
Abstract
The laryngeal adductor reflex (LAR) is an involuntary protective response to stimuli in the larynx. The superior laryngeal nerve acts as the afferent limb and the recurrent laryngeal nerve as the efferent limb of this reflex, which is modulated by the central nervous system. Perhaps the most clinically significant application of the LAR is its use in laryngopharyngeal (LP) sensory discrimination testing. Importantly, aberrations in the LAR may predict dysphagia or portend clinical phenotypes of chronic cough, vocal cord dysfunction or pediatric apneas. LP sensation is a potential target for interventions addressing the aforementioned conditions though currently remains an area of active investigation.
Similar content being viewed by others

Introduction
In humans, the laryngopharyngeal (LP) complex serves three principle functions: airway protection, respiration and voice production. To accomplish and coordinate these fundamental tasks, we rely on a dynamic and efficient physiologic process generated from interactions of specialized anatomic components. To perform properly, the motor functions of the laryngopharynx are matched in importance by sensory contributions such as those producing the LAR. The primitive, protective function of the LAR to prevent against aspiration has been underscored by the finding that normal individuals maintain the reflex during various vocal tasks [1].
Definition
The laryngeal adductor reflex, also called the glottic closure reflex, is a mechanism of laryngeal protection, preventing material from inappropriately entering the upper airway. Mechanically, it is the bilateral thyroarytenoid (TA) muscle response to mechanical or chemical irritation of the laryngeal mucosa.
Review of Anatomy and Neural Circuitry
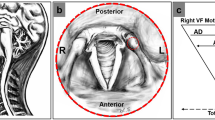
The LAR is a brainstem-mediated, involuntary reflex arc providing airway protection from ingested material [2]. Mechanoreceptors and chemoreceptors in the LP mucosa receive innervation from the internal branch of the SLN, which serves as the afferent component of the LAR [3]. Sensory information is then transduced through the central nervous system via the nucleus tractus solitaries to the ipsilateral nucleus ambiguus in the medulla of the brainstem. The motor neurons within the nucleus ambiguus then project to the recurrent laryngeal nerve (RLN), the efferent component. In response to a unilateral stimulus, a discrete and rapid bilateral contraction of the TA muscles is produced.
Though brief, the neuronal mechanics responsible for this critical reflex are quite complex and have been extensively studied in humans as well as animal models. Much of our modern understanding of the neurophysiology behind the glottic closure reflex is a product of extensive work done in felines and canines by Sasaki and Suzuki during the late 1970s [4–6]. More recently, using a porcine model, Sasaki [7] reported the important finding that the ipsilateral LAR is maintained but the contralateral LAR is extinguished in states of altered consciousness. Contemporary investigations in rodents by Sun and colleagues have suggested that variable ipsilateral and contralateral efferent neuronal activity may be important for the coordination of breathing with the other LP behaviors of swallowing and cough [8].
LAR Testing
The addition of sensory testing to flexible endoscopic evaluation of swallowing (FEES) is termed flexible endoscopic evaluation of swallowing with sensory testing (FEESST). FEESST directly evaluates LP sensation by assessing the ability of a tactile stimulus to elicit the LAR [9, 10, 11∙]. Sensory testing may be grossly performed with the tip of the flexible endoscope or formally quantified with a LP air-pulse stimulator. A pulse of air is delivered to the supraglottic mucosa through a side-channel on the flexible endoscope. Each side is tested individually and is expected to elicit a bilateral response in persons with intact supraglottic sensation.
The pressure of the air-pulse delivered through the endoscope (mmHg) may be varied to quantify the amount of stimulus required to elicit the LAR [9, 12]. Aviv and colleagues [13] described normative sensory thresholds to calibrated pulses of air. An individual with normal LP sensation manifests LAR at a pulse pressure of less than 4 mmHg. Those requiring greater pressure are identified as having moderate (4–6 mmHg) or severe sensory impairment (greater than 6 mmHg). These thresholds correlate with psychophysical testing, or patient-reported sensation of delivered air pulses [14, 15]. Among normal individuals, the average threshold for eliciting the LAR is 2.60 mmHg; this value differs significantly between age groups with an average threshold of 2.06 mmHg in those less than 41 years and 2.97 mmHg in those older than 60 years [16].
