
Abstract
Introduction
This study evaluated efficacy and safety of implanting two second-generation trabecular micro-bypass stents (iStent inject/iStent inject W) with phacoemulsification, either with or without iAccess Precision Blade goniotomy, in patients with mild-to-moderate open-angle glaucoma (OAG).
Methods
This retrospective, non-randomized, unmasked, dual-arm, single-site, multi-surgeon, consecutive case series evaluated all OAG eyes that underwent phacoemulsification and iStent inject implantation either as a dual procedure (group A) or paired with iAccess goniotomy (group B) from July 2020 to May 2022. Effectiveness outcomes analyzed from 1 month onward included intraocular pressure (IOP), proportions of eyes with IOP ≤ 12/≤ 15/≤ 18, proportion medication-free, and medication number. Safety outcomes at all timepoints included adverse events and secondary surgeries.
Results
In group A, mean IOP reduced from 14.9 ± 3.2 mmHg on 1.22 ± 1.31 mean medications preoperatively (n = 63) to 13.5 ± 2.5 mmHg on 0.24 ± 0.61 medications at month 3 (n = 34; p = 0.048 IOP, p < 0.001 medications). In group B, mean IOP reduced from 16.0 ± 4.2 mmHg on 1.12 ± 1.07 medications preoperatively (n = 93) to 12.2 ± 2.3 mmHg on 0.57 ± 1.27 medications at month 3 (n = 23; p < 0.001 IOP, p = 0.003 medications). From preoperative to 3 months, the percent of eyes with IOP ≤ 12 mmHg remained at 32.4% in group A (p = 1.0) and rose from 21.7% to 60.9% in group B (p = 0.0177); eyes with IOP ≤ 15 mmHg rose from 52.9% to 76.5% in group A (p = 0.0963) and from 43.5% to 91.3% in group B (p = 0.0034). Adjusting for baseline between-group differences, group B had significantly greater postoperative IOP reduction than group A (p = 0.043); medication reductions were similar. Safety was favorable in both groups.
Conclusions
Phacoemulsification and iStent inject with or without iAccess Precision Blade goniotomy produced clinically meaningful and safe IOP and medication reductions. The paired iStent inject + iAccess + phacoemulsification procedure enabled greater IOP reduction and lower IOP thresholds than iStent inject + phacoemulsification. The study provides some of the first data on this paired approach and on the novel iAccess Precision Blade.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? |
Safe and efficacious surgical treatments are needed to prevent or minimize vision loss from glaucoma, a major cause of global blindness. |
This dual-arm real-world study assessed 3-month outcomes following implantation of iStent inject trabecular micro-bypass stents with phacoemulsification, either with or without concomitant iAccess Precision Blade goniotomy, in eyes with mild-to-moderate open-angle glaucoma. |
The study hypothesized that stent implantation with phacoemulsification could effectively and safely reduce intraocular pressure (IOP), and that adding goniotomy would provide additional IOP lowering. |
What was learned from the study? |
The data demonstrated significant IOP reductions and favorable safety through 3 months postoperative in both groups. However, pairing stent implantation with goniotomy appeared to allow more eyes to achieve lower thresholds of IOP than did stent implantation and phacoemulsification alone. |
The creation of additional outflow pathways via paired trabecular stenting and goniotomy may provide additional IOP-lowering benefit in patients with mild-to-moderate glaucoma. This study provides some of the first data to date on this paired approach and on the novel iAccess Precision Blade goniotomy device. |
Introduction
The treatment algorithm for glaucoma has shifted dramatically over the past decade. Instead of the former reliance on topical medications or filtration surgery (conservative and aggressive ends of the treatment spectrum, respectively), a new field of procedures, termed micro-invasive glaucoma surgery (MIGS), is now available to occupy this middle ground of therapy. In fact, a recent nationwide study of Medicare procedures showed that between 2011 and 2018, MIGS surgeries rose from constituting almost none of US glaucoma procedures to being the most frequently performed incisional glaucoma surgery; this coincided with a concomitant decline in higher-risk filtration surgeries such as trabeculectomy and tube shunt [1]. Among MIGS interventions, the iStent and iStent inject trabecular micro-bypass stents (Glaukos Corp., Aliso Viejo, CA, USA) have the largest and longest-term evidence base to date [2]. The totality of published data has shown these devices to be a safe and effective treatment option through up to 9 years of follow-up in patients with various severities and subtypes of glaucoma, and in both standalone and combined usage [3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24]. The clinical and preclinical evidence has also demonstrated that creating additional outflow pathways (for example, with multiple versus single stents) can enable additional improvements in IOP, medication, and/or outflow resistance [24,25,26,27,28].
