
Abstract
Introduction
Candida auris (C. auris) is an emerging nosocomial pathogen, and a sharp rise in cases of colonization and infection has been registered in intensive care units (ICUs) during the ongoing coronavirus disease 2019 (COVID-19) pandemic. The unfavorable resistance profile of C. auris and the potential high mortality of C. auris infections represent an important challenge for physicians.
Methods
We conducted a single-center retrospective study including all patients admitted to ICUs with isolation of C. auris in any non-sterile body site between February 20, 2020, and May 31, 2021. The primary aim of the study was to assess the cumulative incidence of C. auris candidemia in colonized patients. The secondary aim was to identify predictors of C. auris candidemia in the study population.
Results
During the study period, 157 patients admitted to ICUs in our hospital became colonized with C. auris; 59% of them were affected by COVID-19. Overall, 27 patients (17%) developed C. auris candidemia. The cumulative risk of developing C. auris candidemia was > 25% at 60 days after first detection of C. auris colonization. Seven patients with C. auris candidemia (26%) also developed a late recurrent episode. All C. auris blood isolates during the first occurring episode were resistant to fluconazole and susceptible to echinocandins, while 15 (56%) were resistant to amphotericin B. During late recurrent episodes, emergent resistance to caspofungin and amphotericin B occurred in one case each. In the final multivariable model, only multisite colonization retained an independent association with the development of C. auris candidemia.
Conclusion
Candida auris candidemia may occur in up to one fourth of colonized critically ill patients, and multisite colonization is an independent risk factor for the development of candidemia. Implementing adequate infection control measures remains crucial to prevent colonization with C. auris and indirectly the subsequent development of infection.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Candida auris (C. auris) is an emergent pathogen causing nosocomial outbreaks at a global scale, especially in intensive care units. |
Identifying predictors of C. auris candidemia could improve early diagnosis and prognosis. |
In our cohort of critically ill colonized patients, the cumulative risk of developing C. auris candidemia exceeded 25% at 60 days after detection of colonization. |
High crude mortality was registered in episodes of late recurrent C. auris candidemia. |
Multisite C. auris colonization was associated with the development of C. auris candidemia in our population. |
Introduction
Candida auris is a yeast isolated for the first time in 2009 from the ear canal of a patient in Japan [1]. Since then, due to its persistence in the hospital environment and ease of transmission, it has caused numerous healthcare-associated outbreaks, described in six continents [2]. Recently, a sharp rise in new cases of colonization and infection has been reported, especially during the ongoing coronavirus disease 2019 (COVID-19) pandemic [3, 4]. These outbreaks involved mainly intensive care units (ICUs) [5].
One of the major challenges posed by C. auris is its unfavorable profile of resistance to antifungal agents, with > 90% of strains being resistant to fluconazole, 35% to amphotericin B, and over 40% expressing combined resistance to two or more classes of antifungals [6]. This characteristic may complicate the management of invasive C. auris infections such as candidemia, potentially contributing to high mortality [7, 8]. C. auris candidemia usually follows colonization; thus, understanding who among colonized patients is at higher risk of developing candidemia may help in improving early diagnosis, and also prevent invasive infection through interventions on modifiable predictors.
The aims of the present single-center study were to assess the cumulative incidence of C. auris candidemia and to identify predictors of C. auris candidemia in colonized patients admitted to the ICU.
Methods
Study Design and Setting
This is a retrospective, single-center study conducted at San Martino Policlinico Hospital, a 1200-bed teaching hospital in Genoa, Northern Italy, during the period from February 20, 2020, to May 31, 2021. All adult patients admitted to any ICU of our hospital and with isolation of C. auris from non-sterile body sites (skin, urine, and/or respiratory tract specimens) were included in the study. The study was approved by the Ethics Committee of the Liguria region (N. CER Liguria 31/2022).
Our hospital has five ICUs: (i) one with 12 beds dedicated to cardiovascular surgical patients; (ii) one with 10 beds dedicated to surgical and solid organ transplant patients; (iii) one with 10 beds dedicated to COVID-19 and respiratory patients; (iv) the largest one with 28 beds for neurosurgical and general ICU patients, which was in part converted to care for COVID-19 patients during the peak of cases in our region; (v) one with 8 beds in the emergency department, also caring for COVID-19 patients when needed for epidemiological reasons. During the whole study period, a dedicated team of infectious diseases specialists provided daily consultations in all the above-cited ICUs, to improve the management of infectious complications in critically ill patients.
