma in HIV-positive persons. It concluded among that alongside other antiretroviral agents, TDF is associated with an increased risk of end-stage liver disease among HIV-positive patients on long-term therapy. It also indicated that the unexpected viral hepatitis independent TDF association should be investigated further [47]. The use of TDF-based PrEP is yet to present any case report involving serious hepatic complications. However, the regular monitoring of liver enzymes in PrEP uses would be helpful in preventing possible toxicities.
The correspondent decrease in sexual risk behaviour among participants in the course of PrEP is very encouraging. This is attributed to behavioural intervention including sexual health counselling and the provision of condoms across the studies where applicable. Undoubtedly, behavioural interventions should be an integral part of PrEP.
Because PrEP is meant for HIV-negative individuals, an important aspect of PrEP is the identification of people who are seroconverting [14]. Preliminary testing methods, for example polymerase chain reaction that can diagnose people who are recently infected with HIV, are thus important but expensive. This will enable provision of treatment options instead of preventive interventions.
Exclusion criteria that run across trials were the low level of creatinine clearance below 50 mL/min, some cases of hepatitis and evidence of bone fractures. People who do not qualify for PrEP but are at risk for HIV should be encouraged to adhere to good evidence-based sexual behavioural prevention practices including regular condom use. The reduction in rates of sex without condoms from 27 to 9% after 24 months of the Partners-PrEP trial [14] is encouraging and shows that counselling and education on good sexual practices is complementary on HIV prevention. Several other studies [48–51], including studies conducted in West African women with TDF, also demonstrate a reduction in high-risk sexual behaviour with counselling during PrEP [52]. TDF/FTC is the only medication with a label indication as PrEP against HIV infection, but new PrEP drugs and formulations are being considered for future trials (Maraviroc, intravaginal rings containing dapivirine and TDF) and long-acting injectables (rilpivirine, carbotegravir). These newer agents also present a good safety profile when used for the treatment of HIV infection, but use for PrEP purposes in HIV-uninfected persons is unknown as efficacy and clinical safety is yet to be established [37]. A new formulation, tenofovir alafenamide that provides 90% lower plasma levels of TDF concentrations compared with standard TDF, has recently being approved by the FDA. It is claimed to have favourable renal and bone safety profile better than original TDF, unfortunately as at the time of this review efficacy and safety in PrEP has not been established in HIV-negative populations [37].
5 Conclusion
The medications currently studied for PrEP (TDF and FTC) are efficacious and seem to have a good safety profile within the average short period of 3 years studied. Emphasis on the use of additional prevention methods should be made alongside. The main adverse effects observed with PrEP are GI related and graded below 2 for severity. These are basically mild to moderate nausea, vomiting and diarrhea. Major concerns are renal, hepatic and bone toxicity, but these are transient and non-progressive and quickly resolved after discontinuation of TDF. Overall, the benefit-risk profiles of the products used for PrEP appear favourable.
PrEP as an intervention to reduce HIV transmission appears to have a safe benefit-risk profile in clinical trials. It is recommended for widespread use but adherence monitoring and real-world safety surveillance are critical in the post-marketing phase to ensure that the benefits observed in clinical trials are maintained in real-world use. Behavioural counselling and assurance of safety and efficacy are important components of PrEP. Other factors of PrEP implementation that have been suggested include improving access, averting stigma, cost effectiveness, and education on PrEP to improve knowledge and assure people of the efficacy profile of products used for PrEP. Further studies must ultimately look at how safe and beneficial PrEP could be for pregnant women and women seeking to get pregnant.
References
UNAIDS. 2015 facts sheet. Geneva: WHO; 2016. http://www.unaids.org/sites/default/files/media_asset/20150901_FactSheet_2015_en.pdf. Accessed 3 June 2016.
Weinhardt LS, Carey MP, Johnson BT, Bickham NL. Effects of HIV counseling and testing on sexual risk behavior: a meta-analytic review of published research, 1985–1997. Am J Public Health. 1999;89(9):1397–405.
