
Abstract
Introduction
To assess differences in associations of ocular perfusion pressure (OPP) as well as retinal and retrobulbar blood flow between men and women with primary open angle glaucoma (OAG).
Methods
A total of 116 patients with OAG (age 66.9 ± 10.9 years, 70 females) participating in the Indianapolis Glaucoma Progression Study were assessed for OPP, retinal microcirculation, and retrobulbar blood flow. Confocal scanning laser Doppler flowmetry measured peripapillary retinal capillary blood flow. Color Doppler imaging measured peak systolic (PSV) and diastolic blood flow velocities and vascular resistance in the ophthalmic (OA), central retinal (CRA), and nasal and temporal short posterior ciliary arteries (N/T PCA). Bivariate Spearman correlation and multivariate linear regression analyses were performed.
Results
In female patients with OAG, inferior retinal capillary flow was associated with OPP (r = 0.246, P = 0.044). In men, superior and inferior sector retinal blood flow was associated with OPP (r = −0.402, P = 0.006 and r = −0.357, P = 0.016, respectively). There was no statistically significant association between OPP and retrobulbar blood vessel flow velocities in male patients with OAG but there was an association between OA and TPCA PSV and OPP in female patients with OAG (r = 0.290, P = 0.015 and r = 0.357, P = 0.002, respectively). In female patients with OAG, multivariate regression showed no statistically significant effect of any variable on the superior retinal capillary blood flow, with CRA PSV as a sole predictor to the inferior retinal sector (partial rho = 0.302, P = 0.015) and in male patients with OAG, superior sector retinal capillary blood flow was independently associated with intraocular pressure (partial rho = −0.371, P = 0.016) and OPP (partial rho = −0.456, P = 0.002) with a trend of association with OPP in the inferior retina (partial rho = −0.301, P = 0.053).
Conclusions
There was a positive linear association between retinal microcirculation and OPP in females and a negative association in males. Male and female patients with OAG may differ in their vascular autoregulation in response to changes in OPP.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Primary open angle glaucoma (OAG) is a multifactorial optic neuropathy characterized by progressive retinal ganglion cell death and visual field loss. Despite being a leading cause of impaired vision worldwide, the risk factors for OAG have not been fully defined. Some speculate that gender plays a role in OAG risk and pathogenesis and it is well established in the literature that there are physiologic and ocular differences between men and women that may explain a difference between the two with respect to glaucoma.
The difference in OAG predilection between men and women is conflicting in the current literature. A number of clinical trials show men to be disproportionately affected in OAG incidence, prevalence, and risk [1–6]. However, a few studies actually show women to be disproportionately affected, including the Arizona Eye Study [7, 8]. Further, a multitude of studies have found no difference in the rate of glaucoma between men and women, including the Baltimore Eye Survey, Beaver Dam Eye Study, and Blue Mountains Eye Study [9–13].
Not only has the incidence of OAG been noted to differ between the sexes in current literature, significant ocular structural disparities have also been noted. Women’s eyes are on average more than 1 mm shorter than men’s are. Average applanation tonometric readings are more than half a unit higher in women, and women’s lens and corneal curvatures have been found to be steeper than those in men are [14]. However, no relationship has yet to be established between these differences and glaucoma incidence or pathogenesis between the genders.
Another possible explanation for the potential differences in glaucoma predilection and pathogenesis between men and women is hormonal status. The relationship between estrogen status and glaucoma is well established in the literature. The Rotterdam Study found that women that were postmenopausal before the age of 45 were at higher risk of developing glaucoma than those who went through menopause after 45 years of age suggesting that estrogen might actually be protective against the development of glaucoma [15]. The Rotterdam study also found that men with a specific haplotype of an estrogen receptor beta (ESR2) had an increased incidence of glaucoma. While the function of this receptor is still unknown, this points towards hormonal status playing a role in glaucoma incidence [16]. Another study found that pregnancy, where estrogen levels are relatively elevated, actually impairs glaucoma progression [17]. Siesky et al. [18] determined that premenopausal women had lower intraocular pressure (IOP), the only known treatable risk factor for glaucoma, than postmenopausal women. Further, the Blue Mountains Eye Study found that women with later onset of menses and increased parity had an increased risk of OAG, possibly explained by decreased exposure to endogenous estrogens [19].