Objectives
The primary objective of our study was to describe the cumulative incidence of C. auris candidemia among critically ill patients colonized by C. auris. The secondary objective was to assess independent predictors of C. auris candidemia in critically ill, colonized patients.
Definitions and Protocols
Colonization with C. auris was defined by the isolation of C. auris from at least one non-sterile site (urine, skin, and/or respiratory tract specimens), in the absence of clinical signs or symptoms of infection. Multisite colonization was defined as isolation of C. auris from more than one non-sterile site. Candidemia was defined by the isolation of C. auris from at least one blood culture. A late recurrent episode of C. auris candidemia was defined as new blood culture positivity after 30 days from the resolution of a previous episode [9]. Blood cultures were collected upon clinical suspicion of invasive infection from caring clinicians.
In order to contain C. auris dissemination in our hospital [10], an internal infection control protocol was implemented. It can be summarized as follows: (i) screening for skin colonization (combined axilla and groin skin swab) at admission to the ICU for early identification of possible community-acquired cases; (ii) repeated weekly screening for skin colonization during ICU admission until first detection of C. auris colonization; (iii) implementation of strict contact precautions for colonized patients; (iv) environmental intervention bundle to reduce the C. auris burden; (v) screening for skin colonization upon C. auris-negative patients’ discharge from the ICU and admission to a different ward, with preventive contact precautions pending culture results. Moreover, per center protocol, all patients admitted to the ICUs of our hospital during the study period underwent weekly culture of deep respiratory samples (whenever mechanically ventilated) and urine culture.
Microbiological Analysis
Candida auris was identified in clinical and screening specimens with matrix-assisted laser desorption ionization–time of flight mass spectrometry (MALDI-TOF MS—VITEK MS; bioMérieux, Marcy-l’Etoile, France) using VITEK MS v4.0 software. Antifungal susceptibility testing (AFST) was carried out according to the Clinical and Laboratory Standards Institute microdilution method using the Sensititre YeastOne panel (Thermo Scientific, Waltham, MA, USA); minimum inhibitory concentration (MIC) values were determined for azoles, echinocandins, and amphotericin B. Since no species-specific susceptibility breakpoints are currently available for C. auris, AFST results were interpreted according to the tentative breakpoints proposed by the US Centers for Disease Control and Prevention [11].
Data Collected for the Analysis
The following information was collected from electronic medical records as they were at the time of detection of C. auris colonization: age in years; gender; Charlson comorbidity index [12]; history of diabetes mellitus, chronic obstructive pulmonary disease (COPD), chronic kidney disease (defined as estimated glomerular filtration rate < 60 mL/min/1.73 m2), previous myocardial infarction, human immunodeficiency virus (HIV) infection, solid cancer, hematological malignancy, solid organ transplant (SOT), hematopoietic stem cell transplantation (HSCT); admission from long-term care facilities (LTCF); previous hospitalization (within 6 months); previous abdominal surgery (within 30 days); previous therapies (within 30 days) with antibiotics, antifungals (azoles and/or echinocandins and/or polyenes), steroids or other immunomodulatory agents; previous ICU stay in days before C. auris colonization; absolute neutrophil count (ANC) < 500 cell/mm3; infection by SARS-CoV-2 defined as a positive real-time polymerase chain reaction (RT-PCR) in at least one respiratory specimen; invasive mechanical ventilation; continuous renal replacement therapy (CRRT); extracorporeal membrane oxygenation (ECMO); total parenteral nutrition (TPN); presence of central venous catheter (CVC). Susceptibility test results for C. auris blood isolates and crude 30-day mortality after the first positive culture in candidemia episodes were also collected.
Statistical Analysis
No a priori sample size calculations were performed for this exploratory study. For the primary descriptive analysis, the cumulative risk of C. auris candidemia in colonized ICU patients was obtained by means of the Aalen–Johansen method, considering the first occurring C. auris candidemia as the event of interest, death as a competing event, and discharge from the ICU as a right-censoring event [13]. The time of origin was set at the day colonization by C. auris was first detected in the ICU (or equal to ICU admission in the case of already colonized patients), with the maximum length of follow-up being 60 days after the time of origin.
