
Abstract
Introduction
Current guidelines recommend renin–angiotensin–aldosterone system (RAAS) inhibitors in the treatment of diabetic kidney disease (DKD). However, evidence suggests that the combined use of RAAS blockers may be associated with increased rates of adverse events.
Objectives
Our objective was to examine the efficacy and safety of dual blockade of the RAAS in patients with DKD.
Methods
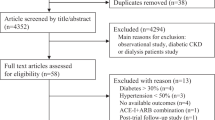
This was a systematic review and meta-analysis of randomized controlled trials (RCTs) published between January 1990 and January 2018 sourced via the PubMed, EMBASE, and Cochrane Library databases. RCTs were included if they investigated the efficacy and safety of dual blockade therapy compared with monotherapy in patients with DKD. Random effects models were used in meta-analysis to account for heterogeneities in effect sizes across the reviewed studies. Analyses were stratified by blood pressure and albuminuria. We further conducted subgroup analyses by considering various combinations of RAAS inhibitors.
Results
Based on 42 RCTs with 14,576 patients, dual RAAS blockade therapy was associated with significant decreases in blood pressure, albuminuria, and proteinuria. However, dual therapy was not superior to monotherapy in terms of reductions in all-cause mortality, cardiovascular mortality, or progression to end-stage renal disease (ESRD). Significant increases in serum potassium and rates of hyperkalemia and hypotension were more common in patients treated with dual therapy. However, glomerular filtration rates (GFR) did not decrease significantly with dual therapy. In subgroup analysis, an angiotensin-converting enzyme inhibitor (ACEI) plus an angiotensin-receptor blocker (ARB) or a direct renin inhibitor (DRI) plus an ACEI/ARB did not significantly increase the risk of hyperkalemia, hypotension, and adverse events, and the risk of hypotension increased significantly within the normotensive subgroup but not within the hypertensive subgroup. The risk of hyperkalemia increased significantly in patients with DKD with macroalbuminuria but not in those with microalbuminuria.
Conclusion
Dual inhibition therapy is superior to monotherapy for blood pressure control and urine protein reduction, though such superiority does not translate into improvements in longer-term outcomes, such as reduced progression to ESRD, all-cause mortality, and cardiovascular mortality. An ACEI plus an ARB or a DRI plus an ACEI/ARB may be a safe and effective therapy for patients with DKD, and combination therapy may be suitable for patients with DKD and hypertension and microalbuminuria.














Similar content being viewed by others


References
Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract. 2010;87:4–14.
Shrishrimal K, Hart P, Michota F. Managing diabetes in hemodialysis patients: observations and recommendations. Cleve Clin J Med. 2009;76:649–55.
National Institute of Diabetes and Digestive and Kidney Diseases. USRDS 2009 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States. https://www.usrds.org/2009/pdf/V1_06_09.pdf. Accessed 7 Feb 2019.
K/DOQI Workgroup. K/DOQI clinical practice guidelines for cardiovascular disease in dialysis patients. Am J Kidney Dis. 2005;45:S1–153.
ESH/ESC Task Force for the Management of Arterial Hypertension. Practice guidelines for the management of arterial hypertension of the European Society of Hypertension (ESH) and the European Society of Cardiology (ESC): ESH/ESC Task Force for the Management of Arterial Hypertension. J Hypertens. 2013;2013(31):1925–38.
Athyros VG, Mikhailidis DP, Kakafika AI, et al. Angiotensin II reactivation and aldosterone escape phenomena in rennin-angiotensin-aldosterone system blockade: is oral renin inhibition the solution? Expert Opin Pharmacother. 2007;8:529–35.
Borch-Johnsen K, Kreiner S. Proteinuria: value as predictor of cardiovascular mortality in insulin dependent diabetes mellitus. BMJ. 1987;294:1651–4.
Gerstein HC, Mann JF, Yi Q, et al. Albuminuria and risk of cardiovascular events, death, and heart failure in diabetic and nondiabetic individuals. JAMA. 2001;286:421–6.
