
Abstract
Introduction
To describe subclinical angioid streaks (AS) as a frequent, peculiar age-related macular degeneration (AMD) phenotype, comparing features of eyes with subclinical AS with those of eyes with AMD without AS.
Methods
This was a retrospective, observational study. Among a patient cohort with AMD, we selected patients without known causes for AS whose eyes showed signs of angioid streaks (AS) on structural optical coherence tomography (OCT) but not on fundus examination. Selected OCT features of AS were Bruch’s membrane (BM) breaks and large BM dehiscences.
Results
Among 543 eyes of 274 patients with AMD (mean ± standard deviation: 82 ± 7 years), 73 eyes of 46 patients (81 ± 7 years; p = 0.432) showed AS features on OCT (OCT AS) that were not visible on fundus examination. Estimated prevalence of subclinical age-related AS was 13.4% (95% confidence interval 10.3–16.3%) in this AMD population. Fifty-three eyes (73%) with AS features were affected by peripapillary atrophy, often with a “petaloid-like” pattern, similar to typical features of AS disease. Almost all cases (97%) presented reticular pseudodrusen (RPD), with (41%) or without (59%) drusen showing a significant difference in RPD prevalence in OCT AS eyes in comparison to AMD eyes without subclinical AS using generalized estimating equations (P < 0.001). Among the 73 subclinical AS cases, 71 were affected by late AMD (57 with macular neovascularization, 14 with geographic atrophy), showing a more advanced AMD stage in comparison with AMD eyes without subclinical AS (P < 0.001). The following OCT features were disclosed: BM breaks in 100% of cases and BM dehiscences in 37%.
Conclusions
Subclinical AS in eyes with AMD is a peculiar phenotype of the disease, with features suggesting a primary involvement of Bruch’s membrane and clinical similarities with mild, late-onset pseudoxanthoma elasticum.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study |
Age-related macular degeneration (AMD) is characterized by several phenotypes, each with a different pathogenesis and involved pathway(s). |
The aim of this study was to describe subclinical angioid streaks (AS) as a frequent, peculiar phenotype of age-related macular degeneration. |
What was learned from the study |
Observing features of eyes with signs of AS on optical coherence tomography but no visible AS using fundus examination, we reported a new phenotype of AMD, namely subclinical AS in AMD. |
Since Bruch’s membrane likely plays a significant role in subclinical AS etiology, therapeutical approaches can be different from those of typical AMD, particularly with respect to possible new therapies for geographic atrophy. |
Introduction
Age-related macular degeneration (AMD) is a multifactorial disease characterized by a genetic and environmental background. AMD is classified into three different stages (i.e. early, intermediate, and late disease) based on different findings [1, 2]. In the early and intermediate stages of the disease, the macular area is characterized by the presence of drusen, reticular pseudodrusen (RPD), and AMD pigmentation abnormalities [2, 3]. Even if drusen are peculiar findings of AMD, the presence of RPD may also be associated with diseases characterized by primary alteration of Bruch’s membrane (BM), such as Sorsby fundus dystrophy or pseudoxanthoma elasticum (PXE) with angioid streaks (AS) [4–6]. The pathogenesis of AMD is not completely understood. Histological and in vivo imaging studies indicate that important structural changes include the retinal pigment epithelium (RPE) cells, BM, and/or the choriocapillaris [7–12].
Angioid streaks (AS) are characterized by breaks in BM, as firstly proposed by Kofler in 1917 and subsequently demonstrated by histological studies [13–15]. BM breaks are not initially associated with alterations of RPE and choriocapillaris [16]. The pathogenesis of AS is complex but usually related to alterations in calcium homeostasis. The most frequent systemic disease associated with AS is PXE, an inherited disease related to ABCC6 gene mutation [17]. Patients with PXE have lower plasma levels of inorganic pyrophosphate, a factor thought to inhibit calcification of elastic fibers [18, 19]. The systemic alterations in calcium homeostasis promote extracellular matrix mineralization, including in BM [20, 21]. While the diagnosis of AS may be based on fundus examination, more in-depth information is available due to findings from structural optical coherence tomography (OCT) [21, 22]. The usual finding on OCT imaging associated with AS is a break in BM with variable dehiscence [16, 22, 23].
The aim of this study was to characterize demographic, clinical, and multimodal imaging features of patients diagnosed with AMD who presented with AS visible on OCT but not on fundus examination. For this reason, we named this phenotype subclinical AS in AMD. We compared features of subclinical AS in AMD eyes with AMD eyes without AS.