To describe the demographic and clinical characteristics of the study population, categorical variables were summarized with numbers and percentages, and continuous variables with median and interquartile range. The 95% confidence interval (CI) was calculated for both categorical and continuous estimates [14, 15]. For the secondary exploratory analysis of predictors of C. auris candidemia in colonized ICU patients, the possible association between demographic/clinical variables and the first occurring C. auris candidemia episode was first tested in univariable Cox regression models for providing unadjusted cause-specific hazard ratios (HR) with their 95% CI, after having verified proportionality of hazards with the Schoenfeld residuals-based test implemented in the R survival library. Then, variables potentially associated with the development of C. auris candidemia in univariable comparisons (p < 0.10) were included in an initial Cox regression multivariable model, and further selected for the final multivariable model through a stepwise backward procedure based on the Akaike information criterion, to provide adjusted cause-specific HR. Statistical analyses were performed using the R Statistical Software program (version 3.6.0, R Foundation for Statistical Computing, Vienna, Austria).
Results
During the study period, 157 patients admitted to the ICU of our hospital became colonized with C. auris. Seventy-one percent (n = 111) were male, with a median age of 64 years (interquartile range [IQR] 58–71). Patients with COVID-19 accounted for 59% of the study population (92/157). The complete demographic and clinical characteristics of the study population are reported in Table 1. All patients had a CVC (157/157, 100%), and the majority had received previous antibiotic therapy (152/157, 97%) and were mechanically ventilated (150/157, 96%).
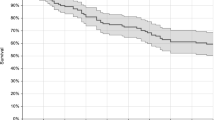
Overall, 27/157 (17%) patients developed at least one episode of C. auris candidemia, after a median of 29 days (IQR 15–38) from the first detection of colonization. The cumulative risk of developing at least one episode of C. auris candidemia exceeded 25% at 60 days after detection of colonization, as shown in Fig. 1. Among patients with candidemia, 7/27 (26%) developed late recurrent C. auris candidemia. AFST revealed that all isolates causing the first episode of candidemia were resistant to fluconazole (MIC50/MIC90: > 256 mg/L) and susceptible to echinocandins (MIC50: 0.12 mg/L; caspofungin/anidulafungin MIC90: 0.25 mg/L, micafungin MIC90: 0.12 mg/L), while 15/27 (56%) were resistant to amphotericin B (MIC50/MIC90: 2 mg/L). During late recurrent episodes, emergent resistance to caspofungin (MIC: 4 mg/L), despite retained susceptibility to other echinocandins, and amphotericin B (MIC: 2 mg/L) occurred in one case each (14% respectively). All patients received antifungal treatment with an echinocandin. A combination of anidulafungin and flucytosine was administered for treating the late recurrent episode caused by the isolate with caspofungin MIC 4 mg/L.

Cumulative risk of Candida auris candidemia in colonized ICU patients. The risk was estimated by means of the Aalen–Johansen method, with the first occurring C. auris candidemia as the event of interest, death as a competing event, and discharge from the ICU as a right-censoring event. BSI bloodstream infection, ICU intensive care unit
Overall, 30-day mortality after detection of C. auris colonization was 31% (48/157), while 30-day mortality after the onset of C. auris candidemia was 26% (7/27). Of note, four out of seven patients (57%) died within 30 days after the onset of late recurrent candidemia.
Table 2 shows the results of the univariable and multivariable analyses of factors potentially associated with the development of C. auris candidemia in colonized critically ill patients. At univariable analysis, CRRT, respiratory colonization, length of previous ICU stay, and multisite colonization showed an association with the development of C. auris candidemia. In the final multivariable model, only multisite colonization retained an independent association with the development of C. auris candidemia.
Discussion
In our study, we observed a 60-day cumulative incidence of C. auris candidemia > 25% among colonized critically ill patients. This risk seems apparently higher than those observed in two other large European cohorts of critically ill patients. C. auris candidemia developed in 18% of colonized patients over 3 years at the University and Polytechnic La Fe Hospital of Valencia [16], and also in 18% of patients with C. auris isolation in a cardiothoracic surgery center in London over a 16-month period [17]. However, these rates were not calculated through incidence curves accounting for censoring and competing events, whereas they are similar to the crude 17% prevalence of C. auris candidemia in our cohort, thereby suggesting a possibly similar risk across studies.
