
Abstract
Hepatitis C virus (HCV) causes a persistent chronic infection of hepatocytes resulting in progressive fibrosis and carcinogenesis. Abnormalities in mitochondria are prominent features of clinical disease where ultrastructural changes, alterations in electron transport, and excess reactive oxygen species production occur. These mitochondrial abnormalities correlate with disease severity and resolve with viral eradication. Multiple viral proteins, particularly core and NS3/4a bind to mitochondria. The core and NS5a proteins primarily cause ER stress, ER Ca2+ release and enhance direct transfer of Ca2+ from ER to mitochondria. This results in electron transport changes, increased ROS production, and sensitivity to mitochondrial permeability transition and cell death. The viral protease, NS3/4a, binds to mitochondria as well where it cleaves an important signaling adapter, MAVS, thus preventing viral clearance by endogenous interferon production. This review discusses the mechanisms by which HCV causes mitochondrial changes and consequences of these for disease.
Similar content being viewed by others


Introduction
Hepatitis C Virus (HCV) is an important human pathogen that infects almost 2 % of the world’s population [1]. It was the first virus to be identified by purely molecular techniques and its discovery in 1989 [2, 3] initiated a tremendous research effort into the mechanisms of tissue injury and fibrosis that has resulted in the development of new concepts and paradigms in liver disease. We now know that chronic viral infections can be cured, most hepatocellular carcinoma is a viral disease, cirrhosis is reversible, and a quartet of immune, host, viral and environmental factors all combine to produce liver disease.
For most of the HCV era, treatment of the disease was difficult and problems such as limited access to medical care, intolerable side effects, or poor efficacy of medications meant that only a small minority of patients could expect to have their HCV cured [4]. This left about 80 % of “real world” HCV patients to progress as the disease as it took its course. This situation created a great interest in understanding the mechanisms of how HCV caused liver injury and how this liver injury might be minimized. Studying chronically infected patients revealed an almost universal presence of mitochondrial alterations that were intimately linked to the pathogenesis and persistence of the disease. Many of these have subsequently been shown to be direct results of viral protein-mitochondrial interactions. New developments in HCV therapy hold out the prospect that it will soon be possible to achieve over 90 % cure rates with easily tolerable oral medications, limited only by financial considerations and access to medical care [5]. With these developments the continued interest in HCV host pathogen interactions is sure to wane, but the information learned from HCV pathogenesis studies will continue to be relevant to deeper understanding of viral-host interactions and liver disease in general.
The association of human HCV infection with cellular and tissue changes that reflect mitochondrial dysfunction was observed shortly after the disease was identified. These have been confirmed in hundreds of studies. These include ultrastructural changes in mitochondria [6], increased markers of oxidative stress in the liver [7] and evidence of oxidative stress markers in blood [7]. In spite of these consistent observations, it has been more difficult to separate specific HCV mechanisms from a more general process occurring in inflammatory diseases as a whole and many questions regarding the significance of HCV-mitochondrial interactions are in dispute. Nonetheless, four key facts have been established that are strongly supported in the literature. These are:
-
1.
Ultrastructural mitochondrial abnormalities and increased ROS production occur in hepatocytes from HCV infected patients.
-
2.
HCV proteins directly bind to mitochondria or mitochondria-associated membrane fractions in a wide variety of experimental model systems.
-
3.
HCV infection alters mitochondrial Ca2+ homeostasis and excess production of mitochondrial ROS induced by HCV in cellular model systems can be prevented by blocking mitochondrial Ca2+ accumulation.
-
4.
HCV cleaves the signaling protein MAVS off the surface of mitochondria blocking an important antiviral innate immune process.
Hepatitis C virus likely has other effects on mitochondria as well, such as altering their clearance by mitophagy and suppressing induction of antioxidant pathways, but these effects have proven less reproducible and may only occur in special circumstances.
While the existence of mitochondrial effects of HCV is clear, the consequences of these effects are not. Data supports both pro- and anti-viral consequences of mitochondrial modifications and the extent to which mitochondrial effects are an appropriate host response, a pathological disease mechanism, or both is unclear. This article will review the evidence for the known effects of HCV on mitochondria and will discuss several areas where understanding the HCV-mitochondrial interactions may provide clues to disease pathogenesis.
The HCV Lifecycle
Hepatitis C virus is an enveloped, single stranded, positive sense RNA virus that circulates in humans as a modified lipoprotein particle sometimes called a lipoviroprotein [8]. The virus infects hepatocytes by binding to a multicomponent receptor consisting of CD81, SR-B1, claudin-1 and occludin. Receptor binding triggers clathrin-mediated endocytosis and a subsequent uncoating step releases the viral RNA into the cytoplasm [9]. This message sense RNA immediately interacts with ER-associated ribosomes generating the first round of viral proteins. The polyprotein is processed by host signal peptidases and then by the NS3/4a viral encoded protease. The individual viral proteins then assemble a replication complex [10].
The processes of HCV RNA replication, protein translation, virion particle assembly, maturation, and secretion are all membrane associated and take place at various sites. The viral protein NS4b serves as an anchor and membrane modifying protein that is sufficient by itself to form a modification of the ER termed the membranous web [11]. The latter stages of HCV particle assembly, maturation, and secretion are less well understood but involve interactions of the nacent virions with lipid droplets, ER, and lipoprotein secretion pathways [12].
The HCV viral polyprotein is processed by a series of host and viral proteases to produce the mature viral proteins. There are three structural proteins, seven non-structural proteins, and one alternate reading frame protein [10]. The structural proteins are the core or capsid protein and the envelop proteins E1 and E2. The nonstructural proteins consist of p7, a small viral ion channel, NS2, NS3 and NS4a which together form a multifunctional viral protease and helicase, NS4b, NS5a, a multifunctional protein involved in particle assembly, RNA replication and modulation of host responses, and NS5b, the RNA-dependent RNA polymerase. As for nearly all viral proteins, the HCV proteins are highly multifunctional and three proteins in particular, core, NS3, and NS5a, bind to hundreds of host target proteins [13] and are active in modulating a number of cellular functions such as lipid metabolism, cell death pathways, innate immune responses, autophagy, and metabolism [14•].