Methods
Study Population
This is a retrospective, observational, and monocentric study conducted at the Medical Retina and Imaging Unit, Department of Ophthalmology, IRCCS San Raffaele Hospital, University Vita-Salute San Raffaele in Milan, Italy. From among all consecutive patients referred to the Unit between September and November 2021, we selected and reviewed medical records of patients aged ≥ 50 years with a diagnosis of AMD in at least one eye. At the time of first diagnosis of AMD, all patients underwent a complete examination, including structural OCT scans; when available, fluorescein (FA) and indocyanine green angiographies (ICGA) were also collected. Exclusion criteria were: the presence of other retinal disorders potentially confounding the clinical assessment (e.g., diabetic retinopathy, retinal vein/artery occlusion, myopia > 6 D); previous ocular surgery in the study eye in the past 6 months; the presence of significant media opacities; prior diagnosis of AS based on fundus examination and/or pictures, infrared reflectance (IR), fundus autofluorescence (FAF) [19]; the known presence of systemic diseases related to AS, including PXE, Paget’s disease, and hemoglobinopathies (sickle cell trait disease and thalassemia).
All patients signed a written general consent approved by the Ethics Committee for inclusion in this retrospective study. The study was conducted in accordance with the Declaration of Helsinki for research involving human subjects. Due to the retrospective nature of the study, the study does not require a specific Ethics Committee Approval according to Italian laws.
Study Protocol
All subjects underwent a comprehensive ophthalmic evaluation, including assessment of distance best-corrected visual acuity (BCVA) using Snellen charts and converted to LogMAR for statistical evaluation, Goldmann applanation tonometry, slit lamp biomicroscopy, dilated fundus examination, multicolor imaging, and spectral-domain structural OCT with enhanced depth imaging (EDI) (Heidelberg Spectralis HR2 + OCT; Heidelberg Engineering, Heidelberg, Germany) of the macular and peripapillary area. FA and ICGA using the Heidelberg Spectralis OCT system (HRA2 + OCT; Heidelberg Engineering) and/or Swept Source OCT-angiography (SS-OCT-A) using the PLEXElite 9000 system (Carl Zeiss, Meditec Inc., Dublin, CA, USA) were performed to detect the presence of macular neovascularization (MNV) at baseline.
Grading Process
Two independent and experienced retinal readers (RS, IZ) analyzed all images. The aim of the grading process was to detect subclinical age-related AS based on structural OCT findings. Since there is no established consensus on subclinical AS expected to become a new clinical entity, the two graders employed OCT criteria previously described for AS [19–22]: BM undulations; BM breaks (i.e., interruption of BM detected by structural OCT); and large dehiscences of BM (i.e., interruption of BM > 250 μm, not contiguous with AS) (Fig. 1). However, a diagnosis of subclinical AS was made if the following criteria were confirmed: (1) the presence of AS evidenced by OCT signs (AS OCT), such as BM breaks and/or large dehiscences of BM; (2) the absence of AS based on fundus photography.

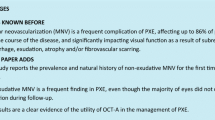
Structural optical coherence tomography (OCT) of a patient affected by neovascular age-related macular degeneration (AMD) with subclinical angioid streaks (AS) in the left eye. a–d Combined infrared reflectance and structural OCT B-scans passing through the fovea showing Bruch’s membrane (BM) dehiscences (a; red line), BM breaks (b, c; yellow triangles), and BM undulations (a, b, d; yellow asterisks)
The two retinal readers performed grading in an independent and blinded fashion, following which they met to compare the level of agreement; disagreements were resolved by further discussion and open adjudication to yield a single assessment for each case. In cases in which the two graders did not agree on a single consensus result, the final decision was made by a third expert in retinal disorders (GQ). Finally, a single grader (BT) evaluated OCT images at baseline for qualitative and quantitative features, including central macular thickness (CMT), subfoveal choroidal thickness (ChT), and type of MNV. CMT was automatically assessed within a 1-mm Early Treatment Diabetic Retinopathy Study (ETDRS) circle centered on the fovea by using the mapping protocol of the OCT software. Subfoveal ChT was measured in structural EDI OCT with the built-in caliper in the foveal location as the vertical distance between the hyper-reflective line of BM and hyporeflective line, corresponding to the sclero-choroidal interface, perpendicular to the RPE.
