
Abstract
Purpose of Review
Maxillectomy for ablative surgery results in defects with significant functional and cosmetic morbidity. The hard or soft palate, dental arch, alveolus, nose, zygoma, malar process, or orbits may be involved, each with attendant considerations. Prosthodontic rehabilitation with a metallic and acrylic obturator has classically been used to replace missing teeth and separate the oral cavity from the nasal cavity and maxillary sinuses. Microvascular free tissue transfer has emerged as the current mainstay of treatment for patients needing composite reconstruction, especially where bony support is needed.
Recent Findings
Technical refinements in skin paddle design, muscle flap orientation, and bone fixation have dominated the literature over the past two decades. Recently, advances in microvascular techniques using virtual surgical planning and navigation-guided implant surgery have improved predictability of dental rehabilitation.
Summary
The current state of the art remains comprehensive functional and cosmetic rehabilitation, comprising facial support, definitive obturation of the oronasal and/or oroantral defect, and functional dental occlusion.




Similar content being viewed by others

References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Louis PJ. Management of panfacial fractures. In: Miloro M, Ghali G, Larsen PE, Waite PD, editors. Peterson’s principles of oral and maxillofacial surgery. Hamilton: BC Decker; 2004. p. 547–59.
Lenox ND, Kim DD. Maxillary reconstruction. Oral Maxillofac Surg Clin N Am. 2013;25(2):215–22.
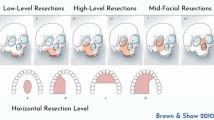
•• Brown JS, et al. A modified classification for the maxillectomy defect. Head Neck. 2000;22(1):17–26. Brown et al. developed the first translational classification system, using language common to both prosthodontists and head and neck surgeons. A four-part numeric scale describes the extent of the vertical defect (globe, nasal, and upper lip support—important to surgeons), and a three-part, lettered horizontal system characterizes the horizontal component (dentoalveolar structures—important to dentists).
•• Andrades P, et al. Current strategies in reconstruction of maxillectomy defects. Arch Otolaryngol Head Neck Surg. 2011;137(8):806–12. This review covers in detail the breadth and complexity of the topic of maxillectomy defect reconstruction, with emphasis on the Cordeiro classification system.
Laraway DC, Rogers SN. A structured review of journal articles reporting outcomes using the University of Washington Quality of Life Scale. Br J Oral Maxillofac Surg. 2012;50(2):122–31.
Kumar P, et al. Assessment of the quality of life in maxillectomy patients: a longitudinal study. J Adv Prosthodont. 2013;5(1):29–35.
List MA, Ritter-Sterr C, Lansky SB. A performance status scale for head and neck cancer patients. Cancer. 1990;66(3):564–9.
Nicoletti G, et al. Chewing and swallowing after surgical treatment for oral cancer: functional evaluation in 196 selected cases. Plast Reconstr Surg. 2004;114(2):329–38.
Aramany MA. Basic principles of obturator design for partially edentulous patients. Part II: design principles. J Prosthet Dent. 1978;40(6):656–62.
Aramany MA. Basic principles of obturator design for partially edentulous patients. Part I: classification. J Prosthet Dent. 1978;40(5):554–7.
Spiro RH, Strong EW, Shah JP. Maxillectomy and its classification. Head Neck. 1997;19(4):309–14.
•• Cordeiro PG, Santamaria E. A classification system and algorithm for reconstruction of maxillectomy and midfacial defects. Plast Reconstr Surg. 2000;105(7):2331–46; discussion 2347–8. Cordeiro and Santamaria describe the maxilla as a six-walled hexahedrium, and classify maxillectomy defects based on the walls involved in tumor resection. For surgeons, this algorithm provides an important approach to the three-dimensional challenges of maxillectomy defects. Free tissue transfer is advocated; this is one of few references where the “folded” osteocutaneous forearm flap is advocated, with excellent cosmetic and functional results.
Cordeiro PG, Chen CM. A 15-year review of midface reconstruction after total and subtotal maxillectomy: part II. Technical modifications to maximize aesthetic and functional outcomes. Plast Reconstr Surg. 2012;129(1):139–47.
Cordeiro PG, Chen CM. A 15-year review of midface reconstruction after total and subtotal maxillectomy: part I. Algorithm and outcomes. Plast Reconstr Surg. 2012;129(1):124–36.
•• Okay DJ, et al. Prosthodontic guidelines for surgical reconstruction of the maxilla: a classification system of defects. J Prosthet Dent. 2001;86(4):352–63. Okay, a well-known maxillofacial prosthodontist, describes a complex system similar to the other Urken/Buchbinder systems used in classification of the mandibulectomy defect. Emphasis is placed on the ability of the prosthodontist to reconstruct the alveolar defect using the remaining available teeth, and the impact of midline involvement and excursive occlusal forces on prosthetic stability.