Castilla J, Del Romero J, Hernando V, et al. Effectiveness of highly active antiretroviral therapy in reducing heterosexual transmission of HIV. J Acquir Immune Defic Syndr. 2005;40(1):96–101.
Kirby T, Thornber-Dunwell M. Uptake of PrEP for HIV slow among MSM. Lancet. 2014;383(9915):399–400.
Molina JM, Capitant C, Spire B, et al. On-demand preexposure prophylaxis in men at high risk for HIV-1 infection. N Engl J Med. 2015;373(23):2237–46.
Holmes D. FDA paves the way for pre-exposure HIV prophylaxis. Lancet. 2012;380(9839):325.
US Food and Drug Administration. FDA approves first drug for reducing the risk of sexually acquired HIV infection. Silver Spring, Maryland: US Food and Drug Administration. 2012.
Centres for Disease Control and Prevention. Preexposure prophylaxis for the prevention of HIV infection in the United States. Atlanta, Georgia: Centres for Disease Control and Prevention. 2014.
World Health Organization. Guideline on when to start antiretroviral therapy and on pre-exposure prophylaxis for HIV. Geneva: World Health Organization; 2015. ISBN: 9789241509565. http://www.who.int/hiv/pub/guidelines/earlyrelease-arv/en/. Accessed 6 June 2016.
Underhill K, Operario D, Skeer M, et al. Packaging PrEP to prevent HIV: an integrated framework to plan for pre-exposure prophylaxis implementation in clinical practice. J Acquir Immune Defic Syndr. 2010;55(1):8.
Arnold EA, Hazelton P, Lane T, et al. A qualitative study of provider thoughts on implementing pre-exposure prophylaxis (PrEP) in clinical settings to prevent HIV infection. PLoS One. 2012;7(7):e40603.
Louissaint NA, Cao Y-J, Skipper PL, et al. Single dose pharmacokinetics of oral tenofovir in plasma, peripheral blood mononuclear cells, colonic tissue, and vaginal tissue. AIDS Res Hum Retrovir. 2013;29(11):1443–50.
Anderson PL, Kiser JJ, Gardner EM, et al. Pharmacological considerations for tenofovir and emtricitabine to prevent HIV infection. J Antimicrob Chemother. 2011;66(2):240–50.
Baeten JM, Donnell D, Ndase P, et al. Antiretroviral prophylaxis for HIV prevention in heterosexual men and women. N Engl J Med. 2012;367(5):399–410.
Kibengo FM, Ruzagira E, Katende D, et al. Safety, adherence and acceptability of intermittent tenofovir/emtricitabine as HIV pre-exposure prophylaxis (PrEP) among HIV-uninfected Ugandan volunteers living in HIV-serodiscordant relationships: a randomized, clinical trial. PLoS One. 2013;8(9):e74314.
Grant RM, Lama JR, Anderson PL, et al. Preexposure chemoprophylaxis for HIV prevention in men who have sex with men. N Engl J Med. 2010;363(27):2587–99.
Thigpen MC, Kebaabetswe PM, Paxton LA, et al. Antiretroviral preexposure prophylaxis for heterosexual HIV transmission in Botswana. N Engl J Med. 2012;367(5):423–34.
Sokal DC, Karim QA, Sibeko S, et al. Safety of tenofovir gel, a vaginal microbicide, in South African women: results of the CAPRISA 004 trial. Antivir Ther. 2013;18(3):301–10.
Smith DK, Thigpen MC, Nesheim SR, et al. Interim guidance for clinicians considering the use of preexposure prophylaxis for the prevention of HIV infection in heterosexually active adults. MMWR Morb Mortal Wkly Rep. 2012;61(31):586–9.
Smith D, Grant R, Weidle P, et al. Interim guidance: preexposure prophylaxis for the prevention of HIV infection in men who have sex with men. MMWR Morb Mortal Wkly Rep. 2011;60(3):65–8.
CDC. Control CfD, prevention. Preexposure prophylaxis for the prevention of HIV infection in the United States–2014: a clinical practice guideline. Atlanta (GA): CDC; 2014.