Mitochondrial Association of HCV Proteins
Viruses frequently modify mitochondrial function through direct interaction of viral proteins with mitochondrial components. Viral proteins can bind to the outer membrane, be imported into the matrix or intermembrane space, or bind to membrane sites closely associated with the mitochondria such as the mitochondria associated membrane (MAM) fraction of the ER [15]. In the case of hepatitis C, a number of different mitochondrial associations have been reported.
The most studied mitochondrial interacting protein is core. Core protein is consistently co-purified in crude mitochondrial preparations from HCV infected or protein overexpressing systems, and subcellular fractionation and protease digestion have revealed primarily an outer membrane site [16–19]. A recent immunoEM study in replicon bearing cells has also shown evidence of core in the inner membrane [20] but this has not been observed in other studies of either viral infection or core protein overexpression. The two most carefully performed studies [16, 17] both identified core as associated with the mitochondrial outer membrane and particularly the MAM fraction. These studies both identified a C-terminal hydrophobic domain sequence that was required for binding. One of the problems with this analysis is that core protein is abundant, extremely hydrophobic, and only a very small fraction of it is present in mitochondria. Much greater quantities are present in both ER and lipid droplets [21, 22]. Since ER is closely associated with mitochondria in hepatocytes, there is still some doubt about whether core protein binds directly to mitochondria or rather binds to an ER fraction that is closely associated with mitochondria such as the MAM.
Another HCV protein that strongly associates with mitochondria is NS3/4a, the primary viral protease [23]. At the mitochondrial surface it cleaves MAVS, a tail anchored outer membrane protein that is required for generation of an interferon response to RNA viruses [24, 25]. This protein is an essential component of the innate immune response in which dsRNA originating from viruses is recognized by the RIG-I receptor and ultimately stimulates activation of IRF3 and production of β-interferon.
Several other HCV proteins have been identified to associate with mitochondria by fractionation, immunoEM or others methods, but many of these interactions have only been observed in overexpression systems. p7 overexpression results in its association with mitochondria [26], and NS5a and NS5b have been identified by immunoEM to be present in the mitochondrial inner membrane and matrix [20]. In these latter cases the functional significance has not been demonstrated and the extent to which the localization is model dependent has not been rigorously evaluated.
Mitochondrial Abnormalities in Human HCV Infection
An association of human HCV infection with hepatic mitochondrial dysfunction and oxidative stress has been a consistent clinical observation. Analysis of patient samples has demonstrated ultrastructural changes in mitochondria [6], increases in lipid peroxidation products [27–31] and oxidative DNA adducts [32, 33], decreased hepatic and circulating antioxidant levels [27–29, 34], induction of oxidant stress induced proteins [35, 36], the presence of oxidized protein and lipid derivatives in the liver [7, 33], and the presence of free radicals in liver biopsy specimens [37].
While oxidative stress is present in nearly all inflammatory diseases, it appears to be greater for hepatitis C than for other liver diseases such as autoimmune hepatitis or chronic hepatitis B [37–39]. In addition, there is a correlation between greater degrees of oxidative stress markers and more severe inflammation [28, 29, 31–33, 37], insulin resistance [40, 41], fibrosis progression and the development of hepatocellular carcinoma [42]. Successful response to interferon based therapy decreases oxidative stress markers [27]. Further circumstantial evidence for the pathological role of oxidative stress and mitochondrial dysfunction in liver injury is the well described disease synergy of HCV with agents that cause mitochondrial injury such as alcohol [43] and acetaminophen [44]. Overall, these observations demonstrate that chronic hepatitis C in humans has a distinct mitochondrial dysfunction footprint that correlates with disease severity.
The conclusion that HCV causes significant functional alterations in mitochondria is further supported by abundant data in experimental model systems. These include transgenic mice expressing viral proteins [18, 19, 45], chimeric mice with humanized livers infected with HCV [46], cell culture systems expressing viral proteins or replicating viral RNA [47–49], and cells infected with culture adapted forms of HCV [50]. The most commonly described phenomena are that HCV causes an increase in mitochondrial ROS production, inhibition of mitochondrial electron transport, alterations in mitochondrial morphology, inhibition of innate immune signaling, and sensitization to mitochondrial cell death cascades. These mitochondrial effects of HCV can be divided into two major classes, those affecting electron transport and ROS production, and those that are independent of changes in electron transport. Both are relevant to pathogenesis and will be discussed separately.
Mechanisms of Oxidative HCV Effects on Mitochondria
The most consistent and best described oxidative effects of HCV result from effects of the viral core protein. While core is the viral capsid protein, only a small fraction of it is incorporated into virions. The remainder resides in membrane and lipid associated structures, particularly in ER, lipid droplets and in the MAM fraction [16, 21, 22]. Mitochondrial effects of core have been highly reproducible between laboratories and across model systems. Core protein expression results in activation of ER stress pathways [51], and Ca2+ release from the ER resulting in a decrease in ER Ca2+ content [49, 52, 53]. In mitochondria, core causes an increase in ROS production [18], an increase in matrix Ca2+ content and greater uptake into mitochondria of the Ca2+ released from the ER [49, 54]. At the level of electron transport, core produces a selective decrease in complex 1 activity, and increased superoxide production from complex 1 [19, 54]. These effects are not sufficient to cause either cell death or mitochondrial permeability transition (MPT), but HCV infected or core expressing cells, unlike control cells, rapidly undergo MPT and cell death after exposure to exogenous oxidative stress or induction of ER Ca2+ release [50, 54, 55]. While ER stress, ER Ca2+ release and activation of stress kinases can be produced by multiple viral proteins [56], core is required for the viral sensitization to MPT [50]. This conclusion is further supported by the observation that addition of purified core protein to isolated mitochondria is sufficient to increase Ca2+ uptake, increase ROS production, and cause ROS and Ca2+-dependent MPT [19, 50, 54].