A known limitation of LP sensory discrimination testing is poor interobserver agreement between endoscopists, but it is particularly useful in individuals with impaired cognition who are unable to participate in the subjective task of recognizing and confirming the presence of a palpable air pulse [10, 17]. Additionally, it has been shown that nasal anesthetic of either 0.05 % oxymetazoline or 4 % cocaine does not alter laryngeal sensory testing during FEESST [18].
Other means of assessing the integrity of SLN function include traditional electromyography [19] or less invasive, external electrodes that detect surface-evoked laryngeal action potentials [20]. However, the utility and application of such methods continue to be defined and they have yet to be adopted into routine clinical practice.
Clinical Implications
Individuals with a diminished or absent LAR may be at risk for significant clinical consequences. In adults, increased LP sensory thresholds have been observed in those with prolonged tracheostomy, gastroesophageal reflux (GER), obstructive sleep apnea, chronic obstructive pulmonary disease, neurodegenerative disorders and advanced age [16, 21–25]. In these populations, sensory impairment may contribute to the development of dysphagia and aspiration. Furthermore, abnormal LAR thresholds may play a role in the spectrum of laryngeal hypersensitivity disorders such as chronic cough and vocal cord dysfunction [21]. The deleterious effects of altered LP sensation in adult and pediatric patients are reviewed in more detail below.
Dysphagia
In adults, altered LP sensation, especially when bilateral, is a risk for impaired and possibly unsafe swallowing. Aviv and colleagues [26] reported a strong association between pharyngeal motor dysfunction, or abnormal pharyngeal squeeze maneuver (PSM), and decreased LP sensation among patients with dysphagia. They found that isolated pharyngeal motor dysfunction with intact LP sensation predicted penetration and aspiration with substances of pureed consistencies whereas an isolated LP sensory deficit with an intact PSM predicted penetration and aspiration with thin liquids. Furthermore, nearly all patients with an absent LAR and PSM aspirated both thin liquids and purees [27, 28]. In a prospective study of 20 adults with cerebral strokes, Aviv found that an abnormal FEESST, even in the presence of a normal modified barium swallow, was associated with later development of pneumonia [29]. This prompted the author’s recommendation to consider sensory testing as an adjunct in guiding post-stroke dietary management in this population.
Other populations with LP sensory deficits manifested by abnormal LAR may be at particular risk for dysphagia. A study by Tabaee and colleagues reviewed a cohort of individuals with unilateral vocal fold immobility of myriad etiologies. They found that 83 % had abnormal SLN function on FEESST and over one-third with an absent LAR. Such deficits were associated with significantly higher rates of penetration and aspiration during trials of purees [30]. Work by Phua and Aviv and their colleagues has shown that individuals with GER or chronic cough have, on average, elevated LAR thresholds and postulate that, as a consequence, may be at a higher risk of swallowing dysfunction [21, 31].
Chronic Cough and Vocal Cord Dysfunction
It has been proposed that enhanced LP sensitivity may result from neural plasticity in the central nervous system which alters sensorimotor pathways including the LAR [32]. The clinical manifestations of these neurosensory changes have been termed the ‘irritable larynx,’ which is suggested to represent of spectrum of disorders including chronic cough, paradoxical vocal cord motion or vocal cord dysfunction, throat clearing, dysphonia and laryngospasm [32]. Heightened laryngeal sensitivity and decreased LAR thresholds have been reported as sequelae of viral upper respiratory infection [33], irritant exposure [34], GER, psychogenic conditions and tissue injury. Abnormal LAR testing in this population of patients may discriminate individuals with altered sensory thresholds from those who experience exposure to more stimuli or irritants.