Statistical Analyses
Statistical calculations were carried out using the Statistical Package for the Social Sciences (SPSS) version 28.0.1.0 software package (SPSS IBM Corp., Armonk, NY, USA). The P-value cutoff point for statistical significance was set at 0.05. All continuous variables were tested for normal distributions using Shapiro–Wilk’s normality test. Descriptive statistics of continuous variables were expressed as the mean ± standard deviation (SD). Categorical variables were reported as frequency and percentage proportions. Differences in the mean (± SD) between two normally distributed quantitative variables at the patient level were analyzed using a Student t-test for independent samples. The significance of the difference between the proportions of independent categorical variables at the patient level was analyzed with Pearson’s Chi-square test. Because outcomes were collected for each eye, for all analyses at the eye level the generalized estimation equation (GEE) was used to correct the intra-ocular dependence of the patients. Inter-rater reliability between two graders (RS, IZ) was assessed by Cohen's kappa coefficient (κ), and considered to be poor, moderate, good, or excellent at κ < 0.50, κ > 0.50 and < 0.75, κ > 0.75 and < 0.90, or κ > 0.90, respectively.
Results
All 274 screened patients affected by AMD were Caucasian. Of the 543 screened eyes of these 274 patients with AMD(188 females, 86 males; mean [± SD] age 81 ± 7 years), 73 eyes of 46 patients (34 females, 12 males; mean age 82 ± 7 years) showed sub-clinical AS features using structural OCT and were included in the analysis (Figs. 2, 3, 4, 5). Therefore, estimated prevalence of subclinical age-related AS in our study cohort was 13.4% (95% confidence interval [CI] 10.3–16.3%). Absence of AS was confirmed by two graders (RS, IZ) on fundus examination, multicolor imaging, IR, and fundus autofluorescence [19]. No statistically significant difference in age and sex was found between patients with other phenotypes of AMD and subclinical AS (P = 0.432 and P = 0.231, respectively) (Table 1). Among the 46 patients included in the study, the fellow eyes of 19 patients were not included for absence of AS breaks/dehiscence (15 patients), the presence of macular hole (2 patients), presence of low-quality images (1 patient), and presence of only one eye (1 patient was monocle due to a childhood trauma).

Multimodal imaging evaluation of a patient affected by geographic atrophy (GA) with reticular pseudodrusen (RPD) and a subclinical AS phenotype in the left eye. a, b Pseudocolor imaging (a) and fundus autofluorescence (b) showing GA lesion in the macular area, peripapillary atrophy, and absence of visible AS. c Structural OCT B-scan passing through the fovea showing area of outer retina and retinal pigment epithelium atrophy (i.e., complete retinal pigment epithelium and outer retinal atrophy [cRORA]) (yellow arrows) and RPD (yellow circle). d Horizontal structural OCT passing in the peripapillary area showing a pigment epithelium detachment with a large peripapillary BM dehiscence (yellow asterisks)

Multimodal imaging evaluation of a patient affected by intermediate AMD with RPD and a subclinical AS phenotype in the left eye. a, b Fundus autofluorescence (a) and pseudocolor imaging (b) showing peripapillary atrophy with a “petaloid-like” pattern characterized by a multilobular hypoautofluorescence around the peripapillary area, and absence of visible AS. c Combined IR and structural OCT B-scan passing through optic nerve showing a BM break (yellow triangles). d Structural OCT passing through the fovea showing the presence of RPD (yellow circle)

Multimodal imaging evaluation of a patient affected by neovascular AMD and a subclinical AS phenotype in the left eye. a, b Fundus autofluorescence (a) and pseudocolor imaging (b) showing macular atrophy, peripapillary atrophy, and absence of visible AS. c Combined IR and structural OCT B-scan passing through optic nerve showing a BM break (yellow triangles). d Structural OCT passing through the fovea showing the presence of neovascular AMD and macular atrophy

Multimodal imaging evaluation of a patient affected by neovascular AMD and a subclinical AS phenotype in the right eye. a, b Pseudocolor imaging (a) and fundus autofluorescence (b) showing macular atrophy, peripapillary atrophy with a “petaloid-like” pattern characterized by a multilobular hypoautofluorescence around the peripapillary area, and absence of visible AS. c Combined IR and structural OCT B-scan passing through optic nerve showing a Bruch’s membrane break (yellow triangle). d Structural OCT passing through the fovea showing the presence of neovascular AMD and macular atrophy
Mean (± SD) BCVA was about 20/63 Snellen equivalent (0.57 ± 0.44 LogMAR), mean CMT was 330 ± 125 μm, and mean subfoveal ChT was 162 ± 64 μm. Of the 73 eyes with AMD and subclinical AS, 55 (73%) showed peripapillary atrophy, which in several cases (36%) was characterized by a “petaloid-like” pattern of atrophy, characterized by a multilobular hypoautofluorescence around the peripapillary area.