While evidence points to estrogen levels playing a role in the incidence of glaucoma, estrogen is also believed to affect ocular blood flow. Choroidal pulsatile ocular blood flow was found to be higher in premenopausal than postmenopausal women [20]. Studies looking at hormone replacement therapy (HRT) and ocular blood flow have determined that retrobulbar blood flow actually increases after instatement of HRT [21, 22]. There is conflicting evidence on the difference in retrobulbar blood flow between pre- and postmenopausal women. Altintas et al. [22] found higher retrobulbar flow in premenopausal compared to postmenopausal women. Siesky et al. [18], however, found no significant difference in retinal capillary and retrobulbar blood flow between pre- and postmenopausal women.
Over the past several decades, dozens of studies have linked abnormalities in ocular perfusion pressure (OPP) and blood flow to glaucomatous optic neuropathy. Specifically, blood flow deficiencies of the retinal, choroidal, and retrobulbar circulations have been reported in patients with OAG [23]. In large population-based trials, reduced OPP has been linked to both the prevalence and incidence of glaucoma [24–27].
Given the potential difference in prevalence of glaucoma between the sexes, the relationship between hormonal status and glaucoma, and the relationship between hormonal status and ocular blood flow, it is important to compare ocular blood flow in men and women. While studies have looked at effects of menopausal status and HRT on ocular blood flow, the literature is lacking in studies that directly compare ocular blood flow between the sexes. This is important to investigate considering the growing evidence linking changes in ocular blood flow and glaucoma [23–27].
The purpose of this study is to directly compare ocular blood flow in men and women by looking at OPP, retrobulbar blood flow, and retinal blood flow considering the larger picture of whether men and women differ in their glaucoma pathogenesis secondary to differences in ocular blood flow.
Methods
A pilot analysis using data from the Indianapolis Glaucoma Progression Study was performed. This investigation was conducted at the Glaucoma Research and Diagnostic Center in conjunction with the Department of Ophthalmology and Division of Biostatistics at the Indiana University School of Medicine. All experimental procedures conformed to the tenets of the Declaration of Helsinki and were approved by the institutional review board at the Indiana University School of Medicine and patients signed informed consent before enrollment. A total of 116 patients with OAG participating in the Indianapolis Glaucoma Progression Study were assessed for OPP, retinal microcirculation, and retrobulbar blood flow. Various baseline measurements were also taken to ensure continuity between the two groups with respect to systemic and ocular structural and functional parameters as outlined below.
Men and women were first assessed for baseline IOP and systemic blood pressure. Brachial artery blood pressure was assessed after a 5-min rest period using a calibrated automated sphygmomanometer. IOP was assessed using Goldmann applanation tonometry (Haag-Streit. Mason, OH, USA). OPP was calculated using systolic blood pressure and IOP with the following equation, OPP = 2/3 mean arterial pressure − IOP. Visual field was assessed using 24-2 standard automated perimetry (SITA) (Carl Zeiss Meditec, Inc. Dublin, CA, USA). Heidelberg Retinal Tomograph (Heidelberg Engineering, Carlsbad, CA 92008, USA), which uses a special laser to take three-dimensional photographs of the optic nerve and surrounding retina, was used to look at cup to disc ratio and retinal nerve fiber layer thickness. The instrument uses multiple two-dimensional images to construct a three-dimensional image of the entire optic nerve.
Color Doppler imaging (CDI) of the retrobulbar blood vessels was conducted using Philips HDI 5000 SonoCT Ultrasound System with the microvascular small parts clinical option (Philips Medical Systems, Bothell, WA, USA) with a 7.5 MHz linear probe as described in detail previously [13–16]. CDI measurements were taken in the ophthalmic (OA), central retinal (CRA), and nasal and temporal (NPCA/TPCA) short posterior ciliary arteries. In each vessel, peak systolic (PSV) and end diastolic (EDV) velocities were determined and Pourcelot’s vascular resistive index (RI) was calculated (RI = (PSV − EDV)/PSV). These techniques have been previously shown to yield reproducible measurements of retrobulbar blood flow velocities and peripheral vascular resistance [28–31].