UKPDS GROUP. Development and progression of nephropathy in type 2 diabetes: the United Kingdom Prospective Diabetes Study (UKPDS 64). Kidney Int. 2003;63:225–32.
de Boer IH, Katz R, Cao JJ, et al. Cystatin C, albuminuria, and mortality among older adults with diabetes. Diabetes Care. 2009;32:1833–8.
Fried LF, Emanuele N, Zhang JH, et al. Combination angiotensin inhibition for the treatment of diabetic nephropathy. N Engl J Med. 2013;369:1892–903.
American Diabetes Association. Report of the expert committee on the diagnosis and classification of diabetes mellitus. Diabetes Care. 1997;20:1183–97.
World Health Organization. Definition, diagnosis and classification of diabetes mellitus and its complications. https://apps.who.int/iris/bitstream/handle/10665/66040/WHO_NCD_NCS_99.2.pdf?sequence=1&isAllowed=y. Accessed 7 Feb 2019.
Kidney Disease Outcomes Quality Initiative (K/DOQI). KDOQI clinical practice guidelines and clinical practice recommendations for diabetes and chronic kidney disease. Am J Kidney Dis. 2007;49:S12–154.
Jadad AR, Moore RA, Carroll D, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Controlled Clin Trials. 1996;17:1–12.
Green S. Cochrane handbook for systematic reviews of interventions version 5.1. 0 [updated March 2011]. The Cochrane Collaboration 2011.
Huedo-Medina TB, Sanchez-Meca J, Marin-Martinez F, et al. Assessing heterogeneity in meta-analysis: Q statistic or I2 index? Psychol Methods. 2006;11:193–206.
Egger M, Davey Smith G, Schneider M, et al. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–34.
Atmaca A, Gedik O. Effects of angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers, and their combination on microalbuminuria in normotensive patients with type 2 diabetes. Adv Ther. 2006;23:615–22.
Bakris GL, Oparil S, Purkayastha D, et al. Randomized study of antihypertensive efficacy and safety of combination aliskiren/valsartan vs valsartan monotherapy in hypertensive participants with type 2 diabetes mellitus. J Clin Hypertens. 2013;15:92–100.
Cetinkaya R, Odabas AR, Selcuk Y. Anti-proteinuric effects of combination therapy with enalapril and losartan in patients with nephropathy due to type 2 diabetes. Int J Clin Pract. 2004;58:432–5.
Epstein M, Williams GH, Weinberger M, et al. Selective aldosterone blockade with eplerenone reduces albuminuria in patients with type 2 diabetes. Clin J Am Soc Nephrol. 2006;1:940–51.
Fernandez Juarez G, Luno J, Barrio V, et al. Effect of dual blockade of the renin–angiotensin system on the progression of type 2 diabetic nephropathy: a randomized trial. Am J Kidney Dis. 2013;61:211–8.
Igarashi M, Hirata A, Kadomoto Y, et al. Dual blockade of angiotensin II with enalapril and losartan reduces proteinuria in hypertensive patients with type 2 diabetes. Endocr J. 2006;53:493–501.
Jacobsen P, Andersen S, Jensen BR, et al. Additive effect of ACE inhibition and angiotensin II receptor blockade in type I diabetic patients with diabetic nephropathy. J Am Soc Nephrol. 2003;14:992–9.
Jacobsen P, Andersen S, Rossing K, et al. Dual blockade of the renin–angiotensin system in type 1 patients with diabetic nephropathy. Nephrol Dial Transplant Off Publ Eur Dial Transpl Assoc Eur Ren Assoc. 2002;17:1019–24.
Jacobsen P, Andersen S, Rossing K, et al. Dual blockade of the renin–angiotensin system versus maximal recommended dose of ACE inhibition in diabetic nephropathy. Kidney Int. 2003;63:1874–80.
Jacobsen P, Parving HH. Beneficial impact on cardiovascular risk factors by dual blockade of the renin–angiotensin system in diabetic nephropathy. Kidney Int Suppl. 2004;92:S108–10.
Kim MJ, Song JH, Suh JH, et al. Additive antiproteinuric effect of combination therapy with ACE inhibitor and angiotensin II receptor antagonist: differential short-term response between IgA nephropathy and diabetic nephropathy. Yonsei Med J. 2003;44:463–72.