In isolated mitochondria, core protein alters the regulation of the mitochondrial Ca2+ uniporter (MCU), increasing both uptake rate and maximal matrix Ca2+ concentration in response to a given extramitochondrial Ca2+ stimulus [54]. All the mitochondrial effects of core protein are entirely Ca2+ dependent and can be prevented by multiple methods that block Ca2+ entry into mitochondria such as Ca2+ chelation or inhibition of the MCU [49, 50]. Selective effects of complex 1 thus appear to be a result of this complex’s unique sensitivity to glutathione oxidation and glutathionylation [57], and not to any specific interaction of core with electron transport complexes. The effect of core protein is thus primarily a modification of the ER-mitochondrial Ca2+ transfer network [58] to more efficiently transfer Ca2+ from ER to mitochondria. This secondarily affects the mitochondrial inner membrane through Ca2+-mediated changes in redox potential. However, the weight of evidence shows that core neither crosses the MOM nor binds to any part of the mitochondrion except the MAM.
One of the important unanswered questions about the HCV-mitochondrial interaction is how the binding of core protein to structures present on the outer surface of mitochondria, or even only the MAM, can alter the regulation of the inner membrane protein MCU. This is an area of active investigation and with the recent identification of MCU protein [59••], it is possible that answers will be forthcoming. The current thinking is that efficient Ca2+ uptake requires close molecular interactions between the MCU, its associated regulatory proteins and outer membrane components such as VDAC [60], and by binding to the external portion of one of these components, core may affect the functioning of the entire system.
In addition to core, other HCV proteins have been shown to produce a mitochondrial ROS phenotype. This is best shown for NS5a although in this case there is limited evidence of direct interactions with mitochondria and the effect seems to be more a result of the rather profound ER stress caused by this protein [61–63]. The NS3/NS4a complex also increases ROS formation [55]. It forms a protease that binds to the mitochondrial outer membrane where it both modulates innate immune signaling [64] and increases mitochondrial ROS production [23].
It is important to note that not all HCV associated oxidative stress comes from mitochondria. ROS production from macrophages and neutrophils [65] as well as cytosolic sources such as NADPH oxidase are present as well [66, 67•]. HCV infection also suppresses hepatic hepcidin production [68, 69] thus increasing intestinal Fe absorption and resulting in hepatic iron overload [70].
Effects of HCV on Antioxidants
As discussed, HCV has a more prominent oxidative stress phenotype than other diseases that share an inflammatory component. Part of the explanation for this appears to be HCV’s ability to manipulate antioxidant responses. Several antioxidant pathways have been shown to be modulated by HCV. Heme oxygenase-1 (HO-1) is an inducible antioxidant enzyme that works by generating the antioxidant biliverdin from heme. HCV inhibits its induction, both in model systems and in patient samples, exacerbating the oxidative stress phenotype [71]. Nrf2 is a redox activated transcription factor that also plays a role in antioxidant responses [72]. Its target genes include the glutathione synthesizing enzyme GCL as well as a number of GSTs. Reduction of Nrf2 activity sensitizes the liver to a number of redox dependent injury steps and augmentation of Nrf2 is hepatoprotective [73]. HCV effects on Nrf2 occur and appear to be context dependent. Several studies have shown an activation as a result of HCV protein expression [74, 75], but in HCV replicating cells there is an inhibition of Nrf2 translocation to the nucleus. This results from its interaction with small Maf proteins which fail to localize to the nucleus because they associate with the HCV replication complexes [76].
Recent studies from our lab have also shown that HCV modulates the function of the redox related transcription factor FOXO3 [77•]. FOXO3 target genes SOD2, catalase and peroxiredoxin 3 are all involved in antioxidant response. While HCV by itself activates FOXO3, the combination of HCV and alcohol causes loss of FOXO3 from the nucleus and a decrease in the mitochondrial expression of SOD2. Taken together, HCV can thus have variable effects on antioxidant capacity, and under some circumstances, such as in the presence of alcohol, there is a loss of antioxidant enzymes at the same time as ROS production is increasing.
Effects of HCV on Mitochondrial Based Signaling Pathways
In addition to their effects on mitochondrial bioenergetic and redox processes, HCV proteins interact with mitochondria in ways that specifically affect innate immune signaling events. The antiviral response to RNA viruses such as HCV involves recognition of dsRNA by the RNA helicase RIG-I and a signal transduction process that requires binding to the mitochondrial outer membrane protein MAVS, and consequent activation of IKKε, phosphorylation of IRF3, and induction of interferon β production [78]. The discovery of MAVS by Chen and colleagues [79] showed the centrality of the mitochondria to this process. Cleavage or relocalization of MAVS off the mitochondria abolished its ability to signal and blocked endogenous interferon production in response to viral infection.
Shortly after discovery of MAVS it was shown that the HCV protease, NS3/NS4a, avidly cleaves a site in the C-terminal anchor loop of MAVS releasing this latter protein from the mitochondria and abolishing IFNβ production in response to HCV [24, 25]. This mechanism has subsequently been shown to play a significant role in HCV persistence and this proteolysis of a mitochondrial protein may be one of HCV’s most significant mitochondrial effects [80].
MAVS is an outer membrane mitochondrial protein but it is also present in membranes from ER and the MAM. The MAM-localized MAVS appears to be the most relevant for initiation of the downstream events of antiviral signaling [81••]. NS3/4a preferentially localizes to the MAM where it cleaves the most signaling active fraction of MAVS [82], preventing the interferon response and allowing establishment of chronic infection.
Hepatitis C virus also has multiple effects on apoptosis pathways with considerable variability, either positive or negative, depending on the experimental systems used [83]. One consistent observation is that infection of hepatoma cells with cell culture adapted HCV eventually causes apoptosis and markedly sensitizes cells to TRAIL-induced apoptosis. This latter phenomenon is mediated primarily by the mitochondrial cell death pathways and while its mechanism is poorly understood, it has been attributed to both increases in cell surface TRAIL receptors [84] and enhanced cleaved Bid and active Bax [85] translocation to mitochondria.