Confocal scanning laser Doppler flowmetry (Heidelberg Retinal Flowmeter, Heidelberg Engineering, Heidelberg, Germany) was used to measure perfusion within peripapillary retinal capillary beds of the superior and inferior temporal fields. Flow was measured as number of zero flow pixels and number of pixels falling into the 10th, 25th, 50th, 75th, and 90th percentiles of total flow thereby describing the total vascularity of the fundus. The technique has been described in detail previously [32].
Statistical Analysis
Bivariate Spearman correlation and multivariate linear regression analysis were performed.
Results
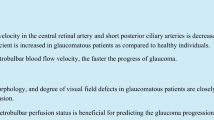
A total of 116 patients (age 66.9 ± 10.9 years, 70 women) with OAG participating in the Indianapolis Glaucoma Progression Study were assessed in female patients with OAG, the inferior retinal capillary flow was positively associated with OPP (r = 0.246, P = 0.044). In male patients with OAG, both superior and inferior sector retinal blood flow were negatively associated with OPP (r = –0.402, P = 0.006 and r = −0.357, P = 0.016, respectively) (Figs. 1, 2). There was no statistically significant association between OPP with the retrobulbar blood vessel flow velocities in male patients with OAG but there was an association between OA and TPCA PSV and OPP in female patients with OAG (r = 0.290, P = 0.015 and r = 0.357, P = 0.002, respectively); an effect that was independent of age in the multivariate analysis. In female patients with OAG, multivariate regression showed no statistically significant effect of any variable on the superior retinal capillary blood flow, with CRA PSV as a sole predictor to the inferior retinal sector (partial rho = 0.302, P = 0.015) and in male patients with OAG, superior sector retinal capillary blood flow was independently associated with IOP (partial rho = −0.371, P = 0.016) and OPP (partial rho = −0.456, P = 0.002) with a trend of association with OPP in the inferior retina (partial rho = −0.301, P = 0.053).

The relationship between inferior retinal mean blood flow and ocular perfusion pressure in female patients with glaucoma

The relationship between inferior retinal mean blood flow and ocular perfusion pressure in male patients with glaucoma
Table 1 contains data comparing measurements of IOP, systemic blood pressure, OPP as well as measurements of visual field as measured by 24–2 standard automated perimetry, including mean deviation and pattern standard deviation, and measurements of structure as measured by Heidelberg Retinal Tomograph, including cup to disc ratio and mean retinal nerve fiber layer thickness, in men and women in our pilot study. This table shows that men and women in our study did not greatly differ with regard to these measurements.
Discussion
In recent years, observational differences have been made between men and women with OAG. Conflicting evidence has been found as it relates to gender and OAG predilection with the majority pointing towards either men having increased predilection for glaucoma, or there being no difference between men and women. The Barbados Eye Study found the 9-year incidence of OAG was 4.9% in men and 4.1% in women [1]. Using published estimates from 25 studies and including 1,355 patients with OAG, Rudnicka et al. [6] found that the prevalence of OAG in men was 1.37 times greater than in women. Dielemans et al. [2] found that men had more than a 3 times greater risk of having OAG than women, with an odds ratio of 3.6. A number of other studies found a higher prevalence in men compared with women [3–5].
A multitude of studies, most notably including the Baltimore Eye Survey, Beaver Dam Eye Study, and Blue Mountains Eye Study have shown there to be no difference in OAG prevalence and incidence between men and women [9–13]. Few studies have found women to have an increased prevalence of OAG compared with men [7, 8]. Many theories exist as to why this difference in predilection may exist and that men and women have differences with respect to glaucoma.
Men and women have known structural differences [14] that could contribute to differences in OAG pathogenesis between the sexes. However, the more well established theory in the literature centers around hormonal status. The Rotterdam study has delved deeply into this issue and these researchers believe that estrogen may have a protective effect based upon their findings that women who went into menopause later had a decreased incidence of glaucoma and that men with the ESR2 haplotype had a 3.6-fold increased risk of OAG [15, 16]. Taken in conjunction with results of the present study, it is possible that ocular blood flow may play into this theory and ocular blood flow and hormonal status may be related as well as related differences in men and women with regards to OAG. Additionally, lower IOP, the only known treatable risk factor for glaucoma, was found in premenopausal women compared with postmenopausal women [18]. This too is interesting in conjunction with results of this study as the authors found no significant difference between men and women with regards to IOP, but we did in ocular blood flow. This supports the idea that ocular blood flow may be a separate risk factor for OAG differing between the sexes.