Like all currently available glaucoma treatments, MIGS surgeries aim to reduce intraocular pressure (IOP), the most unequivocal risk factor for glaucoma incidence and progression [29,30,31]. The majority of MIGS surgeries reduce IOP by facilitating aqueous outflow, either through the conventional pathway (such as with iStent inject, Hydrus, goniotomy, ab interno canaloplasty) or the non-conventional pathway (such as with suprachoroidal procedures like CyPass, which is no longer on the market). Other procedures considered to be in the MIGS space reduce aqueous production by targeting the ciliary body (such as endoscopic cyclophotocoagulation or micropulse cyclophotocoagulation). Aqueous outflow resistance can be encountered throughout the continuum of the outflow system from diseased trabecular columns proximally through the obstructed and/or stenotic collector channels distally. To target multiple potential areas of outflow resistance, surgeons may combine procedures that act on different sites in the outflow pathway.
One such tailored dual intervention pairs trabecular bypass stenting with ab interno canaloplasty (ABiC) [32,33,34], acting at more proximal and distal parts of the outflow pathway, respectively. ABiC has been shown to provide meaningful initial reductions in IOP and number of medications [35,36,37]. Meanwhile, trabecular micro-bypass involves implanting a stent to provide an ongoing patent conduit through the trabecular meshwork, the site of greatest outflow resistance in patients with open-angle glaucoma (OAG), with durable IOP lowering demonstrated through up to 9 years of follow-up [4, 5, 23]. Regarding pairing the two procedures (canaloplasty with stenting), a 6-month study by Heersink et al. examined phacoemulsification and iStent trabecular micro-bypass with or without canaloplasty; the study showed possible IOP- and medication-reducing benefits from adding canaloplasty to phacoemulsification stent surgery [32]. These findings were corroborated by the 24-month results of Shultz et al. [33], which showed that the titrated use of iStent inject and phacoemulsification either with or without canaloplasty could reduce IOP and medications in eyes with greater or lesser medication burden, respectively.
There is also literature supporting the pairing of canaloplasty with trabeculotomy or goniotomy, which act at the level of the collector channels and the inner wall of Schlemm’s canal, respectively. One such study is the 12-month ROMEO study with the OMNI device [38], which demonstrated IOP- and medication-lowering effectiveness in eyes with both controlled and uncontrolled baseline IOP. Another study by Al Habash et al. combined gonioscopy-assisted transluminal trabeculotomy (GATT) and ABiC, and showed substantial IOP and medication reductions through 12 months postoperative [39].
To our knowledge, the present study is the first peer-reviewed publication examining iStent inject trabecular micro-bypass stenting either with or without ab interno goniotomy, both completed with phacoemulsification in a real-world US clinical population. This report is also the first scientific publication documenting early clinical outcomes of the newly introduced iAccess Precision Blade goniotomy device (Glaukos Corp., Aliso Viejo, CA, USA). The three-part phacoemulsification + iStent inject + goniotomy surgery, by targeting more trabecular sites in the conventional outflow pathway, allows surgeons to tailor treatments to patients’ individual pathophysiology.
Methods
Study Design and Participants
In this retrospective, dual-arm, nonrandomized, unmasked, consecutive study, all eyes that underwent phacoemulsification and iStent inject implantation either with or without adjuvant iAccess Precision Blade goniotomy between July 2020 and May 2022 were reviewed for potential inclusion. The majority of cases prior to November 2021 underwent iStent inject implantation with phacoemulsification (Group A), while most cases from November 2021 onward underwent iStent inject implantation with phacoemulsification and iAccess (Group B). All surgeries were performed by one lead surgeon (M.G.) at one US investigative site, in many cases with assistance of a fellow.
Inclusion criteria consisted of a diagnosis of OAG, cataract requiring surgery, no prior incisional glaucoma surgery, and normal anterior chamber angle anatomy. Exclusion criteria included closed angle glaucoma or non-glaucomatous ischemic retinal conditions and neuropathies. Ethics approval was obtained from the Surgical Center of El Paso Medical Executive Committee (El Paso, TX, USA), and the study was conducted according to the tenets of the Declaration of Helsinki and HIPPA privacy laws. All patients gave informed consent prior to undergoing surgery. A separate consent was not required for patients’ data to be analyzed given the retrospective anonymized nature of the study dataset.
Study Endpoints and Data Analysis
Examinations were completed before surgery and postoperatively at day 1, week 1, and months 1 and 3. Effectiveness endpoints were analyzed starting at month 1 and consisted of mean and percent reductions in IOP and medications; proportions of eyes with IOP ≤ 12, ≤ 15, and ≤ 18 mmHg; and proportions of eyes that were medication free. Safety data were analyzed at all timepoints and included intraoperative complications, postoperative adverse events, and secondary glaucoma surgery.
Comparisons of mean IOP and medications were analyzed with one-way repeated measure analysis of variance (ANOVA) followed by post hoc analysis with Bonferonni’s adjustment. Proportional outcomes were compared via the McNemar test for paired proportions in eyes that had data at both preoperative and 3-month time points. In addition, to account for preoperative differences between groups, a multilevel mixed effects model (linear model for IOP, Poisson model for medications) was used. The model compared mean IOP and medications of group A versus group B while accounting for both eyes per patient and longitudinal study design, with covariates of age, baseline IOP (categorical), and baseline medications (categorical). All study data were included in this model, while statistical comparison was calculated for month 3. A p-value < 0.05 was considered statistically significant in all analyses.