Pediatrics
Thompson and colleagues have investigate LP sensation in populations of infants and children. In pediatric patients, they reported that increased LP sensory thresholds, or diminished LAR, resulted in a significantly higher likelihood of laryngeal reflux penetration and aspiration [35]. Furthermore, infants with a history of apneas have been reported to have higher LAR thresholds than their age-matched counterparts [3]. The investigators propose that decreased LP sensitivity results in prolonged and excessive secretion exposure thereby inducing apnea among these infants. In turn, prolonged secretion exposure may promote LP edema, which could further increase LAR thresholds in these infants. Such consequences may represent a potential mechanism for the development of sudden infant death syndrome (SIDS) similar to neonates found to be at high risk for SIDS from apneas secondary to GER [36]. Work in animal models lends support to these clinical observations [37]; however, the cause of SIDS remains speculative.
Interventions
Surgical, medical and behavioral therapies have been proposed for rehabilitation of the impaired LAR. In 1997, Aviv and colleagues [12] reported restoration of normal LAR in two individuals with altered LP sensation following brainstem stokes by performing a neural anastomosis between the great auricular nerve and the superior laryngeal nerve. In a subsequent study, Aviv noted improved LP sensation, measured by LAR thresholds, in patients with laryngopharyngeal reflux (LPR) following the use of a proton pump inhibitor (PPI) [31]. Similar findings were also described in a pediatric population whose LP sensation improved with PPI treatment or Nissen fundoplication [38].
In individuals with primary complaints of cough, symptoms of GER or LPR, or vocal cord dysfunction, a significantly decreased LP sensory threshold was appreciated with the use of PPI and behavioral therapy including respiratory retraining [39∙]. Also, gabapentin, a neuromodulator, has shown to be effective in some individuals with refractory chronic cough or throat clearing [40, 41, 42∙]. Behavioral cough therapy, generally performed by trained speech language pathologists, has demonstrated decreased cough sensitivity, decreased urge to cough and increased cough threshold [43, 44].
Conclusion
Our knowledge of LP sensation and the LAR continues to evolve, and our current understanding of its neuronal circuitry as well as its critical contribution to safe deglutition has influenced clinical application of the LAR, particularly as it is used in FEESST. Efficient and reproducible sensory testing using LAR has enabled implementation of preventative and therapeutic interventions to avoid deleterious consequences of LP sensory dysfunction. In addition to its relationship to dysphagia, impaired LAR is involved in the development and potentiation of chronic cough, vocal cord dysfunction and laryngospasm. Targeting LP sensory contributions to these conditions relies significantly on behavioral therapy and remains an area of active investigation.
References
Papers of particular interest, published recently, have been highlighted as: ∙ Of importance
Henriquez VM, Schulz GM, Bielamowicz S, Ludlow CL. Laryngeal reflex responses are not modulated during human voice and respiratory tasks. J Physiol. 2007;585:779–89.
Ludlow CL, Van Pelt F, Koda J. Characteristics of late responses to superior laryngeal nerve stimulation in humans. Ann Otol Rhinol Laryngol. 1992;101:127–34.
Thompson DM, Rutter MJ, Rudolph CD, Willging JP, Cotton RT. Altered laryngeal sensation: a potential cause of apnea of infancy. Ann Otol Rhinol Laryngol. 2005;114:258–63.
Suzuki M, Sasaki CT. Initiation of reflex glottic closure. Ann Otol Rhinol Laryngol. 1976;85:382–6.
Suzuki M, Sasaki CT. Effect of various sensory stimuli on reflex laryngeal adduction. Ann Otol Rhinol Laryngol. 1977;86:30–6.
Sasaki CT, Suzuki M. Laryngeal reflexes in cat, dog, and man. Arch Otolaryngol. 1976;102:400–2.
Sasaki CT, Yu Z, Xu J, Hundal J, Rosenblatt W. Effects of altered consciousness on the protective glottic closure reflex. Ann Otol Rhinol Laryngol. 2006;115:759–63.
Sun QJ, Chum JM, Bautista TG, Pilowsky PM, Berkowitz RG. Neuronal mechanisms underlying the laryngeal adductor reflex. Ann Otol Rhinol Laryngol. 2011;120:755–60.
Aviv JE, Martin JH, Keen MS, Debell M, Blitzer A. Air pulse quantification of supraglottic and pharyngeal sensation: a new technique. Ann Otol Rhinol Laryngol. 1993;102:777–80.