HCV and Mitochondrial Quality Control Mechanisms
Hepatitis C virus is able to alter the function of mitochondrial chaperones responsible for assembly of the electron transport complexes themselves and this effect may, in part, explain the observation that there is a selective complex 1 deficiency in HCV infection. Several groups have shown that HCV proteins or HCV itself increases the expression level of prohibitin, a mitochondrial matrix chaperone [86, 87]. Prohibitin was shown to avidly bind to HCV core protein and this binding was sufficient to reduce its binding to the mitochondrially encoded protein subunits of complex 1 thus interfering with the assembly of this complex [87].
Further effects of HCV on mitochondrial quality control occur via effects on autophagy pathways [88]. HCV alters autophagy pathways possibly to use autophagy related structures as replicative intermediates or to avoid innate immune responses. It has recently been observed that there is a specific interaction of HCV with a mitochondria specific autophagy pathway termed mitophagy [89]. Mitophagy is controlled to a large extent by two proteins, Pink1 and Parkin [90]. Pink1 is a kinase that accumulates on the surface of depolarized mitochondria. Pink1 accumulation recruits the E3 ubiquitin ligase, Parkin, to the mitochondrial outer membrane where it ubiquitinates mitochondrial substrates triggering mitophagy. A recent study by Siddiqi and colleagues showed that HCV infection increased both Parkin and Pink1 gene expression, increased their association with mitochondria and promoted mitophagy [91•]. The loss of respiratory chain activity, so frequently associated with HCV, could be blocked by silencing Parkin expression. However, another study of the effects of HCV on mitophagy noted that recruitment of Parkin to mitochondria was actually inhibited by HCV and this was attributed to direct binding of Parkin to core protein in the cytosol with loss its ability to be move to mitochondria [92]. Clearly these issues will need to be resolved, but the above studies clearly indicate the ability of HCV not to just alter mitochondrial function but to also affect mitochondrial quality control mechanisms.
Consequences of HCV-Mitochondrial Interactions
There are three main consequences that are currently recognized as resulting from HCV-mitochondria interactions. First is the role of oxidative stress in pathogenesis [93]. Pathologically, oxidative stress contributes to many aspects of the disease. Combined with steatosis, it promotes fibrogenesis [94], carcinogenesis [95] and sets up positive feedback loops promoting steatosis, oxidative DNA damage and cell death signaling [96].
The second consequence is related to ROS effects on the virus itself. There is considerable evidence that ROS directly suppress HCV replication [97]. It has been proposed that this may be a result of either lipid peroxidation [98] or ROS dependent changes in cellular calcium [99]. While it would seem counterintuitive that the virus would develop mechanisms to limit its own replication, unchecked replication could be harmful to long term persistence of the virus if persistently high viral loads either promote immune clearance or so aggressively kill the host that it would reduce the chances of viral transmission. This ROS suppression of viral replication may also explain some of the disappointing clinical results with antioxidant therapies [100]. Finally, the cleavage of mitochondrial MAVS is clearly important for establishment of chronic infection and helps to explain the high efficacy of NS3/4a protease inhibitors in this disease.
Conclusions
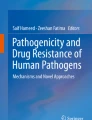
Hepatitis C virus interacts with mitochondria in multiple ways. These are illustrated in Fig. 1. The best documented effects are production of ROS, modulation of antioxidant pathways, suppression of innate immunity, and alteration of mitophagy. These effects play a role in promoting that delicate balance of chronic infection in which viral replication is ongoing but not sufficient to induce either clearance or rapid death of the host. There are many unanswered questions in terms of these mitochondrial effects. The oxidative stress response clearly plays only a small part in the overall pathogenesis and the results of antioxidant therapy trials have been uniformly disappointing. The finding that ROS suppresses rather than promotes replication may be an important part of this equation.

Mechanisms by which HCV modifies mitochondrial function. HCV increases ROS production as a consequence of increasing Ca2+ transfer from the ER to the mitochondria, largely through the effects of NS5a and core. The viral NS3/4a protease cleaves the signaling protein MAVS from the MAM fraction of the mitohcondrial associated ER membrane thus blocking innate immune signaling. The HCV-ethanol combination inhibits the activity of the transcription factor FOXO3 thus decreasing the production of SOD2 and reducing mitochondrial antioxidant capacity. HCV interacts with the cytosolic ubiquitin E3 ligase changing its ability to translocate to the mitochondrial outer membrane and induce mitophagy
Given the limitations of the model systems, many of these questions can best be answered in human patients who are chronically infected. While the details of how mitochondrial-viral interactions promote pathology are of great scientific interest, thankfully the era of studying chronically infected HCV patients with incurable disease may be coming to an end. As of this writing the second generation of direct acting antiviral agents is about to be FDA approved and these hold the promise of much greater therapeutic viral clearance with low levels of side effects. Once these are widely available, it will no longer be a clinical goal to find ways to mitigate liver injury in patients who remain chronically infected. However, the lesson learned from HCV will be applicable to other diseases for which mitochondrial dysfunction plays a pathological role.