Notably, we also found a recurrence rate of 26% after the first episode. Recurrence of C. auris candidemia has been to date limited to case reports and this is the first report estimating the rate of recurrence after the first C. auris candidemia episode in colonized patients [18, 19].
The crude 30-day mortality rate in our study was 27%, which is coherent with the crude in-hospital mortality rate reported for C. auris candidemia (25–70%) [6, 20,21,22]. A recent meta-analysis estimated a crude mortality of 45% when restricting the analysis only to patients with candidemia, and suggested mortality to be possibly lower in the European continent [23]. We reported a far higher crude 30-day mortality in patients suffering from a second episode of C. auris candidemia (reaching almost 60%), although this may also reflect the severity of underlying noninfectious conditions in patients with prolonged ICU stay [9]. The high mortality we found after late recurrent episodes and its interpretation deserves further investigation in larger samples of patients with recurrent C. auris candidemia.
The high occurrence of antifungal resistance among clinical isolates of C. auris is of particular concern. In our cohort, all strains of C. auris causing candidemia were resistant to azoles and almost 60% were resistant to amphotericin B. None of the isolates showed baseline resistance to echinocandins, confirming that this class of antifungals frequently remains an effective option as first-line therapy for invasive C. auris infections. Nonetheless, our observation of a case of emergent resistance to caspofungin is alarming and should prompt further efforts not to jeopardize effective treatment options against this possibly multidrug-resistant yeast. In the latter case, however, AFST results should be carefully interpreted concerning caspofungin, since the concomitant susceptibility to other echinocandins might also suggest a paradoxically improved level of survival (a phenomenon commonly observed with echinocandins in Candida species) rather than emergent resistance.
All considered, there is a specific interest in preventing the occurrence of C. auris in colonized patients. In a cohort of 206 colonized critically ill patients, the presence of CVC and arterial catheter, total parenteral nutrition, diabetes mellitus, chronic kidney disease, CRRT, invasive mechanical ventilation, previous surgical intervention, multifocal colonization, and previous exposure to antifungals or antibiotics were independently associated with the development of C. auris candidemia [16]. Other published studies did not focus specifically on colonized patients and did not differentiate predictors of C. auris infections from those of colonization [21, 24, 25]. In our study, only multisite C. auris colonization (skin, respiratory, and/or urinary) retained a significant association with development of C. auris candidemia in colonized patients. Such a difference with previous reports might be attributed to the even distribution of some risk factors in our population (indwelling CVC, prior antibiotics exposure, mechanical ventilation). Moreover, differences in the baseline characteristics between our cohort and the Spanish one should be underlined [16]. Indeed, COVID-19 patients accounted for more than half of our colonized patients, while surgical patients were only a minority. The absence of association with “classical” risk factors of invasive candidiasis due to their wide distribution in our population (and likely in other ICU populations similar to ours) [26] should further stress the importance of preventing colonization as a crucial measure to indirectly curtail the overall impact of C. auris on mortality in critically ill patients.
The main limitation of our study is its retrospective design. Moreover, despite the fact that a quite large population of C. auris-colonized patients was included compared to current literature, power may still have remained suboptimal for some analyses (e.g., we found possible associations with the development of C. auris candidemia at borderline statistical significance for previous length of ICU stay and CRRT, deserving further investigation). Furthermore, the retrospective nature of the analysis precluded the collection of a sufficient amount of information to properly model potential predictors of candidemia such as days of CVC, days of antifungals, days of total parenteral nutrition, and invasive procedures as time-dependent covariates in Cox regression models. Finally, the rate of late recurrent C. auris candidemia might have been affected by the small denominator.
Conclusions
The cumulative incidence of C. auris candidemia in colonized critically ill patients may exceed 25% at 60 days. Multisite C. auris colonization is associated with the development of C. auris candidemia, suggesting that a higher fungal load may predispose to invasive infections. Our results support the importance of adequate infection control measures to prevent colonization with C. auris, thereby indirectly reducing the burden of morbidity and mortality associated with the development of C. auris candidemia.