Krairittichai U, Chaisuvannarat V. Effects of dual blockade of renin–angiotensin system in type 2 diabetes mellitus patients with diabetic nephropathy. J Med Assoc Thail Chotmaihet Thangphaet. 2009;92:611–7.
Makhlough A, Kashi Z, Akha O, et al. Effect of spironolactone on diabetic nephropathy compared to the combination of spironolactone and losartan. Nephro Urol Mon. 2014;6:e12148.
Matos JP, de Lourdes Rodrigues M, Ismerim VL, et al. Effects of dual blockade of the renin angiotensin system in hypertensive type 2 diabetic patients with nephropathy. Clin Nephrol. 2005;64:180–9.
Mehdi UF, Adams-Huet B, Raskin P, et al. Addition of angiotensin receptor blockade or mineralocorticoid antagonism to maximal angiotensin-converting enzyme inhibition in diabetic nephropathy. J Am Soc Nephrol. 2009;20:2641–50.
Mogensen CE, Neldam S, Tikkanen I, et al. Randomised controlled trial of dual blockade of renin–angiotensin system in patients with hypertension, microalbuminuria, and non-insulin dependent diabetes: the candesartan and lisinopril microalbuminuria (CALM) study. BMJ. 2000;321:1440–4.
Nakamura A, Shikata K, Nakatou T, et al. Combination therapy with an angiotensin-converting-enzyme inhibitor and an angiotensin II receptor antagonist ameliorates microinflammation and oxidative stress in patients with diabetic nephropathy. J Diabetes Investig. 2013;4:195–201.
Nakamura T, Ushiyama C, Osada S, et al. Combination therapy of trandolapril and candesartan cilexetil reduces microalbuminuria and urinary endothelin-1 excretion in patients with type 2 diabetes. Clin Exp Nephrol. 2002;6:135–9.
Nielsen SE, Persson F, Frandsen E, et al. Spironolactone diminishes urinary albumin excretion in patients with type 1 diabetes and microalbuminuria: a randomized placebo-controlled crossover study. Diabet Med. 2012;29:e184–90.
Ogawa S, Takeuchi K, Mori T, et al. Effects of monotherapy of temocapril or candesartan with dose increments or combination therapy with both drugs on the suppression of diabetic nephropathy. Hypertens Res. 2007;30:325–34.
Parving HH, Brenner BM, McMurray JJ, et al. Cardiorenal end points in a trial of aliskiren for type 2 diabetes. N Engl J Med. 2012;367:2204–13.
Parving HH, Persson F, Lewis JB, et al. Aliskiren combined with losartan in type 2 diabetes and nephropathy. N Engl J Med. 2008;358:2433–46.
Persson F, Rossing P, Reinhard H, et al. Renal effects of aliskiren compared with and in combination with irbesartan in patients with type 2 diabetes, hypertension, and albuminuria. Diabetes Care. 2009;32:1873–9.
Rachmani R, Slavachevsky I, Amit M, et al. The effect of spironolactone, cilazapril and their combination on albuminuria in patients with hypertension and diabetic nephropathy is independent of blood pressure reduction: a randomized controlled study (Retracted article see vol 23, pg 818, 2006). Diabet Med. 2004;21:471–5.
Rossing K, Christensen PK, Jensen BR, et al. Dual blockade of the renin-angiotensin system in diabetic nephropathy: a randomized double-blind crossover study. Diabetes Care. 2002;25:95–100.
Rossing K, Jacobsen P, Pietraszek L, et al. Renoprotective effects of adding angiotensin II receptor blocker to maximal recommended doses of ACE inhibitor in diabetic nephropathy: a randomized double-blind crossover trial. Diabetes Care. 2003;26:2268–74.
Rossing K, Schjoedt KJ, Smidt UM, et al. Beneficial effects of adding spironolactone to recommended antihypertensive treatment in diabetic nephropathy: a randomized, double-masked, cross-over study. Diabetes Care. 2005;28:2106–12.
Saklayen MG, Gyebi LK, Tasosa J, et al. Effects of additive therapy with spironolactone on proteinuria in diabetic patients already on ACE inhibitor or ARB therapy: results of a randomized, placebo-controlled, double-blind, crossover trial. J Investig Med. 2008;56:714–9.