Brown JS, Shaw RJ. Reconstruction of the maxilla and midface: introducing a new classification. Lancet Oncol. 2010;11(10):1001–8.
Urken M, Cheney ML. Atlas of regional and free flaps for head and neck reconstruction. Philadelphia PA: Wolters-Kluwer LWW; 2012.
Yu M, et al. A modified technique for reconstruction of a total maxillary defect. Br J Oral Maxillofac Surg. 2016;54(1):106–8.
Arce K. Buccal fat pad in maxillary reconstruction. Atlas Oral Maxillofac Surg Clin North Am. 2007;15(1):23–32.
Morlandt A, Fernandes R, Ramirez C. Scapula free flap. In: Kademani D, Tiwana P, editors. Atlas of oral and maxillofacial surgery. Missouri: Elsevier Saunders; 2016. p. 1211–21.
Patel UA, Bayles SW, Hayden RE. The submental flap: a modified technique for resident training. Laryngoscope. 2007;117(1):186–9.
Andrades P, et al. Zygomatic-maxillary buttress reconstruction of midface defects with the osteocutaneous radial forearm free flap. Head Neck. 2008;30(10):1295–302.
Swartz WM, et al. The osteocutaneous scapular flap for mandibular and maxillary reconstruction. Plast Reconstr Surg. 1986;77(4):530–45.
Deraemaeker R, Tienen CV, Lejour M, Dor P. The serratus anterior-scapular free flap: a new osteomuscular unit for reconstruction after radical head and neck surgery (abstract). In: Proceedings of the Second Intl Conf on Head and Neck Cancer. 1988.
Coleman JJ 3rd, Sultan MR. The bipedicled osteocutaneous scapula flap: a new subscapular system free flap. Plast Reconstr Surg. 1991;87(4):682–92.
• Yetzer J, Fernandes R. Reconstruction of orbitomaxillary defects. J Oral Maxillofac Surg. 2013;71(2):398–409. Fernandes and Yetzer outline 21 patients reconstructed with a variety of free and local flaps, including some with obturators. Brown class III to VI defects were overall happier with free tissue transfer versus obturation. The authors propose that perforator flaps will offer greater dimensional stability and improved facial contour in the long term, in contrast to myocutaneous flaps which undergo denervation atrophy.
Boyes-Varley JG, et al. A protocol for maxillary reconstruction following oncology resection using zygomatic implants. Int J Prosthodont. 2007;20(5):521–31.
Brown JS. Deep circumflex iliac artery free flap with internal oblique muscle as a new method of immediate reconstruction of maxillectomy defect. Head Neck. 1996;18(5):412–21.
Futran ND. Primary reconstruction of the maxilla following maxillectomy with or without sacrifice of the orbit. J Oral Maxillofac Surg. 2005;63(12):1765–9.
Sakuraba M, et al. Simple maxillary reconstruction using free tissue transfer and prostheses. Plast Reconstr Surg. 2003;111(2):594–8; discussion 599–600.
Rogers SN, et al. Health-related quality of life after maxillectomy: a comparison between prosthetic obturation and free flap. J Oral Maxillofac Surg. 2003;61(2):174–81.
Moreno MA, et al. Microvascular free flap reconstruction versus palatal obturation for maxillectomy defects. Head Neck. 2010;32(7):860–8.
Genden EM, et al. Comparison of functional and quality-of-life outcomes in patients with and without palatomaxillary reconstruction: a preliminary report. Arch Otolaryngol Head Neck Surg. 2003;129(7):775–80.
Holmes JD, Aponte-Wesson R. Dental implants after reconstruction with free tissue transfer. Oral Maxillofac Surg Clin N Am. 2010;22(3):407–18, vii.
Kornblith AB, et al. Quality of life of maxillectomy patients using an obturator prosthesis. Head Neck. 1996;18(4):323–34.
Seignemartin CP, et al. Understandability of speech predicts quality of life among maxillectomy patients restored with obturator prosthesis. J Oral Maxillofac Surg. 2015;73(10):2040–8.
Kreeft AM, et al. Oral function after maxillectomy and reconstruction with an obturator. Int J Oral Maxillofac Surg. 2012;41(11):1387–92.
Chigurupati R, et al. Quality of life after maxillectomy and prosthetic obturator rehabilitation. J Oral Maxillofac Surg. 2013;71(8):1471–8.
Urken ML, et al. Functional evaluation following microvascular oromandibular reconstruction of the oral cancer patient: a comparative study of reconstructed and nonreconstructed patients. Laryngoscope. 1991;101(9):935–50.