References
Recently published papers of particular interest have been highlighted as: • Of importance •• Of major importance
Shepard CW, Finelli L, Alter MJ (2005) Global epidemiology of hepatitis C virus infection. Lancet Infect Dis 5:558–567
Alter HJ, Purcell RH, Shih JW, Melpolder JC, Houghton M, Choo QL, Kuo G (1989) Detection of antibody to hepatitis C virus in prospectively followed transfusion recipients with acute and chronic non-A, non-B hepatitis. N Engl J Med 321:1494–1500
Choo QL, Kuo G, Weiner AJ, Overby LR, Bradley DW, Houghton M (1989) Isolation of a cDNA clone derived from a blood-borne non-A, non-B viral hepatitis genome. Science 244:359–362
John-Baptiste A, Krahn M, Heathcote J, Laporte A, Tomlinson G (2010) The natural history of hepatitis C infection acquired through injection drug use: meta-analysis and meta-regression. J Hepatol 53:245–251
Kiser JJ, Flexner C (2013) Direct-acting antiviral agents for hepatitis C virus infection. Annu Rev Pharmacol Toxicol 53:427–449
Barbaro G, Di Lorenzo G, Asti A, Ribersani M, Belloni G, Grisorio B, Filice G et al (1999) Hepatocellular mitochondrial alterations in patients with chronic hepatitis C: ultrastructural and biochemical findings. Am J Gastroenterol 94:2198–2205
Paradis V, Kollinger M, Fabre M, Holstege A, Poynard T, Bedossa P (1997) In situ detection of lipid peroxidation by-products in chronic liver diseases. Hepatology 26:135–142
Alvisi G, Madan V, Bartenschlager R (2011) Hepatitis C virus and host cell lipids: an intimate connection. RNA Biol 8:258–269
Farquhar MJ, Harris HJ, McKeating JA (2011) Hepatitis C virus entry and the tetraspanin CD81. Biochem Soc Trans 39:532–536
Moradpour D, Penin F, Rice CM (2007) Replication of hepatitis C virus. Nat Rev Microbiol 5:453–463
Gosert R, Egger D, Lohmann V, Bartenschlager R, Blum HE, Bienz K, Moradpour D (2003) Identification of the hepatitis C virus RNA replication complex in Huh-7 cells harboring subgenomic replicons. J Virol 77:5487–5492
Popescu CI, Rouille Y, Dubuisson J (2011) Hepatitis C virus assembly imaging. Viruses 3:2238–2254
de Chassey B, Navratil V, Tafforeau L, Hiet MS, Aublin-Gex A, Agaugue S, Meiffren G et al (2008) Hepatitis C virus infection protein network. Mol Syst Biol 4:230
• Diamond DL, Syder AJ, Jacobs JM, Sorensen CM, Walters KA, Proll SC, McDermott JE, et al. Temporal proteome and lipidome profiles reveal hepatitis C virus-associated reprogramming of hepatocellular metabolism and bioenergetics. PLoS Pathog 2010;6:e1000719. This paper used the tools of systems biology to directly demonstrate the ability of HCV to reprogram a number of metabolic cellular functions related to mitochondrial energy production, fatty acid oxidation and cell survival
D’Agostino DM, Bernardi P, Chieco-Bianchi L, Ciminale V (2005) Mitochondria as functional targets of proteins coded by human tumor viruses. Adv Cancer Res 94:87–142
Schwer B, Ren S, Pietschmann T, Kartenbeck J, Kaehlcke K, Bartenschlager R, Yen TS et al (2004) Targeting of hepatitis C virus core protein to mitochondria through a novel C-terminal localization motif. J Virol 78:7958–7968
Suzuki R, Sakamoto S, Tsutsumi T, Rikimaru A, Tanaka K, Shimoike T, Moriishi K et al (2005) Molecular determinants for subcellular localization of hepatitis C virus core protein. J Virol 79:1271–1281
Okuda M, Li K, Beard MR, Showalter LA, Scholle F, Lemon SM, Weinman SA (2002) Mitochondrial injury, oxidative stress, and antioxidant gene expression are induced by hepatitis C virus core protein. Gastroenterology 122:366–375
Korenaga M, Wang T, Li Y, Showalter LA, Chan T, Sun J, Weinman SA (2005) Hepatitis C virus core protein inhibits mitochondrial electron transport and increases reactive oxygen species (ROS) production. J Biol Chem 280:37481–37488
Chu VC, Bhattacharya S, Nomoto A, Lin J, Zaidi SK, Oberley TD, Weinman SA et al (2011) Persistent expression of hepatitis C virus non-structural proteins leads to increased autophagy and mitochondrial injury in human hepatoma cells. PLoS One 6:e28551
McLauchlan J, Hepatitis C (2009) virus: viral proteins on the move. Biochem Soc Trans 37:986–990
Barba G, Harper F, Harada T, Kohara M, Goulinet S, Matsuura Y, Eder G et al (1997) Hepatitis C virus core protein shows a cytoplasmic localization and associates to cellular lipid storage droplets. Proc Natl Acad Sci USA 94:1200–1205
Nomura-Takigawa Y, Nagano-Fujii M, Deng L, Kitazawa S, Ishido S, Sada K, Hotta H (2006) Non-structural protein 4A of hepatitis C virus accumulates on mitochondria and renders the cells prone to undergoing mitochondria-mediated apoptosis. J Gen Virol 87:1935–1945
Li XD, Sun L, Seth RB, Pineda G, Chen ZJ (2005) Hepatitis C virus protease NS3/4A cleaves mitochondrial antiviral signaling protein off the mitochondria to evade innate immunity. Proc Natl Acad Sci USA 102:17717–17722
Loo YM, Owen DM, Li K, Erickson AK, Johnson CL, Fish PM, Carney DS et al (2006) Viral and therapeutic control of IFN-beta promoter stimulator 1 during hepatitis C virus infection. Proc Natl Acad Sci USA 103:6001–6006
Griffin S, Clarke D, McCormick C, Rowlands D, Harris M (2005) Signal peptide cleavage and internal targeting signals direct the hepatitis C virus p7 protein to distinct intracellular membranes. J Virol 79:15525–15536
Serejo F, Emerit I, Filipe PM, Fernandes AC, Costa MA, Freitas JP, de Moura MC (2003) Oxidative stress in chronic hepatitis C: the effect of interferon therapy and correlation with pathological features. Can J Gastroenterol 17:644–650