Schjoedt KJ, Rossing K, Juhl TR, et al. Beneficial impact of spironolactone in diabetic nephropathy. Kidney Int. 2005;68:2829–36.
Schjoedt KJ, Rossing K, Juhl TR, et al. Beneficial impact of spironolactone on nephrotic range albuminuria in diabetic nephropathy. Kidney Int. 2006;70:536–42.
Sengul AM, Altuntas Y, Kurklu A, et al. Beneficial effect of lisinopril plus telmisartan in patients with type 2 diabetes, microalbuminuria and hypertension. Diabetes Res Clin Pract. 2006;71:210–9.
Song JH, Cha SH, Lee HJ, et al. Effect of low-dose dual blockade of renin–angiotensin system on urinary TGF-beta in type 2 diabetic patients with advanced kidney disease. Nephrol Dial Transplant Off Publ Eur Dial Transpl Assoc Eur Ren Assoc. 2006;21:683–9.
Tan F, Mukherjee JJ, Lee KO, et al. Dual blockade of the renin–angiotensin–aldosterone system is safe and effective in reducing albuminuria in Asian type 2 diabetic patients with nephropathy. Singap Med J. 2010;51:151–6.
Titan SM, Vieira JM Jr, Dominguez WV, et al. ACEI and ARB combination therapy in patients with macroalbuminuric diabetic nephropathy and low socioeconomic level: a double-blind randomized clinical trial. Clin Nephrol. 2011;76:273–83.
Tutuncu NB, Gurlek A, Gedik O. Efficacy of ACE inhibitors and ATII receptor blockers in patients with microalbuminuria: a prospective study. Acta Diabetol. 2001;38:157–61.
Van Buren PN, Adams-Huet B, Nguyen M, et al. Potassium handling with dual renin–angiotensin system inhibition in diabetic nephropathy. Clin J Am Soc Nephrol. 2014;9:295–301.
van den Meiracker AH, Baggen RG, Pauli S, et al. Spironolactone in type 2 diabetic nephropathy: Effects on proteinuria, blood pressure and renal function. J Hypertens. 2006;24:2285–92.
Persson F, Lewis JB, Lewis EJ, Rossing P, Hollenberg NK, Hans-Henrik P. Impact of aliskiren treatment on urinary aldosterone levels in patients with type 2 diabetes and nephropathy: an AVOID substudy. J Renin-Angiotensin-Aldosterone Syst. 2012;13(1):118–21.
Doulton TW, He FJ, MacGregor GA. Systematic review of combined angiotensin-converting enzyme inhibition and angiotensin receptor blockade in hypertension. Hypertension. 2005;45:880–6.
Susantitaphong P, Sewaralthahab K, Balk EM, et al. Efficacy and safety of combined vs. single renin–angiotensin–aldosterone system blockade in chronic kidney disease: a meta-analysis. Am J Hypertens. 2013;26:424–41.
MacKinnon M, Shurraw S, Akbari A, et al. Combination therapy with an angiotensin receptor blocker and an ACE inhibitor in proteinuric renal disease: a systematic review of the efficacy and safety data. Am J Kidney Dis. 2006;48:8–20.
Bakris GL, Ruilope L, Locatelli F, et al. Treatment of the microalbuminuria in hypertensive subjects with elevated cardiovascular risk: results of the IMPROVE trial. Kidney Int. 2007;72:879–85.
Menne J, Farsang C, Deák L, et al. Valsartan in combination with lisinopril versus the respective high dose monotherapies in hypertensive patients with microalbuminuria: the VALERIA trial. J Hypertens. 2008;26:1860–7.
Catapano F, Chiodini P, De Nicola L, et al. Antiproteinuric response to dual blockade of the renin-angiotensin system in primary glomerulonephritis: meta-analysis and metaregression. Am J Kidney Dis. 2008;52:475–85.
Kunz R, Friedrich C, Wolbers M, et al. Meta-analysis: effect of monotherapy and combination therapy with inhibitors of the renin angiotensin system on proteinuria in renal disease. Ann Intern Med. 2008;148:30–48.