References
Satoh K, Makimura K, Hasumi Y, Nishiyama Y, Uchida K, Yamaguchi H. Candida auris sp. nov., a novel ascomycetous yeast isolated from the external ear canal of an inpatient in a Japanese hospital. Microbiol Immunol. 2009;53(1):41–4.
Lone SA, Ahmad A. Candida auris—the growing menace to global health. Mycoses. 2019;62(8):620–37.
Chowdhary A, Sharma A. The lurking scourge of multidrug resistant Candida auris in times of COVID-19 pandemic. J Glob Antimicrob Resist. 2020;22:175–6.
Prestel C, Anderson E, Forsberg K, et al. Candida auris outbreak in a COVID-19 Specialty Care Unit-Florida, July–August 2020. MMWR Morb Mortal Wkly Rep. 2021;70(2):56–7.
Magnasco L, Mikulska M, Giacobbe DR, et al. Spread of carbapenem-resistant gram-negatives and Candida auris during the COVID-19 pandemic in critically ill patients: one step back in antimicrobial stewardship? Microorganisms. 2021;9(1):95.
Lockhart SR, Etienne KA, Vallabhaneni S, et al. Simultaneous emergence of multidrug-resistant Candida auris on 3 continents confirmed by whole-genome sequencing and epidemiological analyses. Clin Infect Dis. 2017;64(2):134–40.
Morales-López SE, Parra-Giraldo CM, Ceballos-Garzón A, et al. Invasive infections with multidrug-resistant yeast Candida auris, Colombia. Emerg Infect Dis. 2017;23(1):162–4.
Eyre DW, Sheppard AE, Madder H, et al. A Candida auris outbreak and its control in an intensive care setting. N Engl J Med. 2018;379(14):1322–31.
Muñoz P, Vena A, Valerio M, et al. Risk factors for late recurrent candidaemia. A retrospective matched case–control study. Clin Microbiol Infect. 2016;22(3):277.e11-20.
Di Pilato V, Codda G, Ball L, et al. Molecular epidemiological investigation of a nosocomial cluster of C. auris: evidence of recent emergence in Italy and ease of transmission during the COVID-19 pandemic. J Fungi (Basel, Switzerland). 2021;7(2):140.
Centre for Diseases Control and Prevention. Available online: https://www.cdc.gov/fungal/diseases/candidiasis/recommendations.html.
Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40:373–83.
Aalen OO, Johansen S. An empirical transition matrix for non-homogeneous Markov chains based on censored observations. Scand J Stat. 1978;5:141–50.
Pereira CA de B, Polpo A. MedOr: order of medians based on confidence statements. arXiv.org 2012. http://arxiv.org/abs/1212.5405.
Blaker H. Confidence curves and improved exact confidence intervals for discrete distributions. Can J Stat. 2000;28:783–98.
Garcia-Bustos V, Salavert M, Ruiz-Gaitán AC, Cabañero-Navalon MD, Sigona-Giangreco IA, Pemán J. A clinical predictive model of candidaemia by Candida auris in previously colonized critically ill patients. Clin Microbiol Infect. 2020;26(11):1507–13.
Schelenz S, Hagen F, Rhodes JL, et al. First hospital outbreak of the globally emerging Candida auris in European hospital. Antimicrob Resist Infect Control. 2016;5:35.
Biagi MJ, Wiederhold NP, Gibas C, Wickes BL, Lozano V, Bleasdale SC, et al. Development of high-level echinocandin resistance in a patient with recurrent Candida auris candidemia secondary to chronic candiduria. Open Forum Infect Dis. 2019;6(7):ofz262.
Mulet-Bayona JV, Salvador-García C, Tormo-Palop N, Gimeno-Cardona C. Recurrent candidemia and isolation of echinocandin-resistant Candida auris in a patient with a long-term central catheter. Enferm Infect Microbiol Clin (Engl Ed). 2021. https://doi.org/10.1016/j.eimc.2021.04.003.
Cortegiani A, Misseri G, Fasciana T, Giammanco A, Giarratano A, Chowdhary A. Epidemiology, clinical characteristics, resistance, and treatment of infections by Candida auris. J Intensive Care. 2018;6:69.