Yadav D, Hertan HI, Schweitzer P, Norkus EP, Pitchumoni CS (2002) Serum and liver micronutrient antioxidants and serum oxidative stress in patients with chronic hepatitis C. Am J Gastroenterol 97:2634–2639
Jain SK, Pemberton PW, Smith A, McMahon RF, Burrows PC, Aboutwerat A, Warnes TW (2002) Oxidative stress in chronic hepatitis C: not just a feature of late stage disease. J Hepatol 36:805–811
Boya P, de la Pena A, Beloqui O, Larrea E, Conchillo M, Castelruiz Y, Civeira MP et al (1999) Antioxidant status and glutathione metabolism in peripheral blood mononuclear cells from patients with chronic hepatitis C. J Hepatol 31:808–814
Vendemiale G, Grattagliano I, Portincasa P, Serviddio G, Palasciamo G, Altomare E (2001) Oxidative stress in symptom-free HCV carriers: relation with ALT flare-up. Eur J Clin Invest 31:54–63
Cardin R, Saccoccio G, Masutti F, Bellentani S, Farinati F, Tiribelli C (2001) DNA oxidative damage in leukocytes correlates with the severity of HCV-related liver disease: validation in an open population study. J Hepatol 34:587–592
Mahmood S, Kawanaka M, Kamei A, Izumi A, Nakata K, Niiyama G, Ikeda H et al (2004) Immunohistochemical evaluation of oxidative stress markers in chronic hepatitis C. Antioxid Redox Signal 6:19–24
Barbaro G, Di Lorenzo G, Ribersani M, Soldini M, Giancaspro G, Bellomo G, Belloni G et al (1999) Serum ferritin and hepatic glutathione concentrations in chronic hepatitis C patients related to the hepatitis C virus genotype. J Hepatol 30:774–782
Sumida Y, Nakashima T, Yoh T, Nakajima Y, Ishikawa H, Mitsuyoshi H, Sakamoto Y et al (2000) Serum thioredoxin levels as an indicator of oxidative stress in patients with hepatitis C virus infection. J Hepatol 33:616–622
Larrea E, Beloqui O, Munoz-Navas MA, Civeira MP, Prieto J (1998) Superoxide dismutase in patients with chronic hepatitis C virus infection. Free Radic Biol Med 24:1235–1241
Valgimigli M, Valgimigli L, Trere D, Gaiani S, Pedulli GF, Gramantieri L, Bolondi L (2002) Oxidative stress EPR measurement in human liver by radical-probe technique. Correlation with etiology, histology and cell proliferation. Free Radic Res 36:939–948
Wang T, Weinman SA (2006) Causes and consequences of mitochondrial reactive oxygen species generation in hepatitis C. J Gastroenterol Hepatol 21(Suppl 3):S34–S37
Koike K, Miyoshi H (2006) Oxidative stress and hepatitis C viral infection. Hepatol Res 34:65–73
Vidali M, Tripodi MF, Ivaldi A, Zampino R, Occhino G, Restivo L, Sutti S et al (2008) Interplay between oxidative stress and hepatic steatosis in the progression of chronic hepatitis C. J Hepatol 48:399–406
Mitsuyoshi H, Itoh Y, Sumida Y, Minami M, Yasui K, Nakashima T, Okanoue T (2008) Evidence of oxidative stress as a cofactor in the development of insulin resistance in patients with chronic hepatitis C. Hepatol Res 38:348–353
Maki A, Kono H, Gupta M, Asakawa M, Suzuki T, Matsuda M, Fujii H et al (2007) Predictive power of biomarkers of oxidative stress and inflammation in patients with hepatitis C virus-associated hepatocellular carcinoma. Ann Surg Oncol 14:1182–1190
Siu L, Foont J, Wands JR (2009) Hepatitis C virus and alcohol. Semin Liver Dis 29:188–199
Nguyen GC, Sam J, Thuluvath PJ (2008) Hepatitis C is a predictor of acute liver injury among hospitalizations for acetaminophen overdose in the United States: a nationwide analysis. Hepatology 48:1336–1341
Moriya K, Nakagawa K, Santa T, Shintani Y, Fujie H, Miyoshi H, Tsutsumi T et al (2001) Oxidative stress in the absence of inflammation in a mouse model for hepatitis C virus-associated hepatocarcinogenesis. Cancer Res 61:4365–4370
Joyce MA, Walters KA, Lamb SE, Yeh MM, Zhu LF, Kneteman N, Doyle JS et al (2009) HCV induces oxidative and ER stress, and sensitizes infected cells to apoptosis in SCID/Alb-uPA mice. PLoS Pathog 5:e1000291
Otani K, Korenaga M, Beard MR, Li K, Qian T, Showalter LA, Singh AK et al (2005) Hepatitis C virus core protein, cytochrome P450 2E1, and alcohol produce combined mitochondrial injury and cytotoxicity in hepatoma cells. Gastroenterology 128:96–107
Ando M, Korenaga M, Hino K, Ikeda M, Kato N, Nishina S, Hidaka I et al (2008) Mitochondrial electron transport inhibition in full genomic hepatitis C virus replicon cells is restored by reducing viral replication. Liver Int 28:1158–1166
Piccoli C, Scrima R, Quarato G, D’Aprile A, Ripoli M, Lecce L, Boffoli D et al (2007) Hepatitis C virus protein expression causes calcium-mediated mitochondrial bioenergetic dysfunction and nitro-oxidative stress. Hepatology 46:58–65
Wang T, Campbell RV, Yi MK, Lemon SM, Weinman SA (2010) Role of hepatitis C virus core protein in viral-induced mitochondrial dysfunction. J Viral Hepat 17:784–793
Benali-Furet NL, Chami M, Houel L, De Giorgi F, Vernejoul F, Lagorce D, Buscail L et al (2005) Hepatitis C virus core triggers apoptosis in liver cells by inducing ER stress and ER calcium depletion. Oncogene 24:4921–4933
Tardif KD, Waris G, Siddiqui A (2005) Hepatitis C virus, ER stress, and oxidative stress. Trends Microbiol 13:159–163
Qadri I, Iwahashi M, Capasso JM, Hopken MW, Flores S, Schaack J, Simon FR (2004) Induced oxidative stress and activated expression of manganese superoxide dismutase during hepatitis C virus replication: role of JNK, p38 MAPK and AP-1. Biochem J 378:919–928
Li Y, Boehning DF, Qian T, Popov VL, Weinman SA (2007) Hepatitis C virus core protein increases mitochondrial ROS production by stimulation of Ca2+ uniporter activity. FASEB J 21:2474–2485