Study Devices and Surgical Implantation Techniques
iStent inject
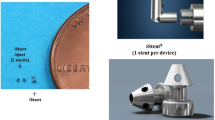
The iStent inject trabecular micro-bypass system and surgical procedure have been detailed previously [3]. Briefly, the injector is preloaded with two titanium stents, each of which allows multidirectional outflow through four side lumens and one central lumen. To complete implantation, the injector was placed through the phacoemulsification incision and advanced to the nasal trabecular meshwork, where the stents were placed approximately 2–3 clock hours apart through the meshwork into Schlemm’s canal. Stent position was then verified with intraoperative gonioscopy. Although micro-scale in size, each stent has been shown to fully handle the entire volume of aqueous humor production of the human eye [26]. The stents have also been proven capable of revitalizing previously dysfunctional outflow networks [40].
iAccess Precision Blade
In this study, group B underwent ab interno goniotomy with the iAccess Precision Blade (Fig. 1) in addition to phacoemulsification and iStent inject implantation. The Blade consisted of a 30-gauge titanium nitride-coated blade that was inserted through the clear corneal incision and used to create multiple channels (typically ~ 5) over a 90–100 degree area both within and outside the borders of the sites of iStent inject implantation. Each incision was a consistent, micro-scale 220 micron diameter, thereby preserving tissue and helping to maintain the pulsatile motion of the trabecular meshwork [41].

iAccess Precision Blade
After completion of either phacoemulsification + iStent inject (group A) or phacoemulsification + iStent inject + iAccess (group B), viscoelastic and residual blood were removed with irrigation/aspiration and wound sealing was confirmed. Patients were treated with a compounded topical mixture of prednisolone, nepafenac, and moxifloxacin four times a day for 1 week, then reduced to two times a day for an additional 2 weeks.
Results
Study Participants
The study enrolled 156 consecutive eyes of 108 patients with OAG who had undergone cataract extraction with iStent inject implantation either as a dual procedure (group A, n = 63) or a three-part procedure with adjuvant iAccess Precision Blade goniotomy (group B, n = 93). The groups had generally similar preoperative age, gender and ethnicity distribution, glaucoma type [vast majority primary OAG (POAG)], mean cup-to-disc ratio, baseline glaucoma severity [per Hodapp-Parrish-Anderson (HPA) criteria], and mean IOP and medication burden. Demographic and ocular parameters are supplied in Table 1.
Group A: Intraocular Pressure and Medications
Mean IOP for eyes in group A was 14.9 ± 3.2 (n = 63), 13.1 ± 2.5 (n = 49, p < 0.001), and 13.5 ± 2.5 (n = 34, p = 0.048) mmHg at baseline and 1 and 3 months postoperative, respectively (Fig. 2). Mean medication burden was 1.22 ± 1.31, 0.35 ± 0.83 (p < 0.001), and 0.24 ± 0.61 (p < 0.001) at baseline and 1 and 3 months postoperative, respectively (Fig. 3). At baseline, 32.4% of eyes had IOP ≤ 12 mmHg, 52.9% had IOP ≤ 15 mmHg, and 91.2% had IOP ≤ 18 mmHg. At 3 months postoperative, the proportions were 32.4% (p = 1.0), 76.5% (p = 0.0963), and 100% (p = 0.250) respectively (Fig. 4a). The proportion of eyes that were medication free also rose from 47.1% preoperatively to 85.3% at 3 months (p = 0.0002) (Fig. 4a).

Mean Intraocular Pressure at Baseline, 1 Month, and 3 Months; All Available Eyes at Each Time Point. Footnotes: group A underwent iStent inject implantation with phacoemulsification; group B underwent iStent inject implantation with phacoemulsification and iAccess Precision Blade goniotomy. Statistical analysis was based on one-way repeated measure ANOVA followed by post hoc analysis with Bonferroni’s adjustment.