Shastri PS, Shankarnarayan SA, Oberoi J, Rudramurthy SM, Wattal C, Chakrabarti A. Candida auris candidaemia in an intensive care unit—prospective observational study to evaluate epidemiology, risk factors, and outcome. J Crit Care. 2020;57:42–8.
Mulet Bayona JV, Tormo Palop N, Salvador García C, et al. Characteristics and management of Candidaemia episodes in an established Candida auris outbreak. Antibiotics (Basel). 2020;9(9):558.
Chen J, Tian S, Han X, et al. Is the superbug fungus really so scary? A systematic review and meta-analysis of global epidemiology and mortality of Candida auris. BMC Infect Dis. 2020;20(1):827.
Ruiz-Gaitán A, Martínez H, Moret AM, et al. Detection and treatment of Candida auris in an outbreak situation: risk factors for developing colonization and candidemia by this new species in critically ill patients. Expert Rev Anti Infect Ther. 2019;17(4):295–305.
van Schalkwyk E, Mpembe RS, Thomas J, et al. Epidemiologic shift in candidemia driven by Candida auris, South Africa, 2016–2017. Emerg Infect Dis. 2019;25(9):1698–707.
León C, Ruiz-Santana S, Saavedra P, et al. A bedside scoring system (“Candida score”) for early antifungal treatment in nonneutropenic critically ill patients with Candida colonization. Crit Care Med. 2006;34(3):730–7.
Acknowledgements
We would like to thank all the colleagues working in the Infectious Diseases Unit and in all the Intensive Care Units for their daily dedication to the care of patients and their support during the conduction of the present study.
Funding
No funding or sponsorship was received for this study or publication of this article.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Author Contributions
Conceptualization and methodology: Federica Briano, Laura Magnasco and Daniele Roberto Giacobbe; formal analysis and investigation: Federica Briano, Laura Magnasco, Chiara Sepulcri, Silvia Dettori, Chiara Dentone, Lorenzo Ball, Chiara Robba, and Daniele Roberto Giacobbe; writing—original draft preparation, Federica Briano, Laura Magnasco and Daniele Roberto Giacobbe; writing—review and editing, Federica Briano, Laura Magnasco, Chiara Sepulcri, Chiara Dentone, Antonio Vena, Raffaele D’Angelo, Malgorzata Mikulska, Erika Coppo, Vincenzo Di Pilato, Anna Marchese, Angelo Gratarola, Matteo Bassetti, Paolo Pelosi, Lorenzo Ball, Chiara Robba, Nicolò Patroniti, Iole Brunetti, Antonio Vena, Silvia Dettori, Chiara Sepulcri, and Daniele Roberto Giacobbe; resources: Vincenzo Di Pilato, Erika Coppo, and Anna Marchese; supervision: Matteo Bassetti, Paolo Pelosi, Angelo Gratarola, Iole Brunetti, Nicolò Patroniti, and Malgorzata Mikulska.
Disclosures
Matteo Bassetti is an editorial board member for Infectious Diseases and Therapy. Outside the submitted work, Matteo Bassetti reports research grants and/or personal fees for advisor/consultant and/or speaker/chairman from Bayer, BioMérieux, Cidara, Cipla, Gilead, Menarini, MSD, Pfizer, and Shionogi. Daniele Roberto Giacobbe is an advisory board member for Infectious Diseases and Therapy. Outside the submitted work, Daniele Roberto Giacobbe reports investigator-initiated grants from Pfizer Inc and Gilead Italia. Outside the submitted work, Anna Marchese reports investigator-initiated grant from Gilead Italia. Outside the submitted work, Vincenzo Di Pilato reports research grant from Seegene Inc. The other authors have no conflicts of interests to disclose.
Compliance with Ethics Guidelines
The study was approved by the Ethics Committee of the Liguria region (N. CER Liguria 31/2022). Specific informed consent for this study was waived due to the retrospective nature of the analyses.
Data Availability
The data presented in this study are available upon scientifically sounded request from the corresponding author.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Briano, F., Magnasco, L., Sepulcri, C. et al. Candida auris Candidemia in Critically Ill, Colonized Patients: Cumulative Incidence and Risk Factors. Infect Dis Ther 11, 1149–1160 (2022). https://doi.org/10.1007/s40121-022-00625-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40121-022-00625-9