Of the 73 eyes with AMD and features of subclinical AS, 57 (78%) were affected by MNV (Figs. 4, 5), 14 eyes (19%) were affected by GA (Fig. 2), and two eyes (3%) were not affected by either MNV or GA (diagnosed as intermediate AMD) (Fig. 3). Interestingly, the distribution among these three stages was significantly different in comparison with eyes with AMD but without OCT features of subclinical AS (Exp(B) = 0.204; P < 0.001) (Table 1); eyes with subclinical AS were usually characterized by a more advanced stage of AMD (i.e., presence of MNV or GA) (P < 0.001). Among the 57 eyes with subclinical AS and MNV, 70% (38/54) displayed a type 1 MNV, 24% (13 eyes) displayed a type 2 MNV, 9% (5 eyes) displayed a mixed type 1 and 2 MNV, and 2% (1 eyes) displayed a type 3 MNV. Furthermore, 49 of the MNVs (86%) were located in the macular area, whereas eight MNVs (14%) were located in the peripapillary area.
Analyzing the phenotype (presence of drusen, RPD, or both), almost all cases of subclinical AS (71/73 cases, 97%) were affected by RPD, in combination with drusen (29/71 cases, 41%) or without drusen (42/71 cases, 59%); the remaining two cases (3%) displayed only drusen without RPD. The distribution of RPD and drusen was significantly different in eyes with AMD and features of subclinical AS compared to eyes with AMD but without OCT features of subclinical AS (P < 0.001) (Table 1). In particular, the presence of RPD was significantly higher in patients with subclinical AS in eyes with AMD (Exp(B) = 2.589, P < 0.001).
Structural OCT Features of Subclinical AS
Based on their analysis of structural EDI-OCT scans, the two expert graders (RS and IZ) identified the presence of structural OCT features of AS. The agreement between the two readers was excellent (Cohen's κ: 0.91). All 73 eyes showed BM breaks and/or dehiscences and were diagnosed as subclinical AS in AMD. All 73 eyes also showed the concomitant presence of BM undulations. We did identify an additional 22 eyes in our cohort of 543 AMD eyes showing only BM undulations but without BM breaks and/or dehiscences; these 22 eyes were not included in the series of subclinical AS in AMD.
BM breaks were identified in 73 of 73 eyes (100%) (Figs. 3, 4, 5). In 47 of the 73 cases (64%), BM breaks were observed only in the macular area; in eight of 73 cases (11%) BM breaks were identified only in the peripapillary area; and in 18 of 73 cases (25%), BM breaks were identified in both the macular and peripapillary areas (Table 2). Analyzing the distribution of BM breaks among the different groups (eyes with MNV, eyes with GA, and eyes with intermediate AMD), there was no association between the location of breaks in the peripapillary area and AMD stage.
BM dehiscences were identified in 27 of 73 eyes (37%) (Fig. 2); of these 27 eyes, in 23 eyes (85%) BM dehiscences were observed only in the macular area, in three eyes (11%) BM dehiscences were observed only in the peripapillary area, and in only one eye (4%) were BM dehiscences observed in both the macular and peripapillary areas. Analyzing the presence and distribution of BM dehiscences among the different groups (eyes with MNV, eyes with GA, and eyes with intermediate AMD), BM dehiscences were not present in eyes with intermediate AMD, whereas they were more frequent in eyes with MNV (44% of cases) in comparison with eyes without MNV (Exp(B) = 5.469, P = 0.033) (Table 2).