Mean Number of Glaucoma Medications at Baseline, 1 Month, and 3 Months, All Available Eyes at Each Time Point. Footnotes: group A underwent iStent inject implantation with phacoemulsification; group B underwent iStent inject implantation with phacoemulsification and iAccess Precision Blade goniotomy. Statistical analysis was based on one-way repeated measure ANOVA followed by post hoc analysis with Bonferroni’s adjustment

a Baseline and 3-Month Proportional Analysis of IOP ≤ 12 mmHg, ≤ 15 mmHg, and ≤ 18 mmHg, and Eyes Medication Free, group A (n = 34 eyes with data at both time points). Footnotes: group A underwent iStent inject implantation with phacoemulsification; group B underwent iStent inject implantation with phacoemulsification and iAccess Precision Blade goniotomy. Statistical analysis was based on McNemar test for paired proportions, analyzing eyes that had both baseline and 3-month data. Hence, the sample size (n = 34) is smaller than the overall group A. b Baseline and 3-Month Proportional Analysis of IOP ≤ 12 mmHg, ≤ 15 mmHg, and ≤ 18 mmHg, and Eyes Medication Free, group B (n = 23 eyes with data at both time points). Footnotes: group A underwent iStent inject implantation with phacoemulsification; group B underwent iStent inject implantation with phacoemulsification and iAccess Precision Blade goniotomy. Statistical analysis was based on McNemar test for paired proportions, analyzing eyes that had both baseline and 3-month data. Hence, the sample size (n = 23) is smaller than the overall group B
Group B: Intraocular Pressure and Medications
Mean IOP for eyes in group B was 16.0 ± 4.2 (n = 93), 13.2 ± 3.2 (n = 65, p < 0.001), and 12.2 ± 2.3 (n = 23, p < 0.001) mmHg at baseline and 1 and 3 months, respectively (Fig. 2). Mean medication burden was 1.12 ± 1.07, 0.34 ± 0.92 (p < 0.001), and 0.57 ± 1.27 (p = 0.003) at baseline and 1 and 3 months, respectively (Fig. 3). At baseline, 21.7% of eyes had IOP ≤ 12 mmHg, 43.5% had IOP ≤ 15 mmHg, and 69.6% had IOP ≤ 18; this rose to 60.9% (p = 0.0177), 91.3% (p = 0.0034), and 100% (p = 0.0156) respectively at 3 months (Fig. 4b). The proportion of eyes that were medication free also rose from 52.2% preoperatively to 78.3% at 3 months (p = 0.0703) (Fig. 4b).
Intergroup Comparison: Intraocular Pressure and Medications
The postoperative performance of the two groups was compared using multilevel mixed effects models accounting for both eyes per patient and longitudinal study design, and with covariates of age, baseline IOP, and baseline medications. After this adjustment, the mean IOP reduction of group B was significantly greater than that of group A: specifically, there was 2.43 mmHg of additional IOP lowering with the addition of iAccess (p = 0.043)(Table 2). For medications, there was no statistical difference between groups in the amount of postoperative medication reduction (Table 2).
Safety
Safety was favorable in both groups. All eyes were successfully implanted with two trabecular stents; no intraoperative complications were noted. Postoperatively in group A, there were two cases of IOP elevation due to steroid response at week 1 (both eyes of the same patient; IOP 30 and 32 mmHg, respectively). These were managed with topical medication, and IOP reduced to 18 mmHg in both eyes at month 1. In group B, there was one case of 1 mm hyphema at day 1; this improved to microhyphema by week 1 and had resolved without intervention or sequelae by month 1. There was one case of corneal edema at day 1, which resolved without intervention or sequelae by week 1. No secondary surgeries nor persistent adverse events were reported in either group throughout the 3-month follow-up period.
Discussion
This real-world US cohort contributes some of the first data on the titrated use of iStent inject + phacoemulsification either with or without goniotomy. The three-part phacoemulsification + iStent inject + goniotomy surgery targets different trabecular sites in the conventional aqueous outflow pathway, allowing surgeons to tailor treatments to patients’ individual pathophysiology. This study also provides some of the first published data on the newly-introduced iAccess Precision Blade device used for goniotomy.
As the cornerstone of glaucoma treatment, IOP reduction is central in evaluating the efficacy of potential treatment interventions. In the current study, both groups experienced significant IOP reductions through 3 months postoperative. However, there was further treatment benefit from combining goniotomy with stent implantation. This suggests that combining both procedures may be synergistic in potentiating aqueous outflow, reaching lower levels of IOP than either procedure independently. Safety outcomes were similarly favorable in both groups in our study, consistent with the tissue-sparing ab interno nature of both stenting and goniotomy.
The results from the present study, specifically the added utility of performing goniotomy alongside trabecular stenting and phacoemulsification, confirm the findings of prior clinical reports evaluating single versus multiple stents. For example, a study by Katz et al. of one, two, or three stents [24], as well as an evaluation by Belovay et al. of two or three stents [25], both demonstrated that additional stents enabled further IOP reduction in an incremental manner. Their results were consistent with laboratory investigations of multiple iStent devices, which showed stepwise improvements in IOP and outflow resistance with additional stents [26,27,28]. For example, Hunter et al. reported 6 mmHg of IOP reduction and 30% decrease in outflow resistance after one stent, versus 8.9 mmHg and 44% decrease, respectively, after two stents [26]. Likewise, Bahler et al. estimated IOP reductions of 6.1 mmHg and 9.7 mmHg with one versus two stents, respectively [27, 28]. A potential explanation for this incremental IOP reduction lies in the biomechanical models of Johnstone et al., who showed aqueous tissue deformation induced by IOP gradients; if such tissue alteration were to decrease the action of a single trabecular stent, the use of multiple stents (or, as in the case of our cohort, the addition of goniotomy to trabecular stenting) hypothetically may circumvent this decrease [41]. Indeed, this hypothesis was consistent with our own results, which showed lower target pressures being reached in the group that underwent the combined stenting–goniotomy procedure.