Aviv JE, Martin JH. Kim Tet al. Laryngopharyngeal sensory discrimination testing and the laryngeal adductor reflex. Ann Otol Rhinol Laryngol. 1999;108:725–30.
∙ Merati AL. In-office evaluation of swallowing: FEES, pharyngeal squeeze maneuver, and FEESST. Otolaryngol Clin North Am 2013;46:31–9. This is a comprehensive review of in-office, endoscopic evaluation of swallowing with a detailed section describing the history and contemporary use of FEEST.
Aviv JE, Mohr JP, Blitzer A, Thomson JE, Close LG. Restoration of laryngopharyngeal sensation by neural anastomosis. Arch Otolaryngol Head Neck Surg. 1997;123:154–60.
Aviv JE, Martin JH, Sacco RL, et al. Supraglottic and pharyngeal sensory abnormalities in stroke patients with dysphagia. Ann Otol Rhinol Laryngol. 1996;105:92–7.
Aviv JE, Martin JH, Kim T, et al. Laryngopharyngeal sensory discrimination testing and the laryngeal adductor reflex. Ann Otol Rhinol Laryngol. 1999;108:725–30.
Bhabu P, Poletto C, Mann E, Bielamowicz S, Ludlow CL. Thyroarytenoid muscle responses to air pressure stimulation of the laryngeal mucosa in humans. Ann Otol Rhinol Laryngol. 2003;112:834–40.
Aviv JE. Effects of aging on sensitivity of the pharyngeal and supraglottic areas. Am J Med. 1997;103:74S–6S.
Cunningham JJ, Halum SL, Butler SG, Postma GN. Intraobserver and interobserver reliability in laryngopharyngeal sensory discrimination thresholds: a pilot study. Ann Otol Rhinol Laryngol. 2007;116:582–8.
Johnson PE, Belafsky PC, Postma GN. Topical nasal anesthesia and laryngopharyngeal sensory testing: a prospective, double-blind crossover study. Ann Otol Rhinol Laryngol. 2003;112:14–6.
Sulica L. The superior laryngeal nerve: function and dysfunction. Otolaryngol Clin North Am. 2004;37:183–201.
Bock JM, Blumin JH, Toohill RJ, Merati AL, Prieto TE, Jaradeh SS. A new noninvasive method for determination of laryngeal sensory function. Laryngoscope. 2011;121:158–63.
Phua SY, McGarvey LP, Ngu MC, Ing AJ. Patients with gastro-oesophageal reflux disease and cough have impaired laryngopharyngeal mechanosensitivity. Thorax. 2005;60:488–91.
Sasaki CT, Suzuki M, Horiuchi M, Kirchner JA. The effect of tracheostomy on the laryngeal closure reflex. Laryngoscope. 1977;87:1428–33.
Nguyen AT, Jobin V, Payne R, Beauregard J, Naor N, Kimoff RJ. Laryngeal and velopharyngeal sensory impairment in obstructive sleep apnea. Sleep. 2005;28:585–93.
Clayton NA, Carnaby-Mann GD, Peters MJ, Ing AJ. The effect of chronic obstructive pulmonary disease on laryngopharyngeal sensitivity. Ear Nose Throat J 2012; 91:370, 372, 374 passim.
Amin MR, Harris D, Cassel SG, Grimes E, Heiman-Patterson T. Sensory testing in the assessment of laryngeal sensation in patients with amyotrophic lateral sclerosis. Ann Otol Rhinol Laryngol. 2006;115:528–34.
Aviv JE, Spitzer J, Cohen M, Ma G, Belafsky P, Close LG. Laryngeal adductor reflex and pharyngeal squeeze as predictors of laryngeal penetration and aspiration. Laryngoscope. 2002;112:338–41.
Setzen M, Cohen MA, Perlman PW, et al. The association between laryngopharyngeal sensory deficits, pharyngeal motor function, and the prevalence of aspiration with thin liquids. Otolaryngol Head Neck Surg. 2003;128:99–102.