Discussion
In this study, we report a specific phenotype of AMD with subclinical angioid streaks and describe associated demographic, clinical, and structural OCT features. Even though AS are not visible using fundus examination/photography (for this reason the name is “subclinical”), AMD patients with this phenotype displayed the OCT findings typically seen in eyes with AS [16, 22]. Another common feature between AS seen in patients with, for example, PXE and those with subclinical AS in AMD is the frequent involvement of the peripapillary area as the location of the BM alterations and atrophy development [23]. Indeed, peripapillary atrophy developed in 73% of subclinical AS in AMD cases in our series, and in > 50% in a previously reported series of AS secondary to PXE [24]. Interestingly, 36% of cases in our series showed a peculiar “petaloid-like” pattern of atrophy. This pattern was previously described by Marchese et al. [24] as a typical pattern of atrophy in AS patients secondary to PXE (affecting 34% of patients in that series). Finally, AS and subclinical AS in AMD showed a high prevalence of choroidal neovascularization (CNV) development. CNV is a well-known and frequent complication of AS, with a predominance of type 2 CNV [25]. In the present study, we found a similar rate of MNV prevalence (70%), with no predilection for the type of neovascularization. These above-mentioned aspects might suggest a partial common pathophysiological mechanism of onset, which could mainly be related more to BM alterations than to dysfunction of RPE and choriocapillaris. This assumption proposes BM pathology as the key factor for the development of RPE atrophy development and consequent choriocapillaris thinning and ingrowth of fibrous tissue through BM ruptures. The involvement of the BM with its conversion from an elastic structure to a calcified and brittle one is a well-known feature predisposing to developing AS. Due to its reduced elasticity, a brittle BM may be more vulnerable to mechanical stresses and thus to ruptures, even after physiological tension. This process is often located in the peripapillary area, which is a “locus minoris resistentiae” due to the interruption of BM in the papillary area. Due to the similar BM alterations and peripapillary involvement of subclinical AS in AMD, we suggest the predominant involvement of BM as a driving factor of this phenotype.
Interestingly, several differences characterize subclinical AS in AMD in comparison to AS. First, we excluded from our series all patients with systemic AS-related disease (e.g., PXE). Secondary, subclinical AS occurred in AMD patients who were older (mean ± SD: 82 ± 7 years in our series) than patients with conventional AS reported in a previous series (65.8 ± 13.9 years old) [22]. On the other hand, several features were shared between patients with subclinical AS and those with AMD. Even if patients with subclinical AS showed a higher prevalence of RPD (almost all cases), 42% of cases also showed drusen, the hallmark of AMD. Furthermore, our series did not provide significant differences in terms of median age between patients with the subclinical AS phenotype and other phenotypes of AMD (82 ± 7 years vs. 81 ± 8 years; P = 0.432). For these reasons, we speculate that subclinical AS could be the result of abnormal aging involving mainly the BM. In this scenario, this phenotype may represent an alternative form of chorioretinal aging with predominant involvement of BM, in contrast to supposed choriocapillaris loss (“vascular” hypothesis) or RPE cell death (“toxic” hypothesis) in AMD etiology [7, 26]. This speculation is supported mainly by the OCT findings and by the higher occurrence of RPD (97%) compared to drusen (42%) in these patients. To date, there is some evidence of lesions resembling RPD in PXE-associated AS, suggesting a possible role of the BM in the pathophysiology of RPD [5]. The frequency of RPD in patients with AMD is estimated to be approximately 30–50% depending on the phenotypes included in the analysis and the sensitivity of the imaging modalities used [4, 27]. Thus, the different ages at the onset of RPD in patients with AMD and AS might reflect a continuum of BM pathologic changes, with a minimal late-onset phenotype due to aging and pronounced early alterations associated with AS [5].
Due to the possible differences in the pathogenesis of subclinical AS and AMD, it can be speculated that subclinical age-related AS may be considered as a separate clinical entity. However, based on the common features between typical AMD and subclinical AS and the high prevalence of this phenotype in the AMD population (the estimated prevalence has been assessed at approximately 13.4% in our series), we propose that subclinical AS should be considered as a peculiar phenotype in the AMD spectrum. Interestingly, in an earlier study by Ellabban et al. [28], OCT undulations in patients with AMD were estimated to occur at a frequency similar to that of subclinical AS prevalence in our cohort of AMD patients. To explain this result, we could hypothesize that subclinical AS was misdiagnosed as “classic” AMD. In our case series, we excluded patients with only BM undulations because they did not show AS-related OCT findings (BM breaks and/or dehiscences). However, we did determine that 22 eyes in our AMD cohort had only BM undulations. This finding could represent a precursor of subclinical AS, as a sign of the first BM alteration. On the other hand, BM undulations may only be a sign of decreased elasticity of the BM-choroid complex associated with aging, as previously reported by Ugarte et al. [29]
It is possible to speculate that BM breaks are due to the passage of MNV from the choroidal circulation to the RPE/sub-RPE space; however, we reported BM breaks also in patients with intermediate AMD and in those with GA without MNV. Furthermore, also in eyes affected by neovascular AMD, the number of BM breaks was higher than those expected to be caused by the MNV passage through the BM.