In comparison with the existing literature on paired procedures, the most relevant prior report is the comparative study by Heersink et al. [32]. The study was a single-center, retrospective, 6-month analysis of 186 eyes that had undergone iStent implantation and phacoemulsification, either with (n = 86) or without (n = 100) canaloplasty using the Visco360 device. At 6 months postoperative, a higher proportion of eyes in the iStent-canaloplasty-phacoemulsification group achieved ≥ 20% IOP reduction and IOP < 18 mmHg on the same or fewer medications versus eyes in the iStent-phacoemulsification group. This suggests that performing an additional IOP-reducing procedure with a different mechanism of action may have further IOP- and/or medication-reducing benefits versus either individual procedure when performed with cataract surgery. Compared with the 6-month Heersink study, outcomes in our present study showed directionally similar between-group differences at 3 months. This again suggests a tangible benefit of completing goniotomy alongside phacoemsulsification–stent surgery, while longer-term follow-up will be needed to enable direct 6-month comparisons between the studies.
Key benefits of a surgical intervention, rather than topical medication, are myriad. They may include, for example, fewer medication side effects [42,43,44]; better quality of life [45,46,47]; higher patient adherence to treatment regimen [48,49,50]; lower risk of surgical failure in cases of future filtration surgery [51]; and reduced IOP variability [52, 53]. iStent implantation also has been proven to be cost-effective in over a dozen health economic studies in the USA and internationally [54,55,56,57,58].
This analysis was a retrospective real-world study, and as such was governed by realistic limitations of patient follow-up, treatment, and adherence. For example, there were no medication washouts, as these would not have been appropriate in real-world clinical practice. Additionally, since the dataset follows an ongoing real-world cohort, and since the Precision Blade technology was only recently introduced, not all patients had follow-up data at all time points, or there might be a delay in receiving records from comanaging optometrists. Patients were not randomized, so although the treatment groups were generally well matched in their preoperative parameters, we cannot exclude the possibility of non-quantifiable differences between them. The current dataset extends through 3 months of follow-up, and thus the results, although informative, should be seen as preliminary. A longer-term dataset will be necessary to further evaluate the performance of the paired procedure. Ongoing follow-up is being completed to that end.
Conclusions
The 3-month outcomes in the phacoemulsification–stent and phacoemulsification–stent–iAccess groups in this study indicate that both treatment options can produce clinically and statistically significant reductions in IOP and medications. However, there may be an additional benefit of completing ab interno goniotomy alongside stent implantation. By combining goniotomy and trabecular micro-bypass stenting, there is the potential to leverage two distinct and possibly synergistic MIGS interventions. The two procedures act upon different trabecular sites within the outflow system and have different expected durations of effect, with longer durations expected after trabecular bypass stents given that stents leave a patent conduit through the trabecular meshwork for aqueous egress. This cohort provides informative data on such a titrated intervention.
In addition, goniotomy in this study was completed with the recently introduced iAccess Precision Blade. Therefore, in addition to reporting novel outcomes of iStent inject with goniotomy, this study is the first scientific publication documenting early clinical outcomes of the new iAccess device. The findings support the practice of using MIGS surgeries in an incremental fashion, combining procedures that target different sites of trabecular outflow to effect greater IOP-reducing benefit.
References
Boland MV, Corcoran KJ, Lee AY (2021) Changes in performance of glaucoma surgeries 1994 through 2017 based on claims and payment data for United States Medicare Beneficiaries. Ophthalmol Glaucoma. Sep-Oct;4(5):463–471.
Businesswire.com Press Release August 23, 2021. Glaukos Announces Market-Leading Clinical Milestone of 200 Peer-Reviewed Publications on iStent Technologies. https://www.businesswire.com/news/home/20210823005049/en/Glaukos-Announces-Market-Leading-Clinical-Milestone-of-200-Peer-Reviewed-Publications-on-iStent%C2%AE-Technologies
Samuelson TW, Sarkisian SR Jr, Lubeck DM, Stiles MC, Duh Y-J, Romo EA, Giamporcaro JE, Hornbeak DM, Katz LJ. For the iStent inject study group, prospective, randomized, controlled pivotal trial of iStent inject trabecular micro-bypass in primary open-angle glaucoma and cataract: two-year results. Ophthalmology. 2019;126(6):811–21.
Hengerer FH, Auffarth GU, Conrad-Hengerer I. iStent inject Trabecular Micro-Bypass with or Without Cataract Surgery Yields Sustained 5-Year Glaucoma Control. Adv Ther. 2022;39(3):1417–31.
Salimi A, Watt H, Harasymowycz P. Long-term outcomes of two first-generation trabecular micro-bypass stents (iStent) with phacoemulsification in primary open-angle glaucoma: eight-year results. Eye Vis (Lond). 2021;8(1):43.
Ziaei H, Au L. Manchester iStent study: long-term 7-year outcomes. Eye (Lond). 2021;35(8):2277–82.
Paletta Guedes RA, Gravina DM, Paletta Guedes VM, Chaoubah A. Standalone implantation of 2–3 trabecular micro-bypass stents (iStent inject ± iStent) as an alternative to trabeculectomy for moderate-to-severe glaucoma. Ophthalmol Ther. 2022;11(1):271–92.
