
Abstract
Purpose
This study compares the ability of two simpler severity rules (classical CRB65 vs. proposed CORB75) in predicting short-term mortality in elderly patients with community-acquired pneumonia (CAP).
Methods
A population-based study was undertaken involving 610 patients ≥65 years old with radiographically confirmed CAP diagnosed between 2008 and 2011 in Tarragona, Spain (350 cases in the derivation cohort, 260 cases in the validation cohort). Severity rules were calculated at the time of diagnosis, and 30-day mortality was considered as the dependent variable. The area under the receiver operating characteristic curves (AUC) was used to compare the discriminative power of the severity rules.
Results
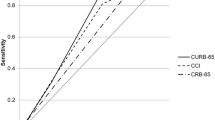
Eighty deaths (46 in the derivation and 34 in the validation cohorts) were observed, which gives a mortality rate of 13.1 % (15.6 % for hospitalized and 3.3 % for outpatient cases). After multivariable analyses, besides CRB (confusion, respiration rate ≥30/min, systolic blood pressure <90 mmHg or diastolic ≤60 mmHg), peripheral oxygen saturation (≤90 %) and age ≥75 years appeared to be associated with increasing 30-day mortality in the derivation cohort. The model showed adequate calibration for the derivation and validation cohorts. A modified CORB75 scoring system (similar to the classical CRB65, but adding oxygen saturation and increasing the age to 75 years) was constructed. The AUC statistics for predicting mortality in the derivation and validation cohorts were 0.79 and 0.82, respectively. In the derivation cohort, a CORB75 score ≥2 showed 78.3 % sensitivity and 65.5 % specificity for mortality (in the validation cohort, these were 82.4 and 71.7 %, respectively).
Conclusions
The proposed CORB75 scoring system has good discriminative power in predicting short-term mortality among elderly people with CAP, which supports its use for severity assessment of these patients in primary care.

Similar content being viewed by others


References
Woodhead M, Blasi F, Ewig S, et al.; Joint Taskforce of the European Respiratory Society and European Society for Clinical Microbiology and Infectious Diseases. Guidelines for the management of adult lower respiratory tract infections—full version. Clin Microbiol Infect. 2011;17:E1–59.
Mandell LA, Wunderink RG, Anzueto A, et al.; Infectious Diseases Society of America; American Thoracic Society. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44:S27–72.
Fine MJ, Auble TE, Yealy DM, et al. A prediction rule to identify low-risk patients with community-acquired pneumonia. N Engl J Med. 1997;336:243–50.
Lim WS, van der Eerden MM, Laing R, et al. Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study. Thorax. 2003;58:377–82.
McNally M, Curtain J, O’Brien KK, Dimitrov BD, Fahey T. Validity of British Thoracic Society guidance (the CRB-65 rule) for predicting the severity of pneumonia in general practice: systematic review and meta-analysis. Br J Gen Pract. 2010;60:e423–33.
Bont J, Hak E, Hoes AW, Macfarlane JT, Verheij TJ. Predicting death in elderly patients with community-acquired pneumonia: a prospective validation study reevaluating the CRB-65 severity assessment tool. Arch Intern Med. 2008;168:1465–8.
Ochoa-Gondar O, Vila-Corcoles A, Rodriguez-Blanco T, et al. Comparison of three predictive rules for assessing severity in elderly patients with CAP. Int J Clin Pract. 2011;65:1165–72.
Ewig S, Bauer T, Richter K, et al. Prediction of in-hospital death from community-acquired pneumonia by varying CRB-age groups. Eur Respir J. 2013;41:917–22.
Teramoto S, Yamamoto H, Yamaguchi Y, et al. Lower respiratory tract infection outcomes are predicted better by an age >80 years than by CURB-65. Eur Respir J. 2008;31:477–8.
Parsonage M, Nathwani D, Davey P, Barlow G. Evaluation of the performance of CURB-65 with increasing age. Clin Microbiol Infect. 2009;15:858–64.
Dwyer R, Hedlund J, Darenberg J, et al. Improvement of CRB-65 as a prognostic scoring system in adult patients with bacteraemic pneumococcal pneumonia. Scand J Infect Dis. 2011;43:448–55.
Buising KL, Thursky KA, Black JF, et al. Identifying severe community-acquired pneumonia in the emergency department: a simple clinical prediction tool. Emerg Med Australas. 2007;19:418–26.
British Thoracic Society, Myint PK, Kamath AV, Vowler SL, Maisey DN, Harrison BD. Severity assessment criteria recommended by the British Thoracic Society (BTS) for community-acquired pneumonia (CAP) and older patients. Should SOAR (systolic blood pressure, oxygenation, age and respiratory rate) criteria be used in older people? A compilation study of two prospective cohorts. Age Ageing. 2006;35:286–91.
Royston P, Moons KG, Altman DG, Vergouwe Y. Prognosis and prognostic research: developing a prognostic model. BMJ. 2009;338:b604.
Altman DG, Vergouwe Y, Royston P, Moons KG. Prognosis and prognostic research: validating a prognostic model. BMJ. 2009;338:b605.
Altman DG, Royston P. What do we mean by validating a prognostic model? Stat Med. 2000;19:453–73.
Chen JH, Chang SS, Liu JJ, et al. Comparison of clinical characteristics and performance of pneumonia severity score and CURB-65 among younger adults, elderly and very old subjects. Thorax. 2010;65:971–7.
Shindo Y, Sato S, Maruyama E, et al. Comparison of severity scoring systems A-DROP and CURB-65 for community-acquired pneumonia. Respirology. 2008;13:731–5.
Charles PG, Wolfe R, Whitby M, et al. SMART-COP: a tool for predicting the need for intensive respiratory or vasopressor support in community-acquired pneumonia. Clin Infect Dis. 2008;47:375–84.
Bewick T, Greenwood S, Lim WS. What is the role of pulse oximetry in the assessment of patients with community-acquired pneumonia in primary care? Prim Care Respir J. 2010;19:378–82.
Majumdar SR, Eurich DT, Gamble JM, Senthilselvan A, Marrie TJ. Oxygen saturations less than 92% are associated with major adverse events in outpatients with pneumonia: a population-based cohort study. Clin Infect Dis. 2011;52:325–31.
Acknowledgments
The authors would like to thank all the physicians and nurses of the primary care centers of Tarragona-Valls, Joan XXIII Hospital, and Santa Tecla Hospital who collaborated in this study. Thanks go to Angel Vila Rovira for his help in collecting the mortality data. Thanks also go to Timothy Bowring for his help in the production of this paper.
This study was supported by a grant from the Instituto de Salud Carlos III from the Spanish Health Ministry (Grant ID FIS PI-09/90484).
Conflict of interest
All authors, none declared.
Author information
Authors and Affiliations
Consortia
Corresponding author
Rights and permissions
About this article
Cite this article
Ochoa-Gondar, O., Vila-Corcoles, A., Rodriguez-Blanco, T. et al. Validation of the CORB75 (confusion, oxygen saturation, respiratory rate, blood pressure, and age ≥75 years) as a simpler pneumonia severity rule. Infection 42, 371–378 (2014). https://doi.org/10.1007/s15010-013-0565-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s15010-013-0565-1