Machida K, Cheng KT, Lai CK, Jeng KS, Sung VM, Lai MM (2006) Hepatitis C virus triggers mitochondrial permeability transition with production of reactive oxygen species, leading to DNA damage and STAT3 activation. J Virol 80:7199–7207
Tardif KD, Mori K, Siddiqui A (2002) Hepatitis C virus subgenomic replicons induce endoplasmic reticulum stress activating an intracellular signaling pathway. J Virol 76:7453–7459
Beer SM, Taylor ER, Brown SE, Dahm CC, Costa NJ, Runswick MJ, Murphy MP (2004) Glutaredoxin 2 catalyzes the reversible oxidation and glutathionylation of mitochondrial membrane thiol proteins: implications for mitochondrial redox regulation and antioxidant DEFENSE. J Biol Chem 279:47939–47951
Piccoli C, Quarato G, Ripoli M, D’Aprile A, Scrima R, Cela O, Boffoli D et al (2009) HCV infection induces mitochondrial bioenergetic unbalance: causes and effects. Biochim Biophys Acta 1787:539–546
•• De Stefani D, Raffaello A, Teardo E, Szabo I, Rizzuto R (2011) A forty-kilodalton protein of the inner membrane is the mitochondrial calcium uniporter. Nature 476:336–340. This landmark paper was the first to identify the mitochondrial calcium uniporter. This protein had been postulated to exist based on more than 40 years of functional studies. Alteration of its function is one mechanism by which HCV increases mitochondrial ROS production
Rizzuto R, De Stefani D, Raffaello A, Mammucari C (2012) Mitochondria as sensors and regulators of calcium signalling. Nat Rev Mol Cell Biol 13:566–578
Gong G, Waris G, Tanveer R, Siddiqui A (2001) Human hepatitis C virus NS5A protein alters intracellular calcium levels, induces oxidative stress, and activates STAT-3 and NF-kappa B. Proc Natl Acad Sci USA 98:9599–9604
Dionisio N, Garcia-Mediavilla MV, Sanchez-Campos S, Majano PL, Benedicto I, Rosado JA, Salido GM et al (2009) Hepatitis C virus NS5A and core proteins induce oxidative stress-mediated calcium signalling alterations in hepatocytes. J Hepatol 50:872–882
Robinson LC, Marchant JS (2008) Enhanced Ca2+ leak from ER Ca2+ stores induced by hepatitis C NS5A protein. Biochem Biophys Res Commun 368:593–599
Horner SM, Gale M Jr (2009) Intracellular innate immune cascades and interferon defenses that control hepatitis C virus. J Interferon Cytokine Res 29:489–498
Bureau C, Bernad J, Chaouche N, Orfila C, Beraud M, Gonindard C, Alric L et al (2001) Nonstructural 3 protein of hepatitis C virus triggers an oxidative burst in human monocytes via activation of NADPH oxidase. J Biol Chem 276:23077–23083
Boudreau HE, Emerson SU, Korzeniowska A, Jendrysik MA, Leto TL (2009) Hepatitis C virus (HCV) proteins induce NADPH oxidase 4 expression in a transforming growth factor beta-dependent manner: a new contributor to HCV-induced oxidative stress. J Virol 83:12934–12946
• de Mochel NS, Seronello S, Wang SH, Ito C, Zheng JX, Liang TJ, Lambeth JD, et al. (2010) Hepatocyte NAD(P)H oxidases as an endogenous source of reactive oxygen species during hepatitis C virus infection. Hepatology 52:47–59. This paper was the first to conclusively demonstrate non-mitochondrial sources for the HCV-induced increase in ROS production
Nishina S, Hino K, Korenaga M, Vecchi C, Pietrangelo A, Mizukami Y, Furutani T et al (2008) Hepatitis C virus-induced reactive oxygen species raise hepatic iron level in mice by reducing hepcidin transcription. Gastroenterology 134:226–238
Kotta-Loizou I, Vassilaki N, Pissas G, Kakkanas A, Bakiri L, Bartenschlager R, Mavromara P (2013) Hepatitis C virus core+1/ARF protein decreases hepcidin transcription through an AP1 binding site. J Gen Virol. doi:10.1099/vir.0.050328-0
Furutani T, Hino K, Okuda M, Gondo T, Nishina S, Kitase A, Korenaga M et al (2006) Hepatic iron overload induces hepatocellular carcinoma in transgenic mice expressing the hepatitis C virus polyprotein. Gastroenterology 130:2087–2098
Moriya K, Miyoshi H, Shinzawa S, Tsutsumi T, Fujie H, Goto K, Shintani Y et al (2010) Hepatitis C virus core protein compromises iron-induced activation of antioxidants in mice and HepG2 cells. J Med Virol 82:776–792
Kang KW, Lee SJ, Kim SG (2005) Molecular mechanism of nrf2 activation by oxidative stress. Antioxid Redox Signal 7:1664–1673
Klaassen CD, Reisman SA (2010) Nrf2 the rescue: effects of the antioxidative/electrophilic response on the liver. Toxicol Appl Pharmacol 244:57–65
Burdette D, Olivarez M, Waris G (2010) Activation of transcription factor Nrf2 by hepatitis C virus induces the cell-survival pathway. J Gen Virol 91:681–690
Ivanov AV, Smirnova OA, Ivanova ON, Masalova OV, Kochetkov SN, Isaguliants MG (2011) Hepatitis C virus proteins activate NRF2/ARE pathway by distinct ROS-dependent and independent mechanisms in HUH7 cells. PLoS One 6:e24957
Carvajal-Yepes M, Himmelsbach K, Schaedler S, Ploen D, Krause J, Ludwig L, Weiss T et al (2011) Hepatitis C virus impairs the induction of cytoprotective Nrf2 target genes by delocalization of small Maf proteins. J Biol Chem 286:8941–8951
• Tikhanovich I, Kuravi S, Campbell RV, Kharbanda K, Artigues A, Villar MT, Weinman SA (2013) Regulation of FOXO3 by phosphorylation and methylation in Hepatitis C virus infection and alcohol exposure. Hepatology. in press. A novel isoelectric focusing method was used to demonstrate how interacting post-translational modifications of the transcription factor FOXO3 result in viral control of the production of the mitochondrial antioxidant protein SOD2