Healey PR, Clement CI, Kerr NM, Tilden D, Aghajanian L. Standalone iStent trabecular micro-bypass glaucoma surgery: a systemic review and meta-analysis. J Glaucoma. 2021;30(7):606–20.
Holmes DP, Clement CI, Nguyen V, Healey PR, Lim R, White A, Yuen J, Lawlor M. Comparative study of 2-year outcomes for Hydrus or iStent inject microinvasive glaucoma surgery implants with cataract surgery. Clin Exp Ophthalmol. 2022;50(3):303–11.
Ferguson TJ, Mechels KB, Dockter Z, et al. iStent trabecular microbypass stent implantation with phacoemulsification in patients with open-angle glaucoma: 6-year outcomes. Clin Ophthalmol. 2020;14:1859–66.
Ferguson T, Swan R, Ibach M, Schweitzer J, Sudhagoni R, Berdahl JP. Evaluation of a trabecular microbypass stent with cataract extraction in severe primary open-angle glaucoma. J Glaucoma. 2018;27(1):71–6.
Ferguson TJ, Ibach M, Schweitzer J, Karpuk K, Stephens JD, Sudhagoni R, Berdahl JP. Trabecular microbypass stent implantation in pseudophakic eyes with open-angle glaucoma: long-term results. J Cataract Refract Surg. 2019;45(4):414–20.
Salimi A, Watt H, Harasymowycz P. Three-year outcomes of second-generation trabecular micro-bypass stents (iStent inject) with phacoemulsification in various glaucoma subtypes and severities. J Glaucoma. 2021;30(3):266–75.
Ferguson TJ, Swan RJ, Bleeker A, et al. Trabecular microbypass stent implantation in pseudoexfoliative glaucoma: long-term results. J Cataract Refract Surg. 2020;46(9):1284–9.
Ferguson TJ, Ibach M, Schweitzer J, Karpuk KL, Stephens JD, Berdahl JP. Trabecular microbypass stent implantation with cataract extraction in pigmentary glaucoma. Clin Exp Ophthalmol. 2020;48(1):37–43.
Clement C, Howes F, Ioannidis A, Shiu M, Manning D, Lusthaus JA, Skalicky SE, Goodwin TW. Multicenter effectiveness and disease stability through 3 years after istent trabecular micro-bypass with phacoemulsification in glaucoma and ocular hypertension. Clin Ophthalmol. 2022;1(16):2955–68.
Guedes RAP, Gravina DM, Paletta Guedes VM, Chaoubah A. Two-year comparative outcomes of first- and second-generation trabecular micro-bypass stents with cataract surgery. Clin Ophthalmol. 2021;5(15):1861–73.
Neuhann R, Neuhann T. Second-generation trabecular micro-bypass stent implantation: retrospective analysis after 12- and 24-month follow-up. Eye Vis (Lond). 2020;10(7):1.
Salimi A, Abu-Nada M, Harasymowycz P. Matched cohort study of cataract surgery with and without trabecular micro-bypass stent implantation in primary angle-closure glaucoma. Am J Ophthalmol. 2021;224:310–20.
Salimi A, Clement C, Shiu M, Harasymowycz P. Second-generation trabecular micro-bypass (iStent inject) with cataract surgery in eyes with normal-tension glaucoma: one-year outcomes of a multi-centre study. Ophthalmol Ther. 2020;9(3):585–96.
Berdahl J, Voskanyan L, Myers JS, Katz LJ, Samuelson TW. iStent inject trabecular micro-bypass stents with topical prostaglandin as standalone treatment for open-angle glaucoma: 4-year outcomes. Clin Exp Ophthalmol. 2020;48(6):767–74.
Lindstrom R, Sarkisian SR, Lewis R, Hovanesian J, Voskanyan L. Four-year outcomes of two second-generation trabecular micro-bypass stents in patients with open-angle glaucoma on one medication. Clin Ophthalmol. 2020;14:71–80.
Dockter ZC, Ferguson TJ, Ibach MJ, Schweitzer JA, Berdahl JP. Trabecular micro-bypass stent implantation with cataract surgery in open-angle glaucoma: 9 year results. Podium presentation at the Annual Meeting of the American Society of Cataract and Refractive Surgery (ASCRS); April 22-26, 2022: Washington, DC, USA
Katz LJ, Erb C, Carceller Guillamet A, et al. Long-term titrated IOP control with one, two, or three trabecular micro-bypass stents in open-angle glaucoma subjects on topical hypotensive medication: 42-month outcomes. Clin Ophthalmol. 2018;31(12):255–62.
Belovay GW, Naqi A, Chan BJ, Rateb M, Ahmed II. Using multiple trabecular micro-bypass stents in cataract patients to treat open-angle glaucoma. J Cataract Refract Surg. 2012;38(11):1911–7.
Hunter K, Fjield T, Heitzmann H, Shandas R, Kahook M. Characterization of micro-invasive trabecular bypass stents by ex vivo perfusion and computational flow modeling. Clin Ophthalmol. 2014;8:499–506.