Interestingly, patients with monoallelic ABCC6 mutations or with frequent hypomorphic variants in combination with a null variant in trans may show retinal changes overlapping certain phenotypic features of AMD (i.e., RPD, GA, and MNV), similar to the cohort in the present study with subclinical age-related AS [30, 31]. Hence, with an estimated carrier frequency in the general population of 1:30–1:200 [32], we can speculate that at least in some patients, the retinal disease is driven by increased soft tissue calcification due to ABCC6 dysfunction. Furthermore, some patients with hemochromatosis were previously reported with angioid-like streaks [33, 34]. For this reason, we cannot exclude the possibility that some of the patients in our series were affected by subclinical hemochromatosis.
We suggest that subclinical AS should be considered to be a different phenotype in the AMD population, particularly with respect to possible new therapies. Indeed, since BM likely plays a significant role in subclinical AS etiology, therapeutical approaches can be different from those for AMD. In particular, anti-complement treatments may not be as effective in this group of patients as in other drusen-driven “classic” AMD phenotypes. An important future target is to identify which structure is predominantly involved in chorioretinal aging, since this as yet unidentified structure could variably affect different anatomical sites.
The present study has several limitations, mainly due to the relatively small number of included eyes, its retrospective design, and the short interval of recruitment. However, our analysis is the first characterization of this novel age-related BM degeneration phenotype in the context of AMD. Of note, the prevalence of advanced stages of AMD (i.e., neovascular AMD and GA) could be overestimated in our population because our center is a tertiary referral center for macular diseases. Prospective studies with larger sample sizes are needed to reach more concrete conclusions and possibly gather more insights into their pathogenesis and progression. Furthermore, longitudinal studies are needed to understand if the response to the treatment in case of MNV is comparable to that of other phenotypes of AMD. Finally, dye angiographies (FA and ICGA) were not available for all included eyes; however, the absence of AS was based on fundus examination and different imaging analyses (multicolor, IR, and FAF) by two retinal experts.
Conclusions
In conclusion, we described the characteristics of subclinical AS in AMD by multimodal imaging approach, defining its prevalence in a cohort of AMD patients. We highlighted that patients with AS in AMD are characterized by different clinical presentation, imaging features, and pathogenesis, in comparison to eyes with AMD but without AS, and thus these eyes could represent a distinct group of the AMD population.
References
Chew EY, Clemons TE, Agrón E, et al. Ten-year follow-up of age-related macular degeneration in the age-related eye disease study: AREDS report no 36. JAMA Ophthalmol. 2014;132:272–7.
Ferris FL III, Wilkinson CP, Bird A, et al. Clinical classification of age-related macular degeneration. Ophthalmology. 2013;120:844–51.
Sacconi R, Vella G, Battista M, et al. Choroidal vascularity index in different cohorts of dry age-related macular degeneration. Transl Vis Sci Technol. 2021;10(12):26.
Rabiolo A, Sacconi R, Cicinelli MV, Querques L, Bandello F, Querques G. Spotlight on reticular pseudodrusen. Clin Ophthalmol. 2017;11:1707–18.
Gliem M, Hendig D, Finger RP, Holz FG, Charbel Issa P. Reticular pseudodrusen associated with a diseased Bruch membrane in pseudoxanthoma elasticum. JAMA Ophthalmol. 2015;133(5):581–8.
Gliem M, Müller PL, Mangold E, et al. Reticular pseudodrusen in Sorsby fundus dystrophy. Ophthalmology. 2015;122:1555–62.
Biesemeier A, Taubitz T, Julien S, Yoeruek E, Schraermeyer U. Choriocapillaris breakdown precedes retinal degeneration in age-related macular degeneration. Neurobiol Aging. 2014;35:2562–73.
McLeod DS, Grebe R, Bhutto I, et al. Relationship between RPE and choriocapillaris in age-related macular degeneration. Invest Ophthalmol Vis Sci. 2009;50:4982–91.