Arnoult D, Soares F, Tattoli I, Girardin SE (2011) Mitochondria in innate immunity. EMBO Rep 12:901–910
Seth RB, Sun L, Ea CK, Chen ZJ (2005) Identification and characterization of MAVS, a mitochondrial antiviral signaling protein that activates NF-kappaB and IRF 3. Cell 122:669–682
Heim MH (2013) Innate immunity and HCV. J Hepatol 58:564–574
•• Horner SM, Liu HM, Park HS, Briley J, Gale M, Jr (2011) Mitochondrial-associated endoplasmic reticulum membranes (MAM) form innate immune synapses and are targeted by hepatitis C virus. Proc Natl Acad Sci USA 108:14590–14595. This elegant study showed that only a fraction of the mitochondrial MAVS protein was involved in the innate immune signaling triggered by HCV RNA binding to RIG-I. This fraction was specifically localized to the MAM component of the ER that contacts the mitohcondrial outer membrane. This paper introduces the concept of an innate immune “synapse” between the ER and the mitochondria at which HCV proteins exert their effects
Horner SM, Park HS, Gale M Jr (2012) Control of innate immune signaling and membrane targeting by the hepatitis C virus NS3/4A protease are governed by the NS3 helix alpha0. J Virol 86:3112–3120
Aweya JJ, Tan YJ (2011) Modulation of programmed cell death pathways by the hepatitis C virus. Front Biosci 16:608–618
Deng Z, Yan H, Hu J, Zhang S, Peng P, Liu Q, Guo D (2012) Hepatitis C virus sensitizes host cells to TRAIL-induced apoptosis by up-regulating DR4 and DR5 via a MEK1-dependent pathway. PLoS ONE 7:e37700
Deng L, Adachi T, Kitayama K, Bungyoku Y, Kitazawa S, Ishido S, Shoji I et al (2008) Hepatitis C virus infection induces apoptosis through a Bax-triggered, mitochondrion-mediated, caspase 3-dependent pathway. J Virol 82:10375–10385
Dang SS, Sun MZ, Yang E, Xun M, Ma L, Jia ZS, Wang WJ et al (2011) Prohibitin is overexpressed in Huh-7-HCV and Huh-7.5-HCV cells harboring in vitro transcribed full-length hepatitis C virus RNA. Virol J 8:424
Tsutsumi T, Matsuda M, Aizaki H, Moriya K, Miyoshi H, Fujie H, Shintani Y et al (2009) Proteomics analysis of mitochondrial proteins reveals overexpression of a mitochondrial protein chaperon, prohibitin, in cells expressing hepatitis C virus core protein. Hepatology 50:378–386
Dreux M, Chisari FV (2011) Impact of the autophagy machinery on hepatitis C virus infection. Viruses 3:1342–1357
Ding WX, Yin XM (2012) Mitophagy: mechanisms, pathophysiological roles, and analysis. Biol Chem 393:547–564
Koh H, Chung J (2012) PINK1 as a molecular checkpoint in the maintenance of mitochondrial function and integrity. Mol Cells 34:7–13
• Kim SJ, Syed GH, Siddiqui A (2013) Hepatitis C virus induces the mitochondrial translocation of Parkin and subsequent mitophagy. PLoS Pathog 9:e1003285. The first demonstration of a direct effect of HCV on a key mechanism responsible for mitochondrial turnover and quality control
Hara Y, Yanatori I, Kiyokage E, Nishina S, Tomiyama Y, Toida K, Ikeda M, et al. Hepatitis C virus core protein suppresses mitophagy by interacting with Parkin. In: 19th International symposium on hepatitis C virus and related viruses. Venice, Italy; 2012. p. 80
Ke PY, Chen SS (2012) Hepatitis C virus and cellular stress response: implications to molecular pathogenesis of liver diseases. Viruses 4:2251–2290
Vidali M, Occhino G, Ivaldi A, Rigamonti C, Sartori M, Albano E (2008) Combination of oxidative stress and steatosis is a risk factor for fibrosis in alcohol-drinking patients with chronic hepatitis C. Am J Gastroenterol 103:147–153
Bartsch H, Nair J (2004) Oxidative stress and lipid peroxidation-derived DNA-lesions in inflammation driven carcinogenesis. Cancer Detect Prev 28:385–391
Choi J, Ou JH (2006) Mechanisms of liver injury. III. Oxidative stress in the pathogenesis of hepatitis C virus. Am J Physiol Gastrointest Liver Physiol 290:G847–G851
Choi J, Lee KJ, Zheng Y, Yamaga AK, Lai MM, Ou JH (2004) Reactive oxygen species suppress hepatitis C virus RNA replication in human hepatoma cells. Hepatology 39:81–89
Huang H, Chen Y, Ye J (2007) Inhibition of hepatitis C virus replication by peroxidation of arachidonate and restoration by vitamin E. Proc Natl Acad Sci USA 104:18666–18670
Choi J, Forman HJ, Ou JH, Lai MM, Seronello S, Nandipati A (2006) Redox modulation of the hepatitis C virus replication complex is calcium dependent. Free Radic Biol Med 41:1488–1498
Singal AK, Jampana SC, Weinman SA (2011) Antioxidants as therapeutic agents for liver disease. Liver International 31:1432–1448
Acknowledgments
The authors thank Drs. Michiari Okuda, Kazuhiro Otani, Masaaki Korenaga, and Roosevelt Campbell for their direct contributions to the work from the Author’s lab, Dr. Keisuke Hino for discussion of unpublished work, and Dr. Stanley Lemon for guidance and helpful discussions over many years. The study in the Author’s lab was supported by Grant AA012863 from the National Institute on Alcoholism and Alcohol Abuse and by a Grant from the Hubert and Richard Hanlon Trust.
Compliance with Ethics Guidelines
This article does not contain any studies with human or animal subjects performed by any of the authors.
Disclosure
Ting Wang and Steven A. Weinman declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wang, T., Weinman, S.A. Interactions Between Hepatitis C Virus and Mitochondria: Impact on Pathogenesis and Innate Immunity. Curr Pathobiol Rep 1, 179–187 (2013). https://doi.org/10.1007/s40139-013-0024-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40139-013-0024-9