Bahler CK, Smedley GT, Zhou J, Johnson DH. Trabecular bypass stents decrease intraocular pressure in cultured human anterior segments. Am J Ophthal. 2004;138(6):988–94.
Bahler C, Hann C, Fjield T, Haffner D, Heitzmann H, Fautsch MP. Second-generation trabecular meshwork bypass stent (iStent inject) increases outflow facility in cultured human anterior segments. Am J Ophthal. 2012;153(6):1206–13.
Kass MA, Heuer DK, Higginbotham EJ, et al. The Ocular Hypertension Treatment Study: a randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma. Arch Ophthalmol 2002;120:701–13. discussion 829e30.
Leske MC, Heijl A, Hussein M, et al. Factors for glaucoma progression and the effect of treatment: the early manifest glaucoma trial. Arch Ophthalmol. 2003;121:48–56.
Lichter PR, Musch DC, Gillespie BW, Guire KE, Janz NK, Wren PA, Mills RP; CIGTS Study Group. Interim clinical outcomes in the Collaborative Initial Glaucoma Treatment Study comparing initial treatment randomized to medications or surgery. Ophthalmology. 2001 Nov;108(11):1943–53.
Heersink M, Dovich JA. Ab interno canaloplasty combined with trabecular bypass stenting in eyes with primary open-angle glaucoma. Clin Ophthalmol. 2019;13:1533–42.
Shultz M. 2nd-Generation trabecular micro-bypass +/- ab interno canaloplasty to potentiate aqueous outflow & reduce intraocular pressure in glaucoma. Podium presentation at the Annual Meeting of the American Society of Cataract and Refractive Surgery (ASCRS); April 22-26, 2022: Washington, DC, USA
Gallardo MJ. Outcomes of cataract surgery with Hydrus trabecular bypass and ab interno canaloplasty in open-angle glaucoma. Poster at the Annual Meeting of the American Glaucoma Society (AGS); March 3-6, 2022: Washington, DC, USA
Khaimi MA. Canaloplasty: a minimally invasive and maximally effective glaucoma treatment. J Ophthalmol. 2015;2015:485065. doi:https://doi.org/10.1155/2015/485065
Gallardo MJ. 24-Month efficacy of viscodilation of Schlemm’s canal and the distal outflow system with iTrack ab-interno canaloplasty for the treatment of primary open-angle glaucoma. Clin Ophthalmol. 2021;16(15):1591–9.
Hughes T, Traynor M. Clinical results of ab interno canaloplasty in patients with open-angle glaucoma. Clin Ophthalmol. 2020;29(14):3641–50.
Vold SD, Williamson BK, Hirsch L, Aminlari AE, Cho AS, Nelson C, Dickerson JE Jr. Canaloplasty and trabeculotomy with the OMNI system in pseudophakic patients with open-angle glaucoma: the ROMEO Study. Ophthalmol Glaucoma. 2021 Mar-Apr;4(2):173–181.
Al Habash A, Alrushoud M, Al Abdulsalam O, Al Somali AI, Aljindan M, Al Ahmadi AS. Combined gonioscopy-assisted transluminal trabeculotomy (GATT) with ab interno canaloplasty (ABiC) in conjunction with phacoemulsification: 12-month outcomes. Clin Ophthalmol. 2020;25(14):2491–6.
Huang AS, Penteado RC, Papoyan V, Voskanyan L, Weinreb RN. Aqueous angiographic outflow improvement after trabecular micro-bypass in glaucoma patients. Ophthalmol Glaucoma. 2019;2:11–21.
Li P, Shen TT, Johnstone M, Wang RK. Pulsatile motion of the trabecular meshwork in healthy human subjects quantified by phase-sensitive optical coherence tomography. Biomed Opt Express. 2013;4(10):2051–65.
Fechtner RD, Godfrey DG, Budenz D, Stewart JA, Stewart WC, Jasek MC. Prevalence of ocular surface complaints in patients with glaucoma using topical intraocular pressure-lowering medications. Cornea. 2010;29(6):618–21. https://doi.org/10.1097/ICO.0b013e3181c325b2.
Baudouin C, Labbé A, Liang H, Pauly A, Brignole-Baudouin F. Preservatives in eyedrops: the good, the bad and the ugly. Prog Retin Eye Res. 2010;29(4):312–34.
Skalicky SE, Goldberg I, McCluskey P. Ocular surface disease and quality of life in patients with glaucoma. Am J Ophthalmol. 2012;153:1-9.e2.
Samuelson TW, Singh IP, Williamson BK, Falvey H, Lee WC, Odom D, McSorley D, Katz LJ. Quality of life in primary open-angle glaucoma and cataract: an analysis of VFQ-25 and OSDI from the iStent inject® Pivotal Trial. Am J Ophthalmol. 2021 Mar 15:S0002–9394(21)00120–3. doi: https://doi.org/10.1016/j.ajo.2021.03.007. Epub ahead of print. PMID: 33737036.