Kalaitzidis RG, Bakris GL. The current state of RAAS blockade in the treatment of hypertension and proteinuria. Curr Cardiol Rep. 2009;11:436–42.
Bomback AS, Toto R. Dual blockade of the renin–angiotensin–aldosterone system: beyond the ACE inhibitor and angiotensin-II receptor blocker combination. Am J Hypertens. 2009;22:1032–40.
Forclaz A, Maillard M, Nussberger J, et al. Angiotensin II receptor blockade: is there truly a benefit of adding an ACE inhibitor? Hypertension. 2003;41:31–6.
Cohen DL, Townsend RR. Is there added value to adding ARB to ACE inhibitors in the management of CKD? J Am Soc Nephrol. 2009;20:1666–8.
Imai E, Haneda M, Yamasaki T, et al. Effects of dual blockade of the renin–angiotensin system on renal and cardiovascular outcomes in type 2 diabetes with overt nephropathy and hypertension in the ORIENT: a post-hoc analysis (ORIENT-Hypertension). Hypertens Res. 2013;36:1051–9.
Mann JF, Schimieder RE, McQueen M, et al. Renal outcomes with telmisartan, ramipril, or both, in people at high vascular risk (the ONTARGET study): a multicenter, randomized, double-blind, controlled trial. Lancet. 2008;372:547–53.
Palmer SC, Mavridis D, Navarese E, et al. Comparative efficacy and safety of blood pressure-lowering agents in adults with diabetes and kidney disease: a network meta-analysis. Lancet. 2015;385:2047–56.
James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311:507–20.
Jennings DL, Kalus JS, Coleman CI, et al. Combination therapy with an ACE inhibitor and an angiotensin receptor blocker for diabetic nephropathy: a meta-analysis. Diabet Med. 2007;24:486–93.
de Zeeuw D, Remuzzi G, Parving HH, et al. Proteinuria, a target for renoprotection in patients with type 2 diabetic nephropathy: lessons from RENAAL. Kidney Int. 2004;65:2309–20.
Messerli FH, Staessen JA, Zannad F. Of fads, fashion, surrogate endpoints and dual RAS blockade. Eur Heart J. 2010;31:2205–8.
Kato S, Maruyama S, Makino H, et al. Anti-albuminuric effects of spironolactone in patients with type 2 diabetic nephropathy: a multicenter, randomized clinical trial. Clin Exp Nephrol. 2015;19:1098–106.
Garg R, Rao AD, Baimas-George M, Hurwitz S, Foster C, Shah RV, Jerosch-Herold M, Kwong RY, Di Carli MF, Adler GK. Mineralocorticoid receptor blockade improves coronary microvascular function in individuals with type 2 diabetes. Diabetes. 2015;64(1):236–42.
Bakris GL, Agarwal R, Chan JC, Cooper ME, Gansevoort RT, Haller H, Remuzzi G, Rossing P, Schmieder RE, Nowack C, Kolkhof P. Effect of finerenone on albuminuria in patients with diabetic nephropathy: a randomized clinical trial. Jama. 2015;314(9):884-94.
Acknowledgements
None.
Author information
Authors and Affiliations
Contributions
PF and YL coordinated the review and organized the team. PF and YF contributed to developing the protocol. YF and RH assessed the studies and extracted data. LL, XZ, RH, JK, and LL contributed to the data analysis and interpretation. YF and RH drafted the review. JK and XZ edited and formatted the review text. YL and PF reviewed the review and made important intellectual contributions.
Corresponding authors
Ethics declarations
Funding
This study was funded by the National Postdoctoral Program for Innovative Talents of China (BX201600112).
Conflict of interest
Yanhuan Feng, Rongshuang Huang, Janet Kavanagh, Lingzhi Li, Xiaoxi Zeng, Yi Li, and Ping Fu have no potential conflicts of interest that might be relevant to the contents of this manuscript.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Feng, Y., Huang, R., Kavanagh, J. et al. Efficacy and Safety of Dual Blockade of the Renin–Angiotensin–Aldosterone System in Diabetic Kidney Disease: A Meta-Analysis. Am J Cardiovasc Drugs 19, 259–286 (2019). https://doi.org/10.1007/s40256-018-00321-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40256-018-00321-5