Celum CL, Robinson NJ, Cohen MS. Potential effect of HIV type 1 antiretroviral and herpes simplex virus type 2 antiviral therapy on transmission and acquisition of HIV type 1 infection. J Infect Dis. 2005;191(Suppl. 1):S107–14.
Derdelinckx I, Wainberg MA, Lange JM, et al. Criteria for drugs used in pre-exposure prophylaxis trials against HIV infection. PLoS Med. 2006;3(11):e454.
Liu AY, Grant RM, Buchbinder SP. Preexposure prophylaxis for HIV: unproven promise and potential pitfalls. JAMA. 2006;296(7):863–5.
Cardo DM, Culver DH, Ciesielski CA, et al. A case-control study of HIV seroconversion in health care workers after percutaneous exposure. N Engl J Med. 1997;337(21):1485–90.
Cohen MS, Baden LR. Preexposure prophylaxis for HIV: where do we go from here? N Engl J Med. 2012;367(5):459–61.
Marrazzo JM, Ramjee G, Richardson BA, et al. Tenofovir-based preexposure prophylaxis for HIV infection among African women. N Engl J Med. 2015;372(6):509–18.
Van Damme L, Corneli A, Ahmed K, et al. Preexposure prophylaxis for HIV infection among African women. N Engl J Med. 2012;367(5):411–22.
McCormack S, Dunn DT, Desai M, et al. Pre-exposure prophylaxis to prevent the acquisition of HIV-1 infection (PROUD): effectiveness results from the pilot phase of a pragmatic open-label randomised trial. Lancet. 2016;387(10013):53–60.
Choopanya K, Martin M, Suntharasamai P, et al. Antiretroviral prophylaxis for HIV infection in injecting drug users in Bangkok, Thailand (the Bangkok Tenofovir Study): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet. 2013;381(9883):2083–90.
Grohskopf LA, Chillag KL, Gvetadze R, et al. Randomized trial of clinical safety of daily oral tenofovir disoproxil fumarate among HIV-uninfected men who have sex with men in the United States. J Acquir Immune Defic Syndr. 2013;64(1):79–86.
Paltiel AD, Freedberg KA, Scott CA, et al. HIV preexposure prophylaxis in the United States: impact on lifetime infection risk, clinical outcomes, and cost-effectiveness. Clin Infect Dis. 2009;48(6):806–15.
Van der Straten A, Van Damme L, Haberer JE, Bangsberg DR. Unraveling the divergent results of pre-exposure prophylaxis trials for HIV prevention. AIDS. 2012;26(7):F13–9.
Brooks RA, Kaplan RL, Lieber E, et al. Motivators, concerns, and barriers to adoption of preexposure prophylaxis for HIV prevention among gay and bisexual men in HIV-serodiscordant male relationships. AIDS Care. 2011;23(9):1136–45.
Tetteh RA, Nartey ET, Lartey M, et al. Association between the occurrence of adverse drug events and modification of first-line highly active antiretroviral therapy in Ghanaian HIV patients. Drug Saf. 2016;39(11):1139–49.
Smith DK, Thigpen MC, Nesheim SR, et al. Interim guidance for clinicians considering the use of preexposure prophylaxis for the prevention of HIV infection in heterosexually active adults. Morb Mortal Wkly Rep. 2012;61(31):586–9.
Mugwanya KK, Baeten JM. Safety of oral tenofovir disoproxil fumarate-based pre-exposure prophylaxis for HIV prevention. Exp Opin Drug Saf. 2016;15(2):265–73.
Grant RM, van Griensven F. The ADAPT Study: A Phase II, Randomised, Open-Label, Pharmacokinetic and Behavioural Study of the Use of Intermittent Oral Emtricitabine/Tenofovir Disoproxil Fumarate Pre-Exposure Prophylaxis (PrEP). United States: DAIDS. 2011.
Chang ML, Liaw YF. Hepatitis B flares in chronic hepatitis B: pathogenesis, natural course, and management. J Hepatol. 2014;61(6):1407–17.
Knox D, Tan D, Harrigan R, Anderson P, editors. HIV-1 infection with multiclass resistance despite pre-exposure prophylaxis (PrEP). CROI Conference: Boston (MA); 22–25 Feb 2016.