Schweitzer JA, Hauser WH, Ibach M, et al. Prospective interventional cohort study of ocular surface disease changes in eyes after trabecular micro-bypass stent(s) implantation (iStent or iStent inject) with phacoemulsification. Ophthalmol Ther. 2020;9(4):941–53.
Al Habash A, Nagshbandi AA. Quality of life after combined cataract and minimally invasive glaucoma surgery in glaucoma patients. Clin Ophthalmol. 2020;14:3049–56.
Nordstrom BL, Friedman DS, Mozaffari E, Quigley HA, Walker AM. Persistence and adherence with topical glaucoma therapy. Am J Ophthalmol. 2005;140(4):598–606.
Newman-Casey PA, Robin AL, Blachley T, et al. The most common barriers to glaucoma medication adherence: a cross-sectional survey. Ophthalmology. 2015;122(7):1308–16.
Robin AL, Covert D. Does adjunctive glaucoma therapy affect adherence to the initial primary therapy? Ophthalmology. 2005;112:863–8.
Broadway D, Hitchings R, Grierson I. Topical antiglaucomatous therapy: adverse effects on the conjunctiva and implications for filtration surgery. J Glaucoma. 1995;4:136.
Posarelli C, Ortenzio P, Ferreras A, Toro MD, Passani A, Loiudice P, Oddone F, Casini G, Figus M. Twenty-four-hour contact lens sensor monitoring of aqueous humor dynamics in surgically or medically treated glaucoma patients. J Ophthalmol. 2019;27(2019):9890831. https://doi.org/10.1155/2019/9890831.eCollection2019.
Muniesa MJ, Ezpeleta J, Benítez I. Fluctuations of the intraocular pressure in medically versus surgically treated glaucoma patients by a contact lens sensor. Am J Ophthalmol. 2019;203:1–11.
Healey PR, Tilden D, Jackson D, Aghajanian L. A cost-utility analysis of trabecular bypass devices versus usual care for patients with open-angle glaucoma. Pharmacoecon Open. 2022;6(3):355–65.
Igarashi A, Ishida K, Shoji N, Chu A, Falvey H, Han R, Ueyama M, Onishi Y. iStent inject® and cataract surgery for mild-to-moderate primary open angle glaucoma in Japan: a cost-utility analysis. Int J Ophthalmol. 2022;15(6):954–61.
Patel V, Ahmed I, Podbielski D, Falvey H, Murray J, Goeree R. Cost-effectiveness analysis of standalone trabecular micro-bypass stents in patients with mild-to-moderate open-angle glaucoma in Canada. J Med Econ. 2019;22(4):390–401.
Nieland K, Labbé A, Schweitzer C, Gicquel G, Kleintjens J, Ostawal A, Treur M, Falvey H. A cost-effectiveness analysis of iStent inject combined with phacoemulsification cataract surgery in patients with mild-to-moderate open-angle glaucoma in France. PLoS One. 2021 Jun 10;16(6):e0252130. https://doi.org/10.1371/journal.pone.0252130.
Berdahl JP, Khatana AK, Katz LJ, Herndon L, Layton AJ, Yu TM, Bauer MJ, Cantor LB. Cost-comparison of two trabecular micro-bypass stents versus selective laser trabeculoplasty or medications only for intraocular pressure control for patients with open-angle glaucoma. J Med Econ. 2017;20(7):760–6.
Acknowledgements
Funding
The journal’s Rapid Service Fee and editorial assistance were provided by Glaukos Corporation (Aliso Viejo, California, USA). No funding was provided for the clinical work itself.
Editorial Assistance
Editorial assistance was provided by Dana M. Hornbeak, MD, MPH of Glaukos Corporation, and funded by Glaukos Corporation.
Authorship
All authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Author Contributions
Mark Gallardo: Concept and design, drafting the manuscript. Matthew Porter: Concept and design, drafting the manuscript.
Prior Publication
This manuscript is based on work that has been presented previously at the Annual Meeting of the American Glaucoma Society (AGS): March 2–5, 2023, Austin, TX.
Disclosures
Mark J. Gallardo: Glaukos: investigator, consultant, speaker, royalties, inventor of iAccess, Abbvie: Investigator, consultant, speaker. Sight Sciences: Investigator, consultant, speaker. Nova Eye: Investigator, consultant, speaker. Matthew Porter: Glaukos speaker.
Compliance with Ethics Guidelines
All procedures performed were in accordance with the ethical standards of the institutional and/or national research committee (the Institutional Review Board (IRB) of the University of Heidelberg), and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. All patients gave informed consent prior to undergoing surgery. A separate consent was not required for patients’ data to be analyzed given the retrospective anonymized nature of the study dataset.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Gallardo, M.J., Porter, M. Efficacy and Safety of Pairing iStent Inject Trabecular Micro-Bypass and iAccess Precision Blade Goniotomy in Patients with Open-Angle Glaucoma. Ophthalmol Ther 12, 1973–1987 (2023). https://doi.org/10.1007/s40123-023-00726-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40123-023-00726-9