Tang JA, Rieger JM, Wolfaardt JF. A review of functional outcomes related to prosthetic treatment after maxillary and mandibular reconstruction in patients with head and neck cancer. Int J Prosthodont. 2008;21(4):337–54.
Cuesta-Gil M, et al. Oral rehabilitation with osseointegrated implants in oncologic patients. J Oral Maxillofac Surg. 2009;67(11):2485–96.
•• Branemark PI, et al. Osseointegrated implants in the treatment of the edentulous jaw. Experience from a 10-year period. Scand J Plast Reconstr Surg Suppl. 1977;16:1–132. Dr. Per Ingvar Branemark is considered the father of osseointegrated implant technology, and is responsible for the worldwide shift from subperiosteal and transmandibular implants to the contemporary root form and zygomatic titanium implants used in dentistry today.
Carrao V, DeMatteis I. Maxillary sinus bone augmentation techniques. Oral Maxillofac Surg Clin North Am. 2015;27(2):245–53.
Vega LG, Gielincki W, Fernandes RP. Zygoma implant reconstruction of acquired maxillary bony defects. Oral Maxillofac Surg Clin N Am. 2013;25(2):223–39.
Frodel JL Jr, et al. Osseointegrated implants: a comparative study of bone thickness in four vascularized bone flaps. Plast Reconstr Surg. 1993;92(3):449–55; discussion 456–8.
•• Moscoso JF, et al. Vascularized bone flaps in oromandibular reconstruction. A comparative anatomic study of bone stock from various donor sites to assess suitability for enosseous dental implants. Arch Otolaryngol Head Neck Surg. 1994;120(1):36–43. In a series of 28 cadavers, a variety of vascularized bone flap sites were assessed for implantability. The most consistent and reliable bone stock for dental implant stability was found in the DCIA, followed by scapula, fibula, and radius respectively.
Shiboski CH, Schmidt BL, Jordan RC. Tongue and tonsil carcinoma: increasing trends in the U.S. population ages 20-44 years. Cancer. 2005;103(9):1843–9.
Goldstein DP, Irish JC. Head and neck squamous cell carcinoma in the young patient. Curr Opin Otolaryngol Head Neck Surg. 2005;13(4):207–11.
Jacobsson M, et al. Integration of titanium implants in irradiated bone. Histologic and clinical study. Ann Otol Rhinol Laryngol. 1988;97(4 Pt 1):337–40.
Santamaria E, et al. A shift from the osteocutaneous fibula flap to the prelaminated osteomucosal fibula flap for maxillary reconstruction. Plast Reconstr Surg. 2012;130(5):1023–30.
• Hirsch DL, et al. Use of computer-aided design and computer-aided manufacturing to produce orthognathically ideal surgical outcomes: a paradigm shift in head and neck reconstruction. J Oral Maxillofac Surg. 2009;67(10):2115–22. Hirsch and colleagues have introduced virtual surgical planning (“VSP”) into contemporary maxillofacial literature. VSP is now widely used in orthognathic and tumor surgery.
Wang YY, et al. Virtual surgical planning in precise maxillary reconstruction with vascularized fibular graft after tumor ablation. J Oral Maxillofac Surg. 2016;74(6):1255–64.
• Roser SM, et al. The accuracy of virtual surgical planning in free fibula mandibular reconstruction: comparison of planned and final results. J Oral Maxillofac Surg. 2010;68(11):2824–32. After VSP gained popularity, Roser et al. confirmed that indeed, preoperative planning using VSP technology in complex mandibular reconstruction (multiple fibula osteotomies) is a precise, and time-saving effort.
•• Levine JP, et al. Jaw in a day: total maxillofacial reconstruction using digital technology. Plast Reconstr Surg. 2013;131(6):1386–91. “Jaw in a Day” is analogous to the “Teeth in a Day” advertised by many implant dentists, where a patient may undergo dental extractions, have immediate implants placed, and a temporary prosthesis in the same day. In an era of increasing public awareness, the “Jaw in a Day” multi-specialty approach offers the most efficient and comprehensive method of rehabilitating a patient’s facial and dental status to their premorbid condition. The traditional methods of dental implant rehabilitation after microvascular free tissue transfer take up to a year or longer.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Dr. Anthony B. Morlandt declares that he has no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Head and Neck Reconstruction.
Rights and permissions
About this article

Cite this article
Morlandt, A.B. Reconstruction of the Maxillectomy Defect. Curr Otorhinolaryngol Rep 4, 201–210 (2016). https://doi.org/10.1007/s40136-016-0130-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40136-016-0130-4