Mimiaga MJ, Case P, Johnson CV, et al. Preexposure antiretroviral prophylaxis attitudes in high-risk Boston area men who report having sex with men: limited knowledge and experience but potential for increased utilization after education. J Acquir Immune Defic Syndr. 2009;50(1):77–83.
Liu A, Cohen S, Follansbee S, Cohan D, et al. Early experiences implementing pre-exposure prophylaxis (PrEP) for HIV prevention in San Francisco. PLoS Med. 2014;11(3):e1001613.
Hosek S, Siberry G, Bell M, et al. Project PrEPare (ATN082): the acceptability and feasibility of an HIV pre-exposure prophylaxis (PrEP) trial with young men who have sex with men (YMSM). J Acquir Immune Defic Syndr. 2013;62(4). doi:10.1097/QAI.0b013e3182801081.
Van der Elst EM, Mbogua J, Operario D, et al. High acceptability of HIV pre-exposure prophylaxis but challenges in adherence and use: qualitative insights from a phase I trial of intermittent and daily PrEP in at-risk populations in Kenya. AIDS Behav. 2013;17(6):2162–72.
Bekker J, Hughes J, Amico R, et al. HPTN 067/ADAPT Cape Town: a comparison of daily and nondaily PrEP dosing in African women. CROI 2015. Seattle (WA): The HIV Prevention Trials Network; 2015.
Haberrer JE. Current concepts for PrEP adherence in the PrEP revolution: from clinical trials to routine practice. Curr Opin HIV AIDS. 2016;11(1):10–7.
Ryom L, Lundgren JD, De Wit S, et al. Use of antiretroviral therapy and risk of end-stage liver disease and hepatocellular carcinoma in HIV-positive persons. AIDS. 2016;30(11):1731–43.
Marcus JL, Glidden DV, Mayer KH, et al. No evidence of sexual risk compensation in the iPrEx trial of daily oral HIV preexposure prophylaxis. PLoS One. 2013;8(12):e81997.
Guest G, Shattuck D, Johnson L, et al. Changes in sexual risk behavior among participants in a PrEP HIV prevention trial. Sex Transm Dis. 2008;35(12):1002–8.
Brooks RA, Landovitz RJ, Kaplan RL, et al. Sexual risk behaviors and acceptability of HIV pre-exposure prophylaxis among HIV-negative gay and bisexual men in serodiscordant relationships: a mixed methods study. AIDS Patient Care STDS. 2012;26(2):87–94.
Mimiaga MJ, Case P, Johnson CV, et al. Preexposure antiretroviral prophylaxis attitudes in high-risk Boston area men who report having sex with men: limited knowledge and experience but potential for increased utilization after education. J Acquir Immun Defic Syndr. 2009;50(1):77–83.
Peterson L, Taylor D, Roddy R, et al. Tenofovir disoproxil fumarate for prevention of HIV infection in women: a phase 2, double-blind, randomized, placebo-controlled trial. PLoS Clin Trials. 2007;2(5):e27.
Authors’ contributions
The authors, RAT, ANOD, BAY and ETN worked on the conception, study design and the final article composition. RAT, ETN, BAY, ML, HGML and ANOD contributed to the methods, results and its continuous critical review. BAY, RAT, ETN, ML, ANOD and HGML worked on the data analysis, discussions and critical revisions. All the authors read and approved the final manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
No sources of funding were used to assist in the preparation of this review.
Conflict of interest
Raymond A. Tetteh, Barbara A. Yankey, Edmund T. Nartey, Margaret Lartey, Hubert G.M. Leufkens, and Alexander N.O. Dodoo have no conflicts of interest that are directly relevant to the content of this review.
Ethics approval
Ethical approval for the study was not obtained as it was a review of published work.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Tetteh, R.A., Yankey, B.A., Nartey, E.T. et al. Pre-Exposure Prophylaxis for HIV Prevention: Safety Concerns. Drug Saf 40, 273–283 (2017). https://doi.org/10.1007/s40264-017-0505-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40264-017-0505-6