Perlman PW, Cohen MA, Setzen M, et al. The risk of aspiration of pureed food as determined by flexible endoscopic evaluation of swallowing with sensory testing. Otolaryngol Head Neck Surg. 2004;130:80–3.
Aviv JE, Sacco RL, Mohr JP. Laryngopharyngeal sensory testing with modified barium swallow as predictors of aspiration pneumonia after stroke. Laryngoscope. 1997;107:1254–60.
Tabaee A, Murry T, Zschommler A, Desloge RB. Flexible endoscopic evaluation of swallowing with sensory testing in patients with unilateral vocal fold immobility: incidence and pathophysiology of aspiration. Laryngoscope. 2005;115:565–9.
Aviv JE, Liu H, Parides M, Kaplan ST, Close LG. Laryngopharyngeal sensory deficits in patients with laryngopharyngeal reflux and dysphagia. Ann Otol Rhinol Laryngol. 2000;109:1000–6.
Morrison M, Rammage L, Emami AJ. The irritable larynx syndrome. J Voice. 1999;13:447–55.
Pratter MR. Cough and the common cold: ACCP evidence-based clinical practice guidelines. Chest. 2006;129:72S–4S.
Hutchings HA, Eccles R, Smith AP, Jawad MS. Voluntary cough suppression as an indication of symptom severity in upper respiratory tract infections. Eur Respir J. 1993;6:1449–54.
Thompson DM. Laryngopharyngeal sensory testing and assessment of airway protection in pediatric patients. Am J Med 2003;115 Suppl 3A:166S–168S.
Amin RS. Gastroesophageal reflux and infant apnea. J Pediatr. 2000;137:298–300.
Bauman NM, Wang D, Jaffe DM, Sandler AD, Luschei ES. Effect of intravenous substance P on laryngeal adductor activity in young dogs. Ann Otol Rhinol Laryngol. 1999;108:112–8.
Suskind DL, Thompson DM, Gulati M, Huddleston P, Liu DC, Baroody FM. Improved infant swallowing after gastroesophageal reflux disease treatment: a function of improved laryngeal sensation? Laryngoscope. 2006;116:1397–403.
∙ Murry T, Branski RC, Yu K, Cukier-Blaj S, Duflo S, Aviv JE. Laryngeal sensory deficits in patients with chronic cough and paradoxical vocal fold movement disorder. Laryngoscope 2010;120:1576–81. This report on a small series of patients strongly implicates altered laryngopharyngeal sensation in the pathophysiology of cough and VCD based on normalization of LAR and symptoms following behavioral and medical (PPI) therapy.
Lee B, Woo P. Chronic cough as a sign of laryngeal sensory neuropathy: diagnosis and treatment. Ann Otol Rhinol Laryngol. 2005;114:253–7.
Van de Kerkhove C, Goeminne PC, Van Bleyenbergh P, Dupont LJ. A cohort description and analysis of the effect of gabapentin on idiopathic cough. Cough. 2012;8:9.
∙ Ryan NM, Birring SS, Gibson PG. Gabapentin for refractory chronic cough: a randomised, double-blind, placebo-controlled trial. Lancet 2012;380:1583–89. This well-designed study shows improved cough-specific quality of life scores and few side effects in refractory cough patients treated with gabapentin compared to placebo.
Ryan NM, Vertigan AE, Gibson PG. Chronic cough and laryngeal dysfunction improve with specific treatment of cough and paradoxical vocal fold movement. Cough. 2009;5:4.
Ryan NM, Vertigan AE, Bone S, Gibson PG. Cough reflex sensitivity improves with speech language pathology management of refractory chronic cough. Cough. 2010;6:5.
Disclosure
Amanda S. Domer, Maggie A. Kuhn, and Peter C. Belafsky declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Domer, A.S., Kuhn, M.A. & Belafsky, P.C. Neurophysiology and Clinical Implications of the Laryngeal Adductor Reflex. Curr Otorhinolaryngol Rep 1, 178–182 (2013). https://doi.org/10.1007/s40136-013-0018-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40136-013-0018-5