To further support the potential relationship between ocular blood flow, hormonal status, and glaucoma incidence, studies have shown that estrogen specifically affects ocular blood flow. Premenopausal women had a significantly higher rate of pulsatile ocular blood flow than post-menopausal women [20]. In looking at retrobulbar blood flow, it was found that pulsatility indices in the CRA declined after HRT was initiated [21]. Altintas et al. [22] also looked at HRT and retrobulbar blood flow and found that the RI in the CRA, TPCA, and NPCA had decreased after 2 months of HRT. In this same study, resistivity indices in the CRA, TPCA, and NPCA were higher in postmenopausal women than premenopausal women, also pointing to estrogen having a positive effect on ocular blood flow. The mechanism of this relationship is not well defined, however, and may be related to differences found in the present study between men and women with respect to ocular blood flow.
Furthermore, female menopausal status is known to have systemic vascular effects in women [18]. Estrogen has been shown to have a protective effect on coronary artery disease and vascular changes have been noted as early as 1-week postsurgical menopause in a group of women [33]. This supports the theory that ocular blood flow is related to the protective effects of estrogen against the development of glaucoma and that ocular blood flow could be related to the potential difference between men and women in glaucoma predilection and pathogenesis. However, to the authors’ knowledge, no studies had directly compared retinal and retrobulbar blood flow in men and women. Before the present study, such a relationship has only been speculated based on hormonal status’ effect on ocular blood flow.
This study supports the idea that men and women do differ with respect to ocular blood flow. Women had a positive relationship between retinal blood flow and OPP while men had a negative relationship between the two. Additionally, men had no relationship between retrobulbar blood flow and OPP, but in women there was a significant relationship between OA and TPCA PSV and OPP. When taken in conjunction with evidence of the relationship between ocular blood flow and glaucoma incidence and pathogenesis [23–27], the results of this study suggest a possible difference in vascular autoregulation between male and female patients with glaucoma during fluctuations of OPP. Autoregulation is defined as the intrinsic ability to maintain perfusion despite changes in the vasculature by vasodilation or constriction. It is theorized that autoregulation may be disrupted in patients with OAG, leading to ischemic damage to the optic nerve and retinal ganglion cells, and thus may play a role in OAG pathogenesis [34]. This study, however, was limited by the fact that the authors were not able to measure fluctuations in OPP thus this theory on differences in men and women with respect to autoregulation is merely speculative.
This study has several limitations in addition to the inability to measure fluctuations in OPP as noted above. The data were from a pilot analysis of data from the Indianapolis Glaucoma Progression Study and thus the authors looked at an uneven number of men and women, with women representing about 60% of the study patients. Additionally, hormonal status of the female patients was unknown and thus while speculation can be made upon the relationship between estrogen, ocular blood flow, and glaucoma, this study only provides information on ocular blood flow differing between the sexes. Finally, each imaging technology has inherit limitations; within this investigation CDI evaluated blood flow velocities and calculated vascular resistance but did not analyze direct flow assessments due to lack of blood vessel diameter [28–31].
This study suggests the possibility of a difference in pathogenesis between men and women in glaucoma secondary to differences in ocular blood flow, especially given the similarities between this study populations with regard to other measurements of glaucoma as evidenced in Table 1. Based on the current literature and theories, perhaps this difference is related to women’s increased exposure to estrogen and estrogen having a positive effect on autoregulation of ocular blood flow. Whether or not this difference in ocular blood flow is related to hormonal status and, ultimately, the incidence of glaucoma between men and women is yet to be determined. Further studies need to be conducted comparing men and women with respect to glaucoma incidence and progression and the relationship to hormonal status and ocular blood flow. This disparity in the relationship between retinal and retrobulbar blood flow and OPP in men compared with women supports the idea that men and women have ocular differences that may be contributory to differences in glaucoma between the two, especially considering the profound relationship in the literature between ocular blood flow and glaucoma incidence and progression [23–27]. Further studies also need to be done on how differences in ocular blood flow may contribute to glaucoma pathology as this may signal a different level of blood flow importance to the disease process in women compared with men with glaucoma.