Friedman E. The pathogenesis of age-related macular degeneration. Am J Ophthalmol. 2008;146:348–9.
Corbelli E, Sacconi R, Rabiolo A, et al. Optical coherence tomography angiography in the evaluation of geographic atrophy area extension. Invest Ophthalmol Vis Sci. 2017;58:5201–8. [Erratum in Invest Ophthalmol Vis Sci. 2018;59(5):1801]
Hilely A, Au A, Freund KB, et al. Non-neovascular age-related macular degeneration with subretinal fluid. Br J Ophthalmol. 2021;105:1415–20.
Sacconi R, Corbelli E, Borrelli E, et al. Choriocapillaris flow impairment could predict the enlargement of geographic atrophy lesion. Br J Ophthalmol. 2021;105:97–102.
Kofler A. Beitrage zur Kenntnis der angioid Streaks. Arch Augenheilkd. 1917;82:134–49.
Dreyer R, Green WR. The pathology of angioid streaks: a study of twenty-one cases. Trans Pa Acad Ophthalmol Otolaryngol. 1978;31:158–67.
Jensen OA. Bruch’s membrane in pseudoxanthoma elasticum. Histochemical, ultrastructural, and x-ray microanalytical study of the membrane and angioid streak areas. Graefes Arch Clin Exp Ophthalmol. 1997;203:311–320.
Charbel Issa P, Finger RP, Holz FG, Scholl HP. Multimodal imaging including spectral domain OCT and confocal near infrared reflectance for characterization of outer retinal pathology in pseudoxanthoma elasticum. Invest Ophthalmol Vis Sci. 2009;50:5913–8.
Bergen AA, Plomp AS, Schuurman EJ, et al. Mutations in ABCC6 cause pseudoxanthoma elasticum. Nat Genet. 2000;25:228–31.
Jansen RS, Küçükosmanoglu A, de Haas M, et al. ABCC6 prevents ectopic mineralization seen in pseudoxanthoma elasticum by inducing cellular nucleotide release. Proc Natl Acad Sci USA. 2013;110:20206–11.
Kozák E, Bartstra JW, de Jong PA, et al. Plasma level of pyrophosphate is low in pseudoxanthoma elasticum owing to mutations in the ABCC6 gene, but it does not correlate with ABCC6 genotype. J Clin Med. 2023;12:1047.
Jampol LM, Acheson R, Eagle RC Jr, Serjeant G, O’Grady R. Calcification of Bruch’s membrane in angioid streaks with homozygous sickle cell disease. Arch Ophthalmol. 1987;105:93–8.
Kerr NM, Cassinelli HR, DiMeglio LA, et al. Ocular manifestations of juvenile Paget disease. Arch Ophthalmol. 2010;128:698–703.
Marchese A, Parravano M, Rabiolo A, et al. Optical coherence tomography analysis of evolution of Bruch’s membrane features in angioid streaks. Eye (Lond). 2017;31:1600–5.
Spaide RF, Jonas JB. Peripapillary atrophy with large dehiscences in bruch membrane in pseudoxanthoma elasticum. Retina. 2015;35:1507–10.
Marchese A, Rabiolo A, Corbelli E, et al. Ultra-widefield imaging in patients with angioid streaks secondary to pseudoxanthoma elasticum. Ophthalmol Retina. 2017;1:137–44.
Corbelli E, Carnevali A, Marchese A, et al. Optical coherence tomography angiography features of angioid streaks. Retina. 2018;38:2128–36.
Sacconi R, Corbelli E, Carnevali A, Querques L, Bandello F, Querques G. Optical coherence tomography angiography in geographic atrophy. Retina. 2018;38:2350–5.
Sacconi R, Corbelli E, Querques L, Bandello F, Querques G. A review of current and future management of geographic atrophy. Ophthalmol Ther. 2017;6:69–77.
Ellabban AA, Hangai M, Yamashiro K, Nakagawa S, Tsujikawa A, Yoshimura N. Tomographic fundus features in pseudoxanthoma elasticum: comparison with neovascular age-related macular degeneration in Japanese patients. Eye (Lond). 2012;26:1086–94.
Ugarte M, Hussain AA, Marshall J. An experimental study of the elastic properties of the human Bruch’s membrane-choroid complex: relevance to ageing. Br J Ophthalmol. 2006;90(5):621–926.