Conclusion
This ultimately raises the larger question, of whether sex should be considered when patients with glaucoma are evaluated. Currently no approved management of glaucoma involves treatment of ocular blood flow, but growing evidence does point to a vascular consideration, especially given the larger number of patients who experience glaucoma progression despite significantly lowered IOP [35, 36]. More studies need to be done not only on the differences in pathogenesis of glaucoma between the sexes, but also on differences between the sexes regarding risk factors, including ocular circulation.
References
Leske MC, Wu SY, Honkanen R, Barbados Eye Studies Group, et al. Nine-year incidence of open-angle glaucoma in the Barbados Eye Studies. Ophthalmology. 2007;114:1058–64.
Dielemans I, Vingerling JR, Wolfs RC, et al. The prevalence of primary open-angle glaucoma in a population-based study in The Netherlands. The Rotterdam Study. Ophthalmology. 1994;101:1851–5.
Reidy A, Minassian DC, Vafidis G, et al. Prevalence of serious eye disease and visual impairment in a north London population: population based, cross sectional study. BMJ. 1998;316:1643–6.
Mukesh BN, McCarty CA, Rait JL, Taylor HR. Five-year incidence of open-angle glaucoma: the visual impairment project. Ophthalmology. 2002;109:1047–51.
Yoshida M, Okada E, Mizuki N, et al. Age-specific prevalence of open-angle glaucoma and its relationship to refraction among more than 60,000 asymptomatic Japanese subjects. J Clin Epidemiol. 2001;54:1151–8.
Rudnicka AR, Mt-Isa S, Owen CG, Cook DG, Ashby D. Variations in primary open-angle glaucoma prevalence by age, gender, and race: a Bayesian meta-analysis. Invest Ophthalmol Vis Sci. 2006;47:4254–61.
Quigley HA, Broman AT. The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol. 2006;90:262–7.
Higgenbotham EJ. Does sex matter in glaucoma? Arch Ophthalmol. 2004;122:374–5.
Tielsch JM, Sommer A, Katz J, et al. Racial variations in the prevalence of primary open-angle glaucoma. The Baltimore Eye Survey. JAMA. 1991;266:369–74.
Klein BE, Klein R, Sponsel WE, et al. Prevalence of glaucoma. The Beaver Dam Eye Study. Ophthalmology. 1992;99:1499–504.
Wensor MD, McCarty CA, Stanislavsky YL, Livingston PM, Taylor HR. The prevalence of glaucoma in the Melbourne Visual Impairment Project. Ophthalmology. 1998;105:733–9.
Varma R, Ying-Lai M, Francis BA, Los Angeles Latino Eye Study Group, et al. Prevalence of open-angle glaucoma and ocular hypertension in Latinos: the Los Angeles Latino Eye Study. Ophthalmology. 2004;111:1439–48.
Mitchell P, Smith W, Attebo K, et al. Prevalence of open-angle glaucoma in Australia. Ophthalmology. 1996;103:1661–9.
Mark HH. Gender differences in glaucoma and ocular hypertension. Arch Ophthalmol. 2005;123:284.
Hulsman CA, Westendorp ICD, Ramrattan RS, et al. Is open-angle glaucoma associated with early menopause? The Rotterdam Study. Am J Epidemiol. 2001;154:138–44.
de Voogd S, Wolfs RC, Jansonius NM, et al. Estrogen receptors alpha and beta and the risk of open-angle glaucoma: the Rotterdam Study. Arch Ophthalmol. 2008;126:110–4.
Phillps CI, Gore SM. Ocular hypotensive effect of late pregnancy with and without high blood pressure. Br J Ophthalmol. 1985;69:117–9.
Siesky BA, Harris A, Patel C, et al. Comparison of visual function and ocular hemodynamics between pre- and post-menopausal women. Eur J Ophthalmol. 2008;18:320–3.
Lee AJ, Mitchell P, Rochtchina E, Healey PR, Blue Mountains Eye Study. Female reproductive factors and open angle glaucoma: the Blue Mountains Eye Study. Br J Ophthalmol. 2003;87:1324–8.
Centofanti M, Bonini S, Manni G, et al. Do sex and hormonal status influence choroidal circulation? Br J Ophthalmol. 2000;84:786–7.
Atalay E, Karaali K, Akar M, et al. Early impact of hormone replacement therapy on vascular hemodynamics detected via ocular colour Doppler analysis. Maturitas. 2005;50:282–8.
Altintas O, Caglar Y, Yuksel N, Demirci A, Karabas L. The effects of menopause and hormone replacement therapy on quality and quantity of tear, intraocular pressure and ocular blood flow. Ophthalmologica. 2004;218:120–9.
Harris A, Kagemann L, Ehrlich R, et al. Measuring and interpreting ocular blood flow and metabolism in glaucoma. Can J Ophthalmol. 2008;43:328–36.
Tielsch JM, Katz J, Sommer A, Quigley HA, Javitt JC. Hypertension, perfusion pressure, and primary open-angle glaucoma. A population-based assessment. Arch Ophthalmol. 1995;113:216–21.
Quigley HA, West SK, Rodriguez J, et al. The prevalence of glaucoma in a population-based study of Hispanic subjects: Proyecto VER. Arch Ophthalmol. 2001;119:1819–26.
Bonomi L, Marchini G, Marraffa M, et al. Vascular risk factors for primary open angle glaucoma: the Egna-Neumarkt Study. Ophthalmology. 2000;107:1287–93.
Leske MC, Wu SY, Nemesure B, Hennis A. Incident open-angle glaucoma and blood pressure. Arch Ophthalmol. 2002;120:954–9.
Harris A, Sergott RC, Spaeth GL, et al. Color Doppler analysis of ocular vessel blood velocity in normal-tension glaucoma. Am J Ophthalmol. 1994;118:642–9.
Williamson TH, Harris A. Color Doppler ultrasound imaging of the eye and orbit. Surv Ophthalmol. 1996;40:255–67.
Harris A, Williamson TH, Martin B, et al. Test/retest reproducibility of color Doppler imaging assessment of blood flow velocity in orbital vessels. J Glaucoma. 1995;4:281–6.
Quaranta L, Harris A, Donato F, et al. Color Doppler imaging of ophthalmic artery blood flow velocity: a study of repeatability and agreement. Ophthalmology. 1997;104:653–8.
Kagemann L, Harris A, Chung HS, et al. Heidelberg retinal flowmetry: factors affecting blood flow measurement. Br J Ophthalmol. 1998;82:131–6.
Belchetz FK. Hormonal treatment of postmenopausal women. N Engl J Med. 1994;330:1062–71.
Moore D, Harris A, Wudunn D, Kheradiya N, Siesky B. Dysfunctional regulation of ocular blood flow: a risk factor for glaucoma? Clin Ophthalmol. 2008;2:849–61.
Heijl A, Leske MC, Bengtsson B, et al. Reduction of intraocular pressure and glaucoma progression: results from the Early Manifest Glaucoma Trial. Arch Ophthalmol. 2002;120:1268–79.
Collaborative Normal-Tension Glaucoma Study Group. Comparison of glaucomatous progression between untreated patients with normal-tension glaucoma and patients with therapeutically reduced intraocular pressure. Am J Ophthalmol. 1998;126:487–97.
Acknowledgments
An unrestricted grant was provided by Research to Prevent Blindness and Pfizer Pharmaceuticals, Inc. Results of this study were presented, in part, at the Association for Research in Vision and Ophthalmology Annual Meeting (ARVO): May 2011; Fort Lauderdale, Florida, USA.
Dr. Harris is the guarantor for this article, and takes responsibility for the integrity of the work as a whole.
Conflict of interest
No author had any commercial or other associations that might pose a conflict of interest in connection with submitted material. None of the authors have a proprietary interest in this publication. Alon Harris, MS, PhD, FARVO, serves as a consultant to Alcon, Allergan, Merck and Sucampo Pharmaceuticals but this does not pose a conflict of interest with the submitted material.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Additional information
ClinicalTrials.gov #NCT01145911.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 2.0 International License (https://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Tobe, L.A., Harris, A., Trinidad, J. et al. Should Men and Women be Managed Differently in Glaucoma?. Ophthalmol Ther 1, 1 (2012). https://doi.org/10.1007/s40123-012-0001-0
Received:
Published:
DOI: https://doi.org/10.1007/s40123-012-0001-0