Charbel Issa P, Tysoe C, Caswell R. Late-onset pseudoxanthoma elasticum associated with a hypomorphic ABCC6 variant. Am J Ophthalmol. 2020;218:255–60.
Gliem M, Wieg I, Birtel J, Müller PL, Faust I, Hendig D, Holz FG, Finger RP, Charbel Issa P. Retinal findings in carriers of monoallelic ABCC6 mutations. Br J Ophthalmol. 2020;104(8):1089–92.
Charbel Issa P, Gliem M, Holz FG, et al. Pseudodominante Vererbung von pseudoxanthoma elasticum. Ophthalmologe. 2015;112:686–90.
Pulido JS, Donaldson MJ, Kitzmann AS, Skorin L Jr, Buettner H, Chen K. Angioid streaks in a patient with hemochromatosis and secondary porphyria cutanea tarda. Retin Cases Brief Rep. 2007;1:254–6.
Win PH, Pulido JS, Mahr MA. Choroidal neovascular membrane secondary to primary hemochromatosis. Retin Cases Brief Rep. 2007;1:147–8.
Acknowledgements
Author Contribution
Riccardo Sacconi, Francesco Bandello, Giuseppe Querques: concept and design. Riccardo Sacconi, Beatrice Tombolini, Ilaria Zucchiatti, Andrea Servillo, Matteo Menean, Giulio Falco Alessandrini, Lea Querques, Francesco Prascina, Peter Charbel Issa: drafting the manuscript. Riccardo Sacconi: statistical analysis. Beatrice Tombolini, Ilaria Zucchiatti, Andrea Servillo, Matteo Menean, Giulio Falco Alessandrini: collecting data.
Funding
This work was supported by the National Institute for Health Research (NIHR) Oxford Biomedical Research Centre (BRC), Oxford, UK. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health. The sponsor and funding organization had no role in the design or conduct of this research. No funding or sponsorship was received for the publication of this article.
Data Availability
The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request.
Ethical Approval
This retrospective study adhered to the 1964 Helsinki declaration and its later amendments. All subjects signed an informed consent at the time of examination for retrospective studies. Due to the retrospective nature of the study, the study does not require a specific Ethics Committee Approval according to Italian laws.
Conflict of Interest
Riccardo Sacconi is a consultant for: Allergan Inc (Irvine, California,USA), Bayer Shering-Pharma (Berlin, Germany), Carl Zeiss Meditec (Dublin, USA), Novartis (Basel, Switzerland). Beatrice Tombolini, Ilaria Zucchiatti, Andrea Servillo, Matteo Menean, Giulio Falco Alessandrini, Lea Querques, Francesco Prascina: none. Peter Charbel Issa has consulted for Gyroscope, ReVision, and Inozyme, has received research support from Heidelberg Engineering and travel support from Bayer. Francesco Bandello is a consultant for Alcon (Fort Worth,Texas,USA), Alimera Sciences (Alpharetta, Georgia, USA), Allergan Inc (Irvine, California,USA), Farmila-Thea (Clermont-Ferrand, France), Bayer Shering-Pharma (Berlin, Germany), Bausch And Lomb (Rochester, New York, USA), Genentech (San Francisco, California, USA), Hoffmann-La-Roche (Basel, Switzerland), NovagaliPharma (Évry, France), Novartis (Basel, Switzerland), Sanofi-Aventis (Paris, France), Thrombogenics (Heverlee,Belgium), Zeiss (Dublin, USA). Giuseppe Querques is a consultant for Alimera Sciences (Alpharetta, Georgia, USA), Allergan Inc (Irvine, California,USA), Amgen (Thousand Oaks, USA), Heidelberg (Germany), KBH (Chengdu, China), LEH Pharma (London, UK), Lumithera (Poulsbo, USA), Novartis (Basel, Switzerland), Bayer Shering-Pharma (Berlin, Germany), Sandoz (Berlin, Germany), Sifi (Catania, Italy), Soof-Fidia (Albano, Italy), Zeiss (Dublin, USA).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Sacconi, R., Tombolini, B., Zucchiatti, I. et al. Subclinical Angioid Streaks with Pseudodrusen: A New Phenotype of Age-Related Macular Degeneration. Ophthalmol Ther 12, 2729–2743 (2023). https://doi.org/10.1007/s40123-023-00778-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40123-023-00778-x